
 Subscribe for E-mail Alerts
Subscribe for E-mail Alerts CCDC Weekly RSS Feed
CCDC Weekly RSS Feed2024 Vol. 6, No. 35
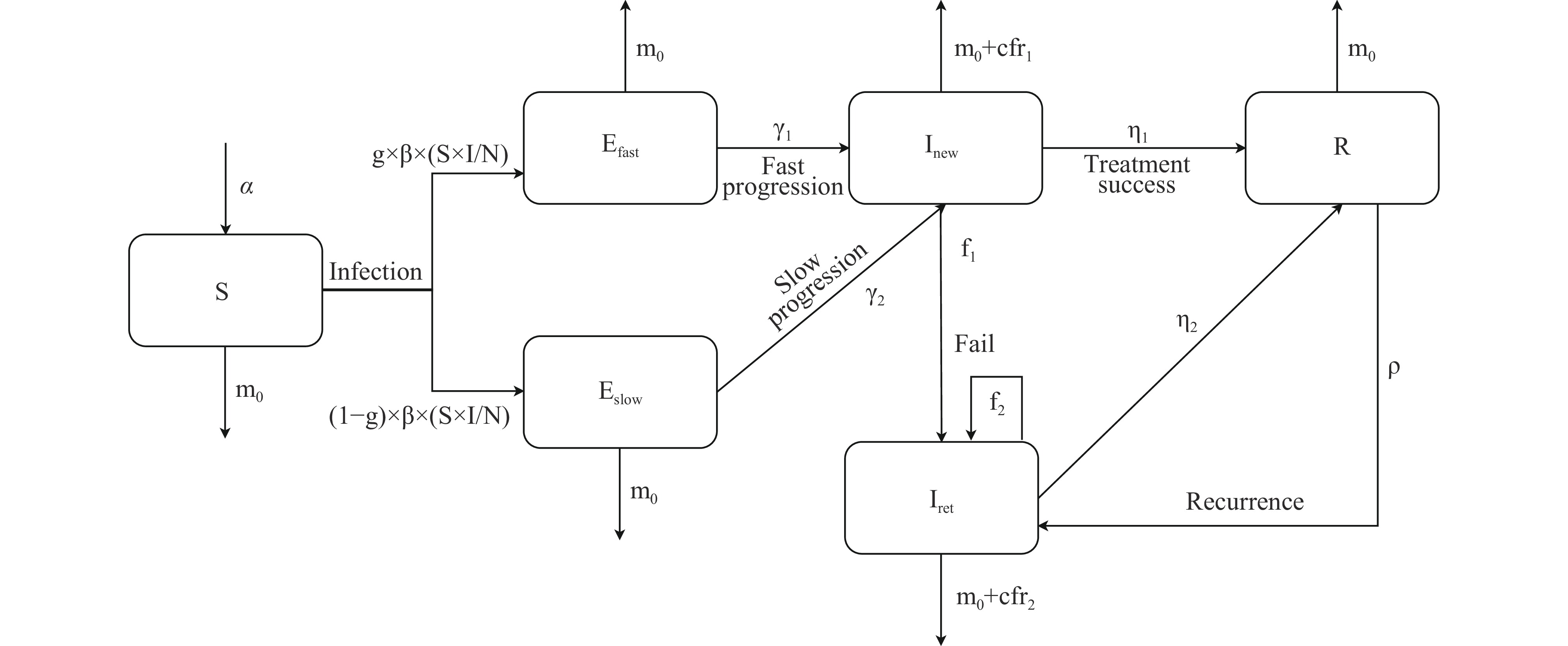
The recurrence of tuberculosis (TB) following successful treatment presents a significant challenge.
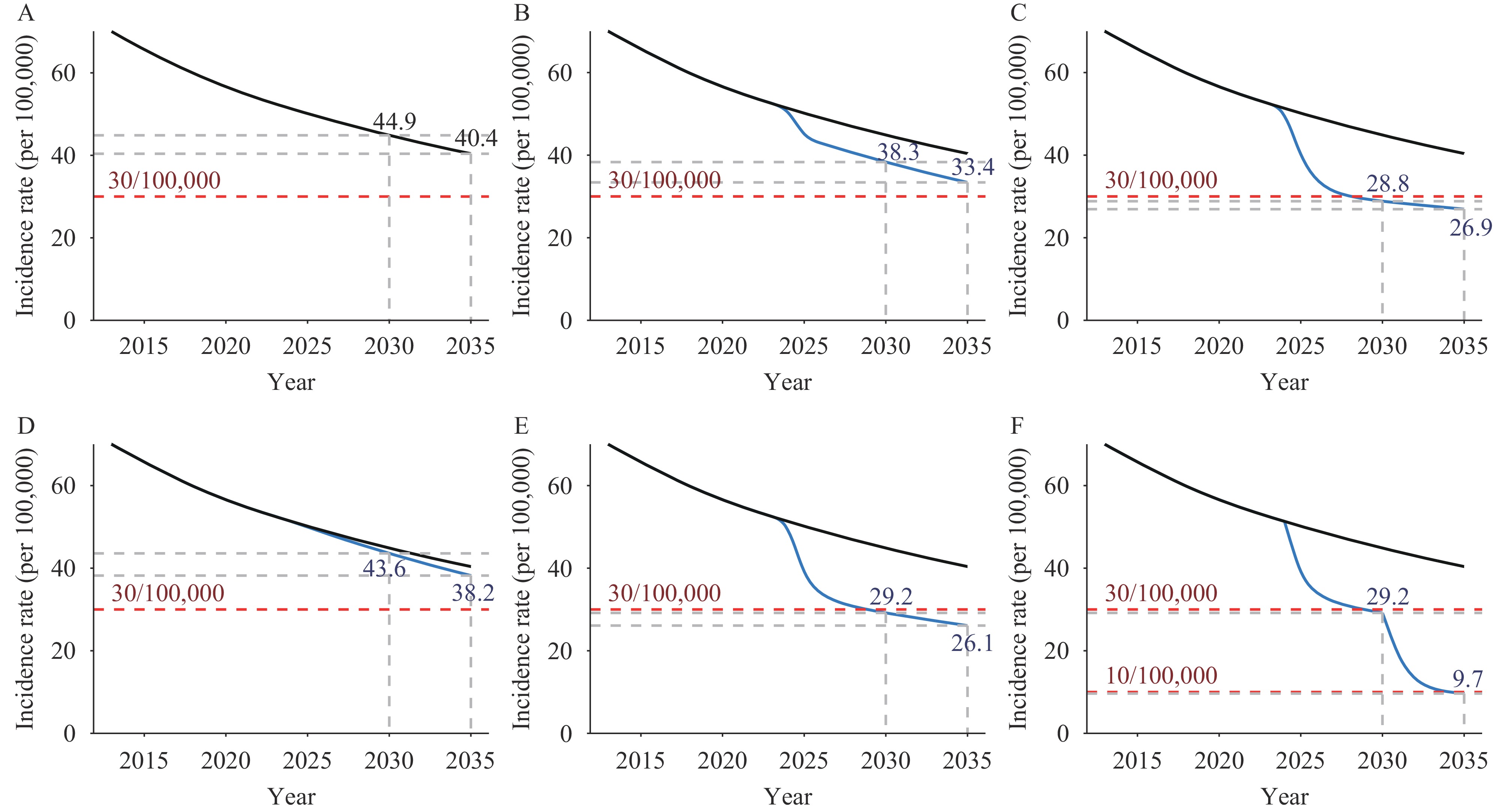
Achieving the global End TB Strategy milestones and targets with the current strategies in China is challenging. However, interventions following recovery to prevent recurrence, in conjunction with preventive treatment for latent TB infection (LTBI), will aid in meeting these objectives.
Implementing interventions to mitigate recurrence is essential for improving TB control strategies both in China and worldwide. Concurrently, the development of new drugs and vaccines should focus on preventing TB recurrence.
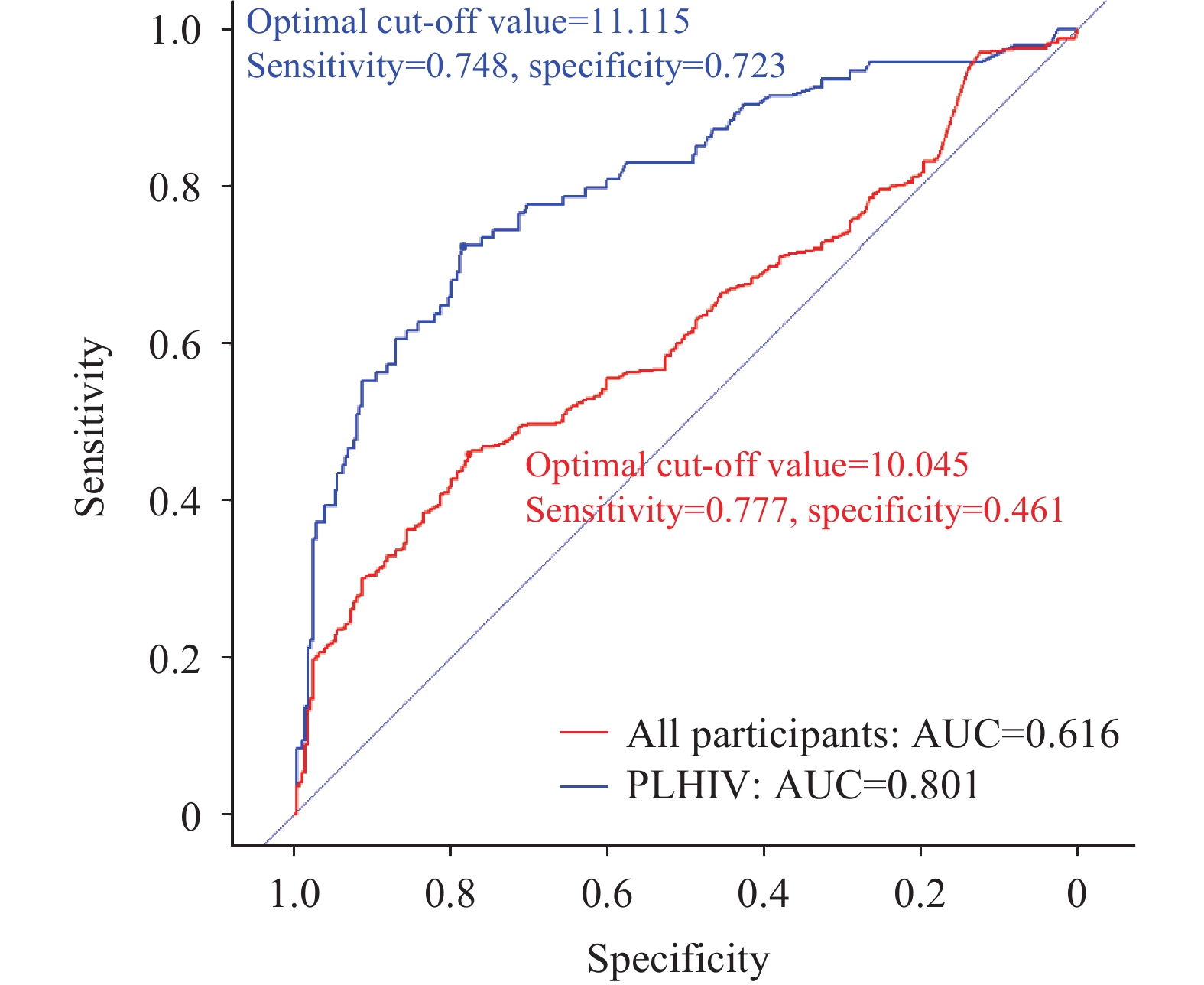
The World Health Organization (WHO) has recommended the inclusion of the C-reactive protein (CRP) test in active tuberculosis (ATB) screening algorithms among human immunodeficiency virus (HIV)-infected individuals. The performance of the CRP test in African regions has been well-documented.
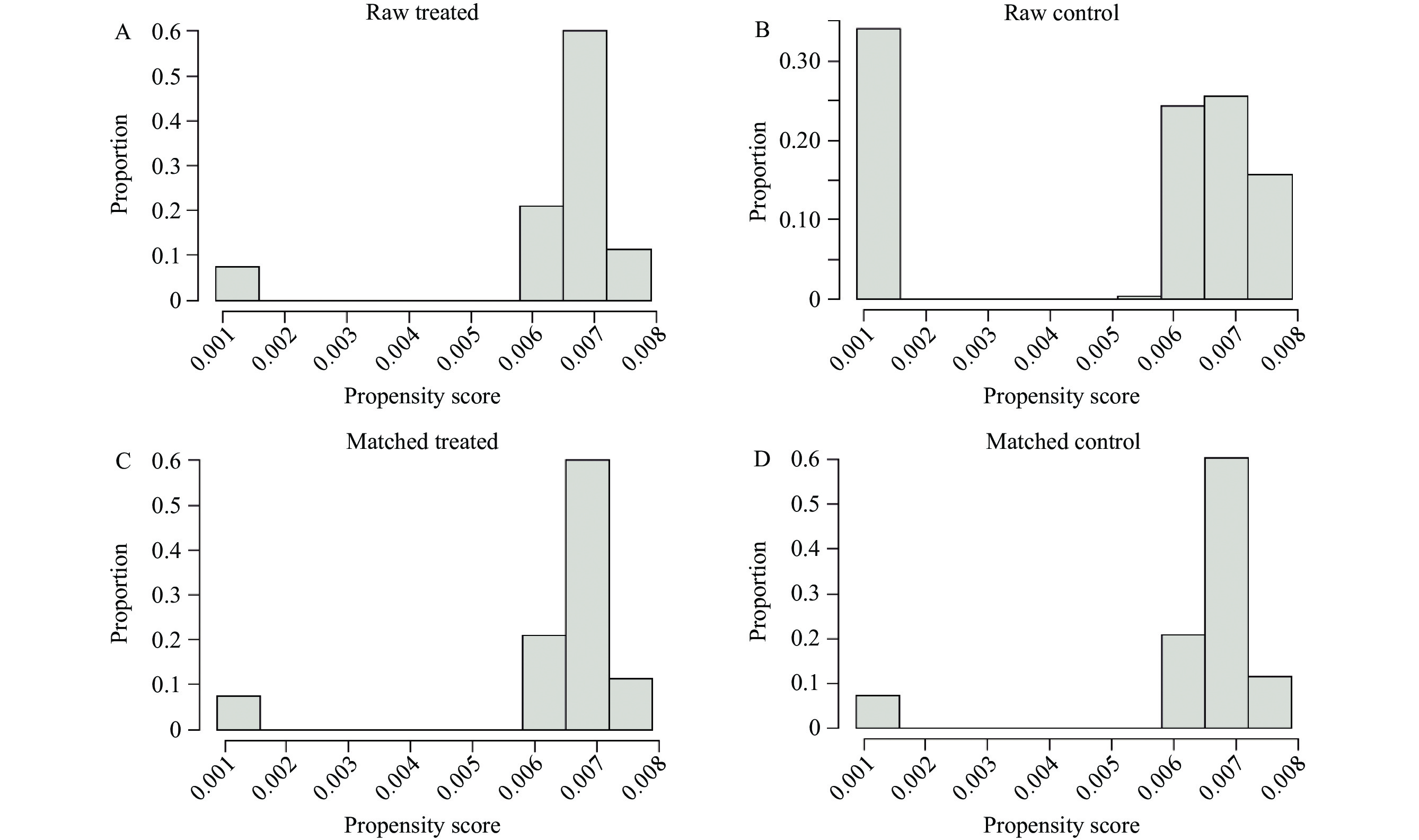
This study analyzed data from a big data platform of Shanghai medical records together with infectious disease surveillance systems. We simulated a screening and plotted a receiver operating characteristic (ROC) curve, which gives the optimal cut-off value of 11.115mg/L with sensitivity and specificity of 0.784 and 0.723, respectively.
We obtained a promising perspective on screening for tuberculosis in people living with HIV (PLHIV) using the CRP test in Shanghai. Our study offers an original standpoint for following research.
Newer skin tests, including the ESAT6-CFP10 (EC) skin test, were recommended for diagnosing Mycobacterium tuberculosis (M. tb) infection. However, no data exist assessing the diagnostic performance of the EC skin test among foreign students with different skin tones.
A cohort study at Nanjing Medical University screened incoming foreign freshmen. The EC skin test was used to assess for M. tb infection, and results were read at 24, 48, 72, and 96-hours post-administration.
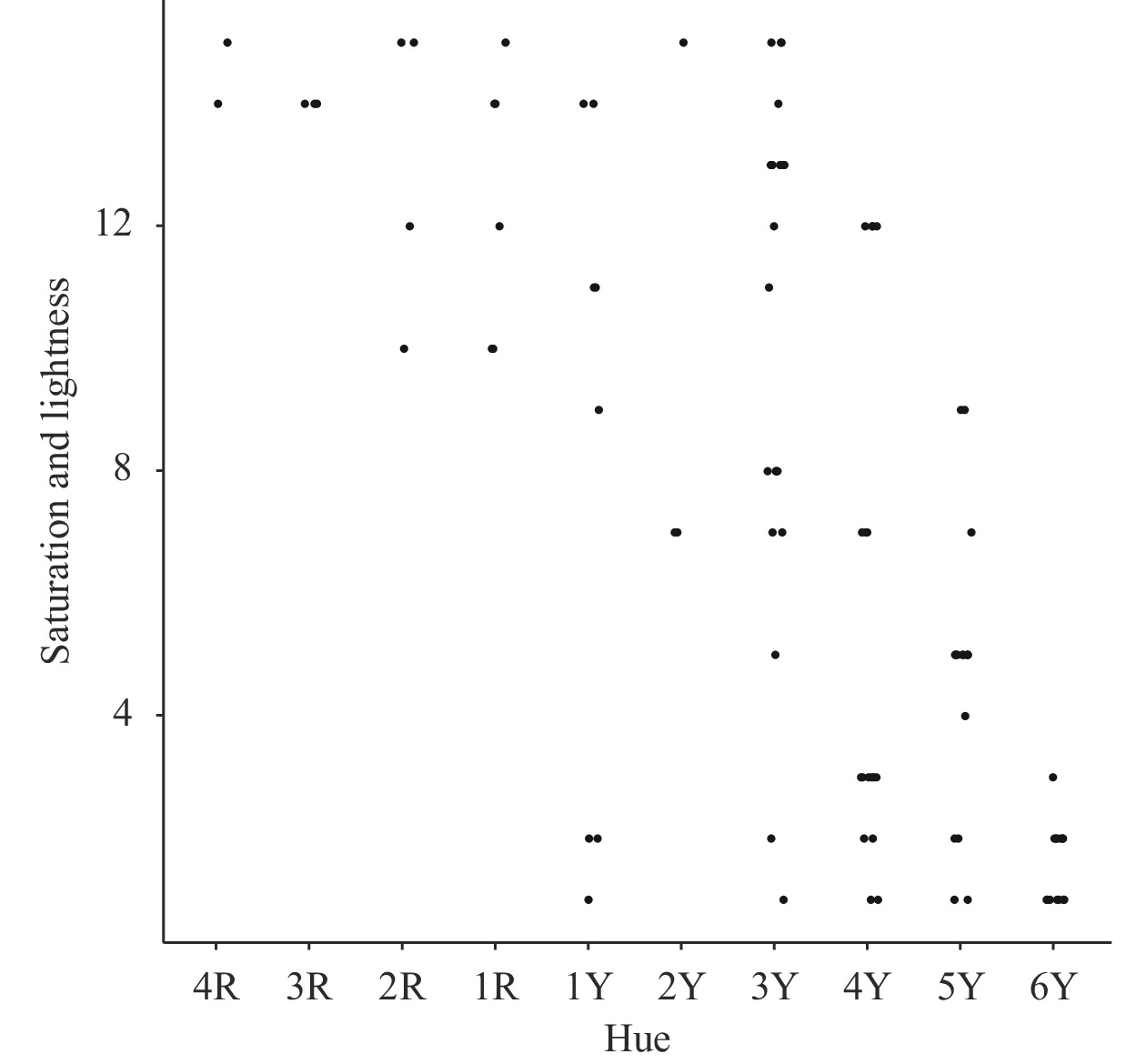
Among 96 participants, M. tb infection rates at 24, 48, 72, and 96-hours post-injection were 3.13%, 7.29%, 13.54%, and 9.38%, respectively. While infection rates were lower among individuals with darker skin tones, the difference was not statistically significant (P=0.186), and variations were consistent across different measurement times. Trajectory analysis revealed 5.3% in the continuous-increasing group, 86.5% in the low-stable group, and 5.2% in the elevated-decreasing group. Notably, participants in the elevated-decreasing group had lighter skin tones, with trajectory patterns consistent across different skin colors.
The EC skin test is safe, and redness diameter is a more reliable indicator than induration. Results should be collected within 48 to 72 hours, with verification at 72 hours crucial if initial results are negative. Importantly, skin color does not affect EC skin test outcomes.
