
 Download:
Download:




-
Globally, an estimated 7.5 million new tuberculosis cases were reported in 2022, with 87% concentrated in 30 high-burden countries. Approximately one-fourth of the global population is infected with Mycobacterium tuberculosis (M. tb) (1). The World Health Organization (WHO) guidelines strongly recommend screening and treatment for M. tb infection in populations at high risk for tuberculosis. Such screening is also conditionally recommended for recent immigrants from high-incidence to low-incidence settings (2). Identifying specific immigrant groups, such as foreign students, for M. tb infection management remains challenging in China. Tuberculosis outbreaks in schools have been frequently reported in recent years, partly due to inadequate tuberculosis screening of incoming freshmen (3). The prevalence of M. tb infection among freshmen in China, as determined by various diagnostic tests, ranged from 1% to 25% (3–4).
In 2022, alternative methods for diagnosing M. tb infection, including newer skin tests based on M. tb antigens, were recommended. One such test is the ESAT6-CFP10 (EC) skin test (5). Recent studies have indicated that the EC skin test demonstrates comparable diagnostic efficacy to IGRAs in the general population (6). Unlike Cy-Tb and Diaskintest, which measure induration diameters, the EC skin test uses the larger measurement of either induration or redness reaction. Redness has been shown to be clearly visible and measurable in Chinese individuals with lighter skin tones (7). However, whether the redness reaction of the EC skin test can be accurately measured on darker skin tones remains uncertain. Furthermore, data evaluating the diagnostic performance of the EC skin test among foreign students with varying skin tones are lacking.
To address this question, we recruited foreign students at Nanjing Medical University to assess the performance of the EC skin test in this high-risk population.
-
This cohort study was conducted in September 2023 at Nanjing Medical University. Screening was conducted as part of the admission process for foreign students in Jiangsu Province. Foreign students are required to undergo M. tb infection screening before university enrollment. The EC skin test developed by Zhifei Longcom Biologic Pharmacy Company was used to assess M. tb infection. Individuals were excluded if they had acute infectious diseases (e.g., measles, pertussis, influenza, pneumonia), acute conjunctivitis, or acute otitis media; a history of multiple drug allergies; or a history of hysteria.
-
For eligible participants, demographic information, including name, gender, age, nationality, educational background, and history of tuberculosis exposure, was collected before EC skin testing. EC skin tests were performed using the Mantoux method on the volar surface of the left forearm (7). Chest X-ray images were taken for all individuals before EC testing to rule out tuberculosis. Subsequently, EC skin test results were assessed at 24, 48, 72, and 96-hours post-administration. At each time point, induration and redness diameters were recorded, and images were captured to verify reactions. Each participant was monitored for a minimum of 30 minutes following test administration to detect acute adverse reactions. Pictures of induration and redness diameters were collected and examined by different staff members. Individuals were excluded from the study if they had acute infectious diseases (e.g., measles, whooping cough, influenza, pneumonia), acute conjunctivitis, or acute otitis media; a history of multiple drug allergies or hysteria; systemic skin diseases; or refused to have induration or redness measurements recorded.
After the injection, skin color was compared among all participants using the Pantone International Standard Color Chart. Yellowness (Y) ranges from 1Y (neutral) to 5Y (most yellow), with higher values indicating greater saturation and a darker appearance. Redness (R) ranges from 1R (neutral) to 5R (pinkest), with higher values indicating greater saturation and a tendency to appear darker. Darker skin was defined as a vertical axis value ≥7 and a horizontal axis value of 1Y–6Y. A positive EC result was defined as an induration or redness reaction ≥5 mm.
-
We used 2×2 contingency tables and means with standard deviations (SDs) to summarize continuous and categorical variables. The Fisher exact test or the χ2 test was used for intergroup comparisons, as appropriate. Repeated-measures analysis of variance (ANOVA) was used to compare skin color and reaction time.
Latent mixture modeling in Stata software (version 16.0; College Station, Texas, US) identified distinct developmental trajectory groups within a population. Models with four, three, two, and one trajectory patterns were examined. The model with the smallest negative Bayesian Information Criterion (BIC) value was selected. Various functional forms were compared based on the significance levels of cubic, quadratic, and linear terms, with P≤0.05 considered statistically significant.
-
This study received ethical approval from the human ethics committee of the Jiangsu Provincial Centers for Disease Control and Prevention was deemed necessary[approval number: JSJK2023-B029-02]. All eligible participants provided their consent by signing written informed consent forms.
-
Ninety-six individuals from 40 countries across six continents participated in the study. Of the 96 international freshmen screened, 49 (51.04%) were female. The median age was 22 years [interquartile range (IQR), 19–27]. More than half (55.2%) were undergraduates. Additionally, 59 individuals (61.46%) originated from 15 countries with a high burden of tuberculosis. Moreover, 61 participants (63.5%) reported lighter skin (Table 1 and Figure 1).
Variables Trajectory patterns of ESAT6-CFP10
skin testAll Continuous-
increasingLow-
stableElevated-
decreasingN (%) 96 (100) 8 (8.3) 83 (86.5) 5 (5.2) age 22 (19,27) 30 (19,35) 22 (19,27) 22 (21,30) Sex Female 49 (51.0) 3 (37.5) 44 (53.0) 2 (40.0) Male 47 (49.0) 5 (62.5) 39 (47.0) 3 (60.0) Education Undergraduate 53 (55.2) 3 (37.5) 47 (56.6) 3 (60.0) Postgraduate 43 (44.8) 5 (62.5) 36 (43.4) 2 (40.0) Region Low-burden 37 (38.5) 3 (37.5) 32 (38.6) 2 (40.0) High-burden 59 (61.5) 5 (62.5) 51 (61.4) 3 (60.0) Skin color Lighter skin 61 (63.5) 3 (37.5) 53 (63.9) 5 (100.0) Dark skin 35 (36.5) 5 (62.5) 30 (36.1) 0 (0) Table 1. Demographic characteristics of the 96 participants, overall and by trajectory patterns.
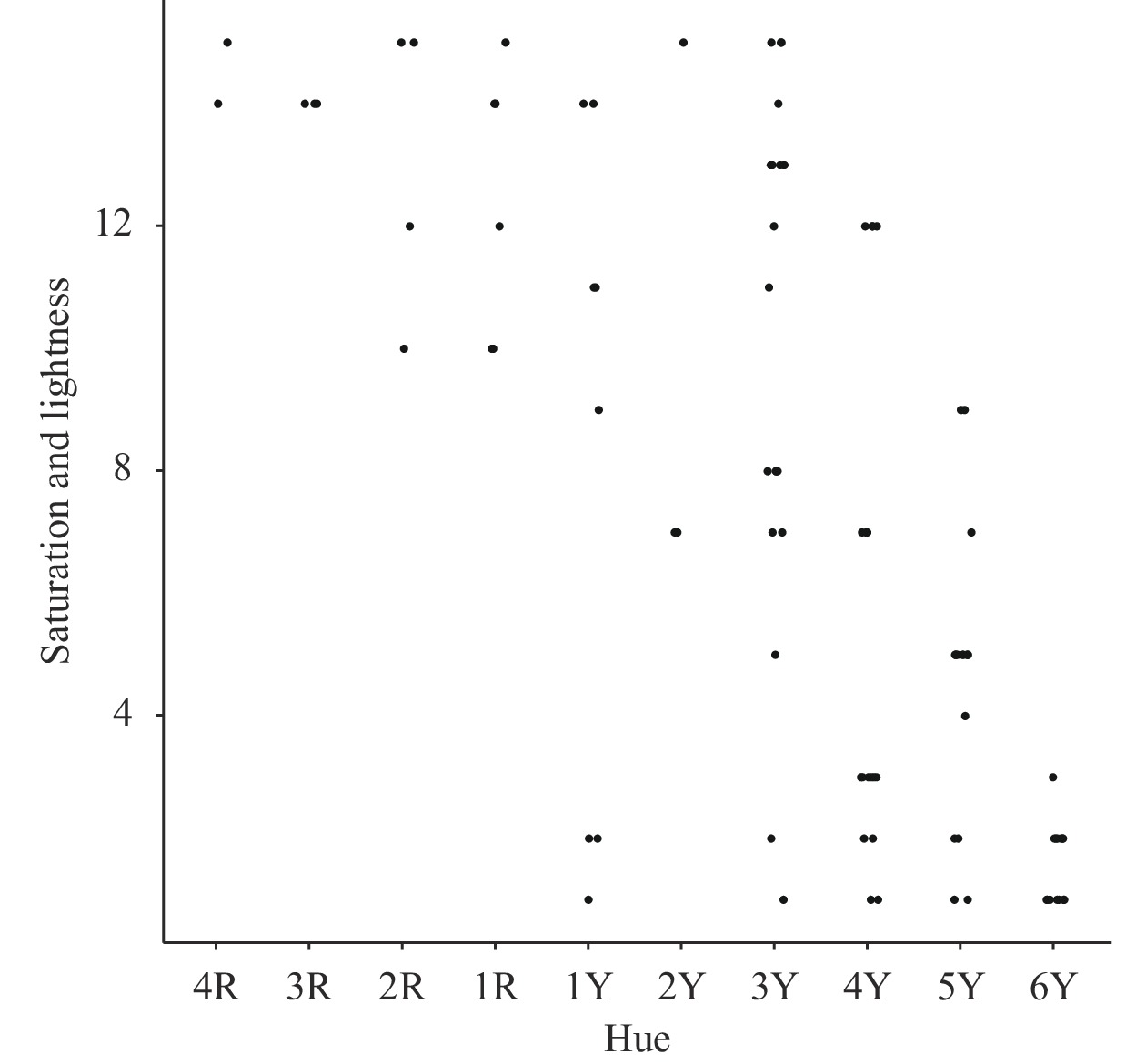 Figure 1.
Figure 1.Scatter plot of skin color distribution among 96 students.
Note: Hue is a fundamental concept in color theory, representing the attribute of color that determines its name (such as red, blue, yellow, etc.). It is a primary dimension of color, used to describe the specific type of color. Horizontal axis (Y, yellowness) ranges from 1Y (neutral) to 5Y (most yellow), with higher values indicating increased saturation and a darker appearance. Vertical axis (R, redness) ranges from 1R (neutral) to 5R (pinkest), with higher values indicating greater saturation and a darker tone. Darker skin: defined by a vertical axis value of ≥7 and a horizontal axis value between 1Y and 6Y. -
Supplementary Figure S1 illustrates that, across all 96 individuals, induration diameters remained consistently smaller than corresponding redness diameters at 24, 48, 72, and 96 hours post-injection. After 24 hours, there were 3 positive cases (all related to redness), representing a 3.13% positivity rate. By 48 hours, positive cases increased to 7 (positivity rate: 7.29%), including 5 individuals from high-burden tuberculosis countries (71.43%). At 72 hours, positive cases rose to 13 (positivity rate: 13.54%), with 8 individuals originating from high-burden tuberculosis countries. The 96-hour assessment revealed 9 positive cases (positivity rate: 9.38%), with 6 from high-burden tuberculosis countries (66.67%). -
Table 2 displays results from repeated measures ANOVA for EC skin test time points. Analysis showed varying infection rates across time points, with the highest rate at 72 hours post-injection (F=5.310, P=0.001), regardless of skin color. Mycobacterium tuberculosis infection rates were lower among individuals with darker skin tones compared to those with lighter skin tones, although this difference was not statistically significant (P=0.186). These variations were not affected by different measurement times.
Test Source Type IV sum of squares df Mean square F P Tests of within-subjects
contrastsTime 120.606 3 40.202 5.31 0.001 Time*group 21.328 3 7.109 0.939 0.422 Tests of between-subjects
effectsIntercept 557.644 1 557.644 6.411 0.013 Color 154.532 1 154.532 1.777 0.186 Abbreviation: ANOVA=analysis of variance; EC=ESAT6-CFP10. Table 2. Repeated measures ANOVA of different time results of EC skin test.
-
Following the trajectory analysis, 8 individuals (5.3%) were classified into the continuous-increasing group, 83 individuals (86.5%) into the low-stable group, and 5 (5.2%) into the elevated-decreasing group (Figure 2). Notably, all individuals in the elevated-decreasing group had lighter skin tones, but trajectory patterns did not differ based on skin tone.
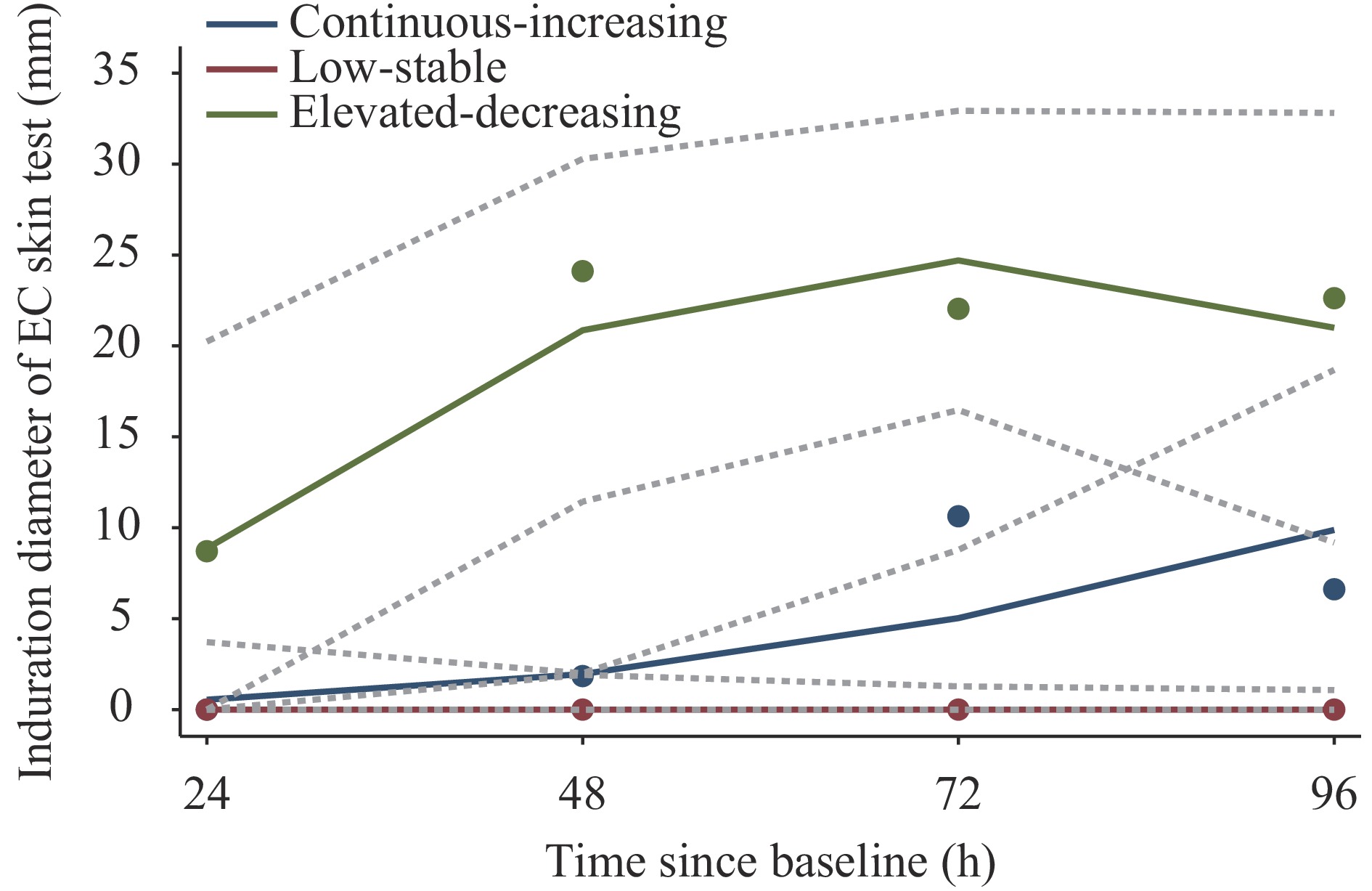 Figure 2.
Figure 2.Trajectory patterns of latent tuberculosis infection over 24, 48, 72, and 96 hours in the screening cohort.
-
Two (2.1%) of the 96 international students in this study experienced adverse reactions during EC skin testing. One participant experienced dizziness, and the other exhibited hyperventilation. Symptoms in both cases were alleviated with symptomatic treatments, such as oxygen administration. No other severe adverse reactions were observed.
-
The Chinese government has prioritized tuberculosis prevention among students, emphasizing screening for close contacts and incoming freshmen. This proactive approach, outlined in national guidelines jointly formulated by the Ministry of Health and Ministry of Education, demonstrates the government’s commitment to student well-being (3). Despite this, the use of the EC skin test among foreign individuals with different skin tones, particularly recent immigrants from high-tuberculosis-incidence regions, remains unexplored in university settings, posing a potential gap in tuberculosis control efforts.
In China, the prevalence of M. tb infection is notably higher among foreign freshmen than among native freshmen. Studies in Shanghai and Beijing reported infection rates among freshmen using various tests: in Shanghai, rates were 3.45% with the EC skin test and 9.00% with the TST (3); in Beijing, among high school freshmen, rates were 9.10% with the EC skin test and 5.35% with the IGRA (8). An investigation in Chongqing revealed positive rates of 10.14% with the EC skin test and 24.13% with the TST. Another study in Jiangsu Province involving 26,398 students indicated a tuberculosis infection rate of 5.68% with the TST (9). However, infection rates among native Chinese students were consistently lower than those among foreign students. Elevated figures observed with the TST may be attributed to false positives associated with the Bacillus Calmette-Guérin vaccine (10).
In our study, we substantiated that the optimal timeframe for assessing the reaction to the EC skin test in foreign students is between 48 and 72 hours post-injection, aligning with the recommended instructions. This parallels the protocols of similar skin tests, such as Cy-Tb (Serum Institute of India, India) (11) and Diaskintest (Generium, Russian Federation) (11), which also advocate for the 48–72-hour window. Our research suggests that for evaluating the EC skin test in foreign students, 72 hours may be more appropriate than the commonly favored 48-hour mark. This conclusion is based on two randomized trials, which showed the highest median diameter of redness or induration at 48 hours compared to 24 and 72 hours. Interestingly, some foreign students initially had negative reactions at 48 hours but turned positive at 72 hours, with some showing increased reactivity up to 96 hours. The reasons for this phenomenon are unclear but could be due to darker skin tones requiring longer to show redness or delayed hypersensitivity among foreign students, necessitating a longer timeframe for reliable results (12–13).
In our study, we observed that the diameter of redness was consistently greater than that of induration among generally healthy foreign students (7), even when some reactions were positive at 24 h after injection. Notably, in contrast to Cy-Tb (Serum Institute of India, India) (11), Diaskintest (Generium, Russian Federation) (14), and TST (15), which rely on the measurement of induration diameter as the primary reaction parameter, our findings highlight the prevalence of a larger redness diameter in our participant cohort. One explanation is that the sensitivity of the skin test response was diminished by the removal of certain nonspecific antigens unrelated to M. tb. This modification may have reduced the test’s ability to detect reactions effectively. Additionally, another factor influencing the observed differences is the distinct genetically modified bacillus used in the EC skin test compared to that used in Cy-Tb and Diaskintest (5).
Furthermore, our investigation revealed that skin color did not impact the response to the EC skin test. In contrast to Cy-Tb and Diaskintest, which measure induration, the EC skin test considers the greater measurement of either redness or induration. This might pose a challenge in accurately gauging reaction diameter in individuals with darker skin tones. Notably, the diameter of redness was consistently larger than that of induration. Despite this observation, the finding that skin color does not influence the EC skin test response is reassuring and suggests its potential applicability for individuals with darker skin.
This study is subject to several limitations. First, the lack of a gold standard for M. tb infection precluded the use of IGRA or TST as a reference, limiting our ability to confirm the appropriateness of the 5mm cutoff point for the EC test in foreign individuals. Second, the small sample size limited our ability to determine the true M. tb infection rate among foreigners across subgroups. Future research should include larger studies of foreign individuals to comprehensively assess M. tb infection rates in diverse populations.
In summary, this study found a persistently high M. tb infection rate among foreign freshmen, as determined by the EC skin test. The test demonstrated a positive safety profile, with redness diameter proving a more reliable indicator than induration. It is recommended to assess EC skin test results between 48 and 72 hours, particularly if initial results at 24–48 hours are negative. Importantly, skin color did not impact test outcomes in our study. Greater attention should be given to international individuals, particularly recent immigrants from regions with high tuberculosis incidence, to address potential gaps in tuberculosis control efforts.
HTML
Study Design and Participants
Procedures
Statistical Analysis
Ethical Approval and Participant Consent
Subject Characteristics
Detection of M. tb Infection of Different Time
Effects of Time and Skin Color on M. tb Infection
Trajectory Patterns of Different Measurement Time Points
Safety of the EC Skin Test Among International Students
| Citation: |

|