Subscribe for E-mail Alerts
Subscribe for E-mail Alerts CCDC Weekly RSS Feed
CCDC Weekly RSS Feed2023 Vol. 5, No. 7
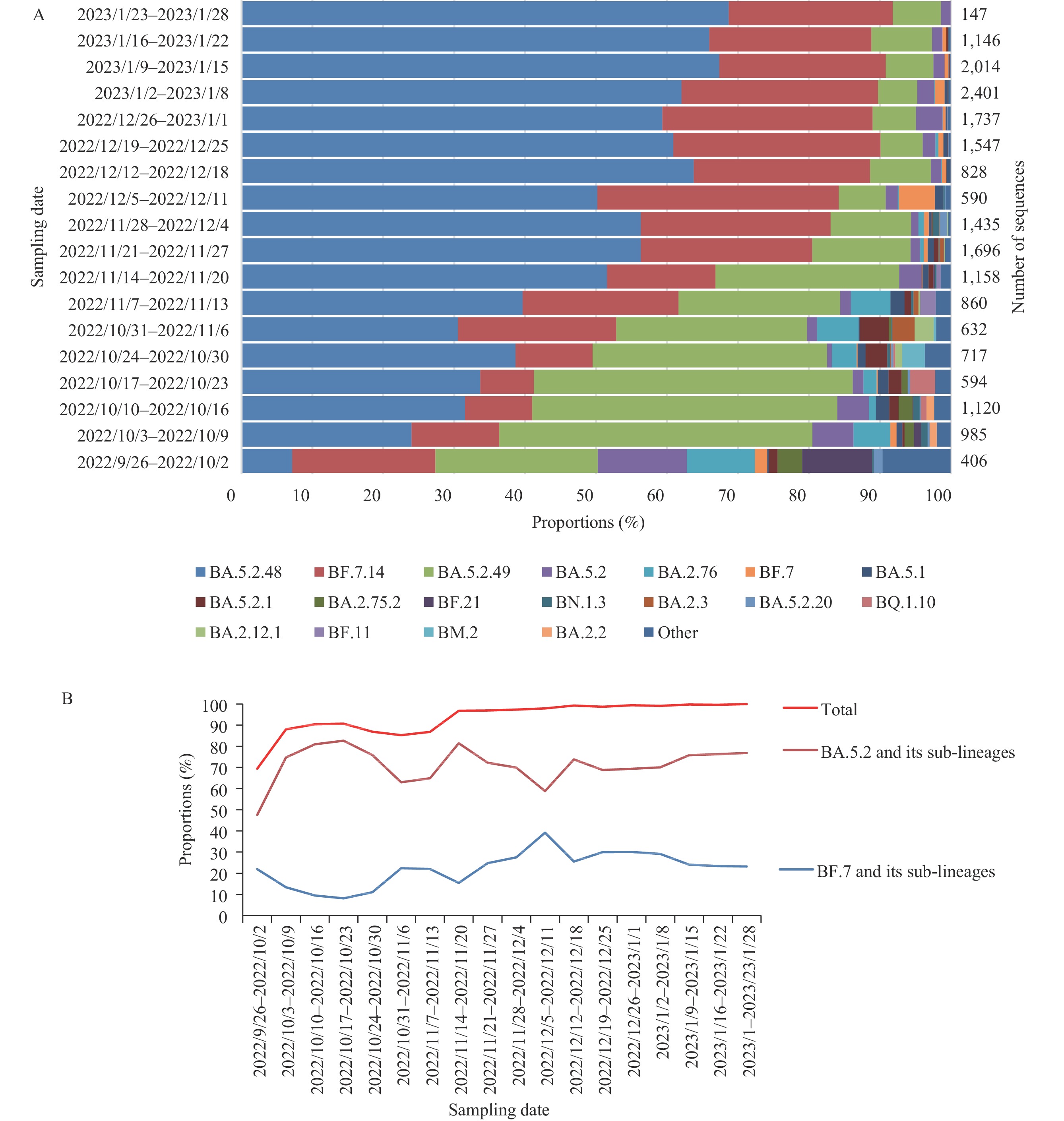
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has generated 2,431 variants over the course of its global transmission over the past 3 years. To better evaluate the genomic variation of SARS-CoV-2 before and after the optimization of coronavirus disease 2019 (COVID-19) prevention and control strategies, we analyzed the genetic evolution branch composition and genomic variation of SARS-CoV-2 in both domestic and imported cases in China (the data from Hong Kong and Macau Special Administrative Regions and Taiwan, China were not included) from September 26, 2022 to January 29, 2023.
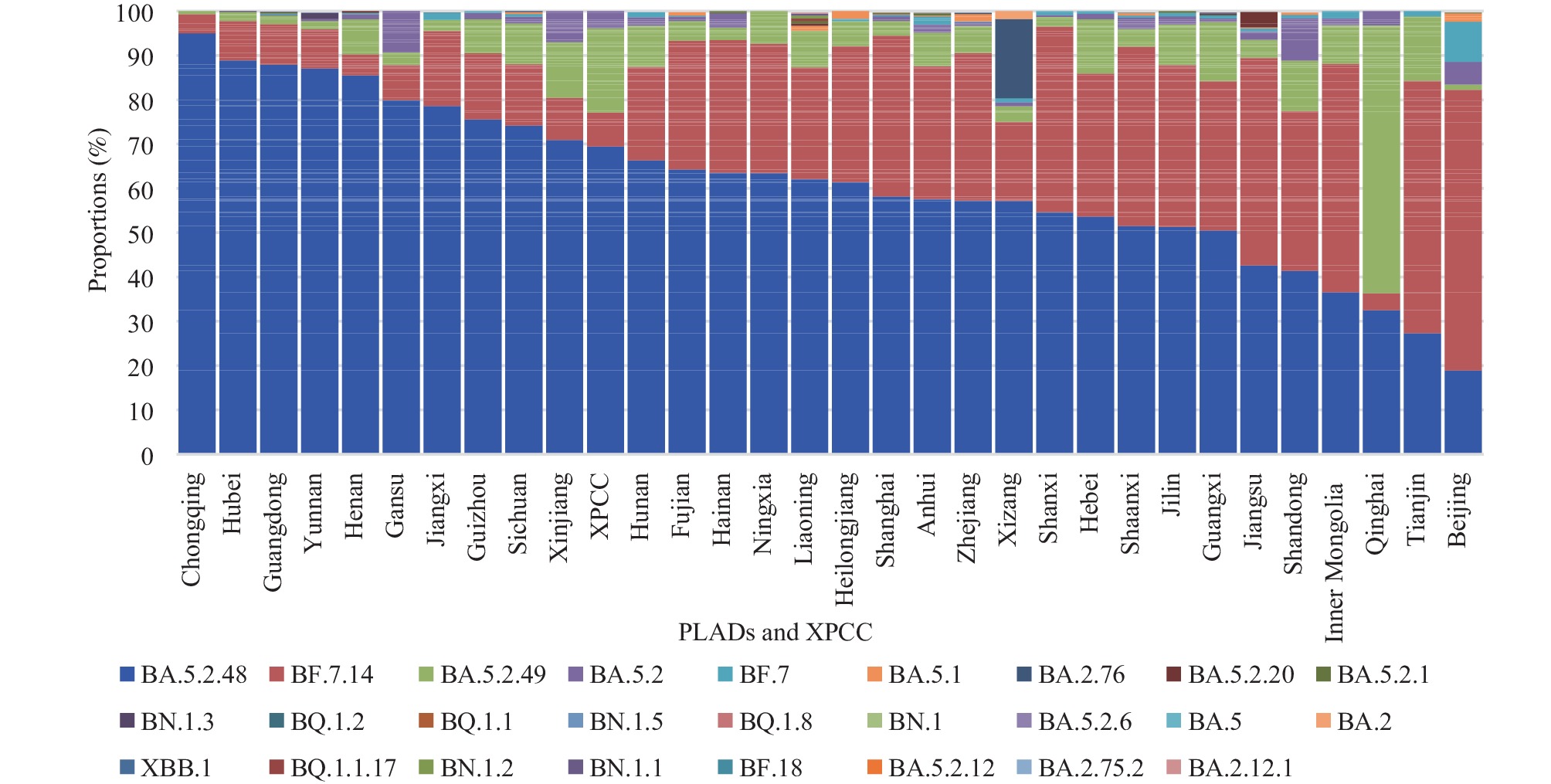
Analysis of the number of genome sequences, sampling time, dynamic changes of evolutionary branches, origin, and clinical typing of SARS-CoV-2 variants submitted by 31 provincial-level administrative divisions (PLADs) and Xinjiang Production and Construction Corps (XPCC) was conducted to assess the accuracy and timeliness of SARS-CoV-2 variant surveillance.
From September 26, 2022 to January 29, 2023, 20,013 valid genome sequences of domestic cases were reported in China, with 72 evolutionary branches. Additionally, 1,978 valid genome sequences of imported cases were reported, with 169 evolutionary branches. The prevalence of the Omicron variants of SARS-CoV-2 in both domestic and imported cases was consistent with that of international epidemic variants.
This study provides an overview of the prevalence of Omicron variants of SARS-CoV-2 in China. After optimizing COVID-19 prevention and control strategies, no novel Omicron variants of SARS-CoV-2 with altered biological characteristics or public health significance have been identified since December 1, 2022.


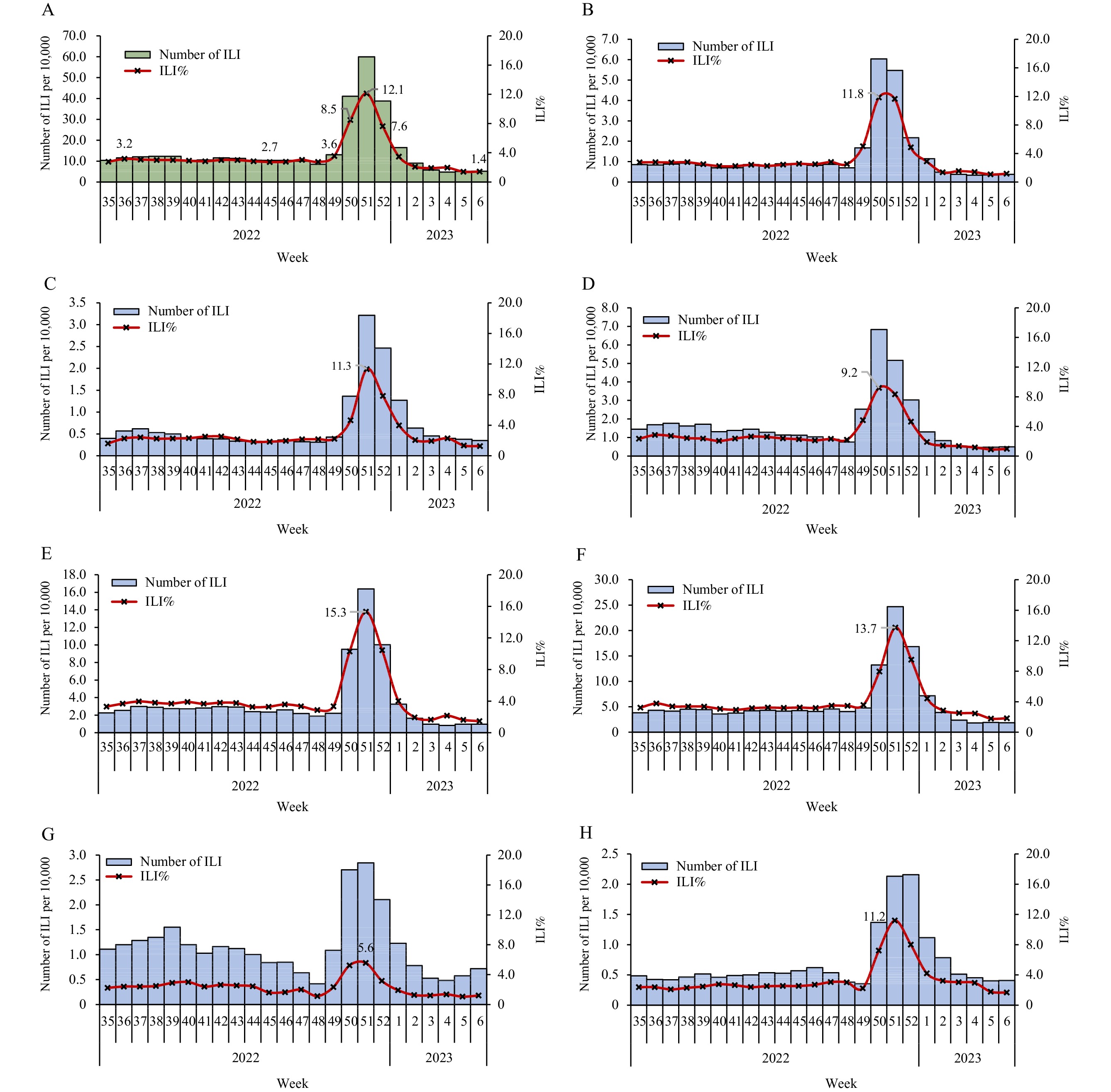
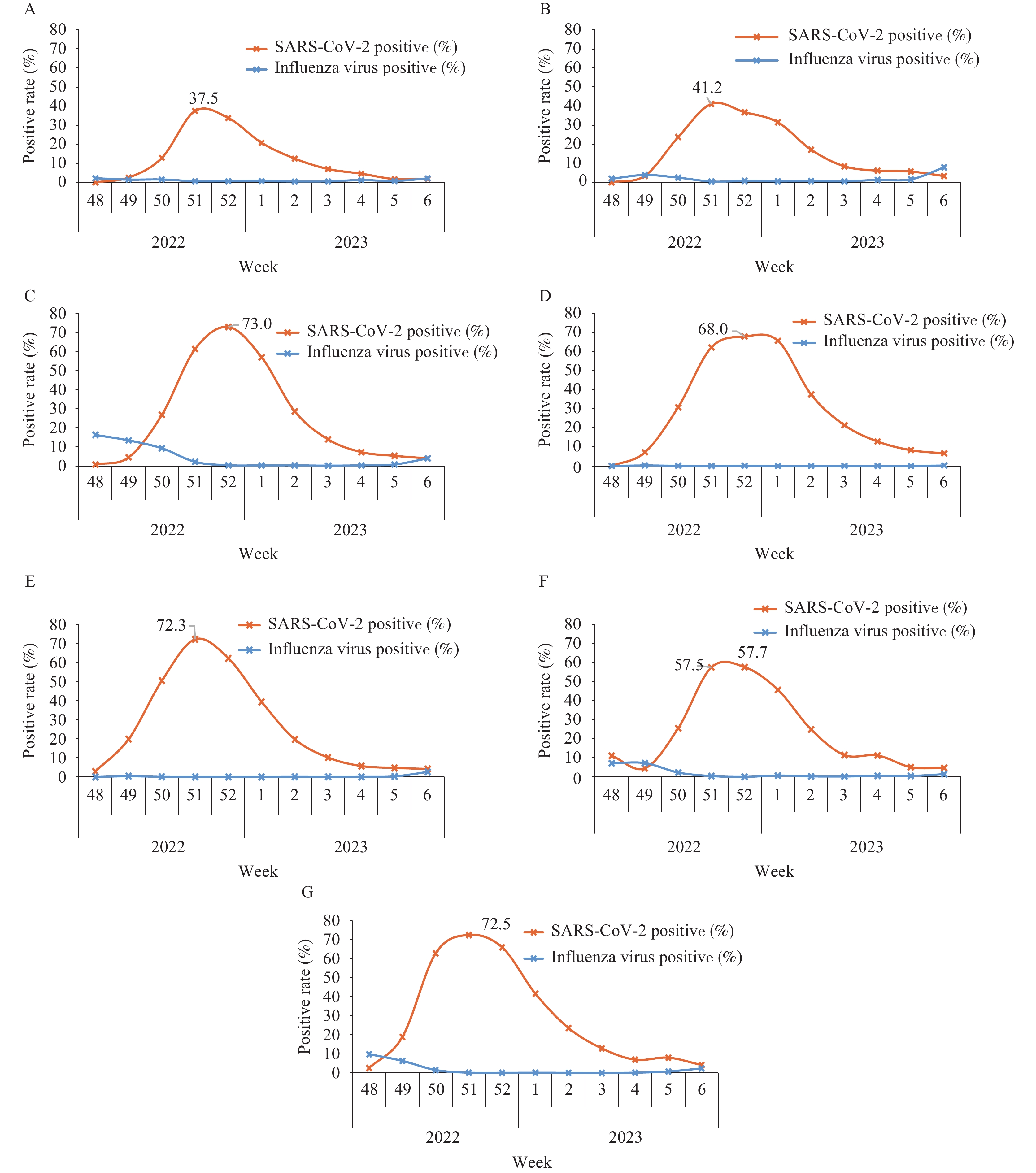
The World Health Organization (WHO) proposed using influenza surveillance systems to carry out coronavirus disease 2019 (COVID-19) surveillance due to the similarity between the two diseases in some respiratory symptoms. To assess the prevalence of COVID-19, we analyzed the influenza-like illness (ILI) and positive rate of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) detections in ILI patients reported to the influenza Surveillance Information System (CNISIS) since late 2022.
Data related to ILI were reported by national surveillance sentinel hospitals. Positive testing for SARS-CoV-2 and influenza viruses was conducted using real-time reverse transcription polymerase chain reaction (rRT-PCR) detection by the national influenza surveillance network laboratories. Surveillance data were reported to CNISIS.
Beginning on December 12, 2022 (Week 50), the ILI percentage increased dramatically, peaking in Week 51 at 12.1%. Subsequently, the ILI percentage began to decline rapidly from Week 52, 2022, and by Week 6, 2023 (February 6–12), the ILI and ILI percentage had returned to the levels observed at the beginning of December 2022. From December 1, 2022 to February 12, 2023, 115,844 specimens were tested for both SARS-CoV-2 and influenza virus. Of these, 30,381 (26.2%) were positive for SARS-CoV-2 and 1,763 (1.5%) were positive for influenza virus. The positive rate of SARS-CoV-2 tests peaked at 74.1% around December 23 and 25.
Sentinel-based surveillance, previously established for influenza, is an effective way to track the circulation trend of SARS-CoV-2 during community-level epidemics. There was no co-prevalence of SARS-CoV-2 and influenza virus during the outbreak of SARS-CoV-2, even during the winter influenza season. However, it is important to remain vigilant for the potential rise of influenza activities following the COVID-19 epidemic.


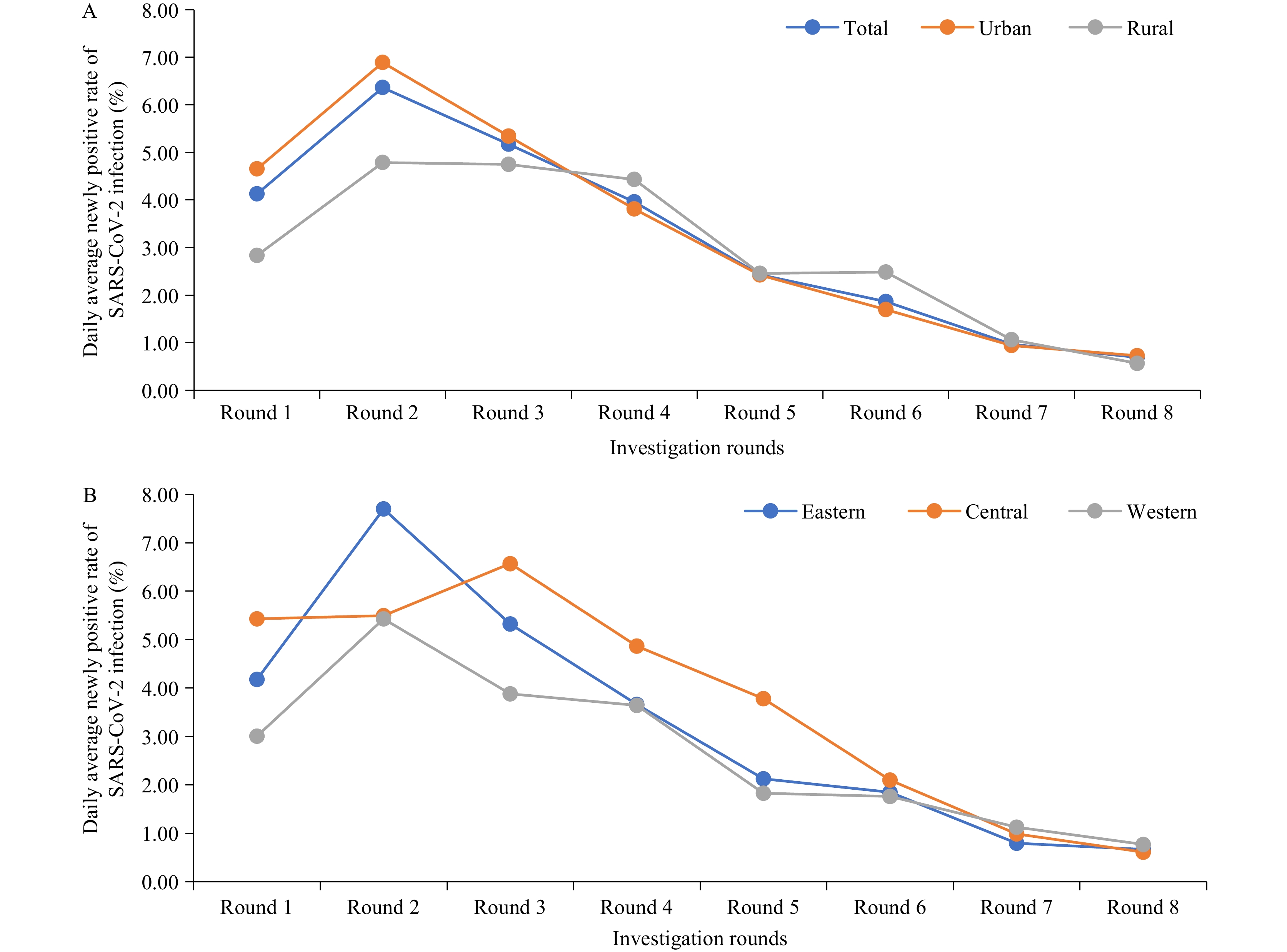
On December 7, 2022, China implemented the “Ten New Measures” to optimize its prevention and control measures for coronavirus disease 2019 (COVID-19). To provide the latest data after the optimization, we evaluated trends of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among the community population in China.
We utilized data from the National Sentinel Community-Based Surveillance (NSCS) system in China to assess trends of SARS-CoV-2 infection. NSCS is a national community-based surveillance cohort with 0.42 million participants from all 31 provincial-level administrative divisions (PLADs) and Xinjiang Production and Construction Corps (XPCC). Participants were tested for infection twice a week (a total of eight rounds) from December 16, 2022 to January 12, 2023. SARS-CoV-2 infection was defined as testing positive for SARS-CoV-2 nucleic acid or antigen. We calculated the daily average of newly positive rates of SARS-CoV-2 infection.
In this national cohort, the daily average newly positive rate of SARS-CoV-2 infection decreased from 4.13% in Round 1 (December 16–19, 2022) to 0.69% in Round 8 (January 10–12, 2023). The epidemic peak occurred in Round 2 (December 20–22, 2022). Similar trends were observed in urban areas (decreasing from 4.65% to 0.73%), rural areas (decreasing from 2.83% to 0.57%), the eastern region (decreasing from 4.18% to 0.67%), the central region (decreasing from 5.43% to 0.61%), and the western region (decreasing from 3.01% to 0.77%).
NSCS data showed that the peak of SARS-CoV-2 infection in China had passed. SARS-CoV-2 infection in community populations in China is currently at a low epidemic level.

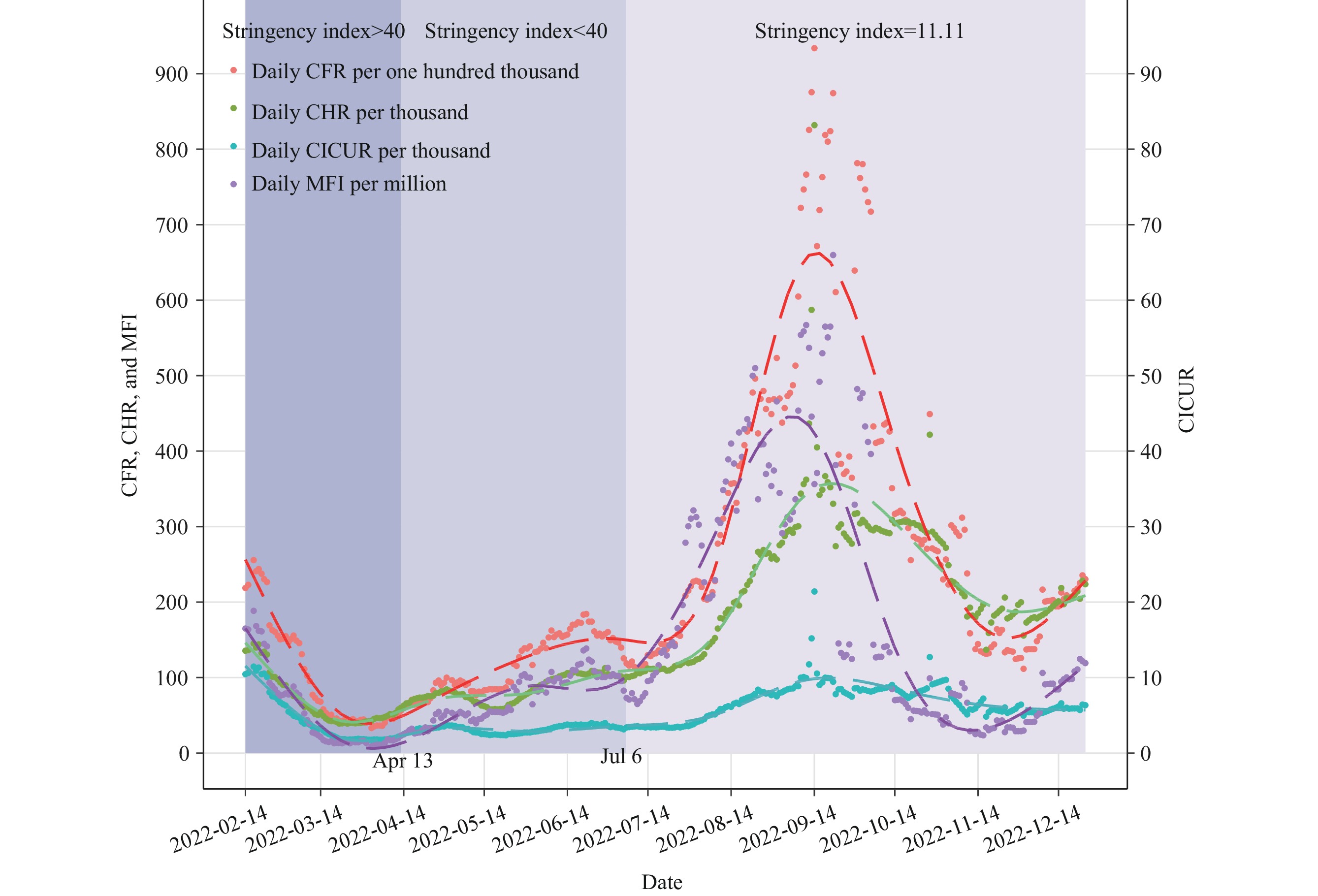
Hospitals have experienced a surge in admissions due to the increasing number of Omicron cases. Understanding the epidemiological features of coronavirus disease 2019 (COVID-19) and the strain it places on hospitals will provide scientific evidence to help policymakers better prepare for and respond to future outbreaks.
The case fatality rate of COVID-19 was 1.4 per 1,000 persons during the Omicron wave. Over 90% of COVID-19-related deaths occurred in individuals aged 60 years or older, with pre-existing chronic conditions such as cardiac conditions and dementia, particularly among males aged 80 years or older.
Public health policy is essential for preparing and preserving medical resource capacity, as well as recruiting additional clinicians and front-line staff in hospitals to address the increased demand. High-risk individuals should be prioritized for healthcare, vaccines, and targeted interventions.