
 Download:
Download:




-
Introduction: Malaria is a major public health concern in Pakistan. Data examining the relation between topography and malaria transmission in Pakistan are limited. This study aimed to analyze malaria transmission in relation to topography across Khyber Pakhtunkhwa from 2019 to 2022.
Methods: This retrospective study analyzed malaria case data collected from the provincial health department, the District Health Information System, and district health offices across Khyber Pakhtunkhwa. Time-series analysis was conducted to determine malaria trends over time.
Results: The results showed the highest cumulative case counts in Charsadda (303,900), Dera Ismail Khan (292,070), and Bannu (241,640), whereas high-altitude districts, such as Kolai Palas (2.56 km), reported far fewer cases (<1,000). These findings indicate an inverse relation between altitude and malaria incidence, highlighting high vector density in low-altitude regions.
Conclusion: Topography strongly influences malaria risk. Integrating elevation-based spatial data into provincial malaria control policies is recommended.
-
Malaria remains a major public health concern, with more than 282 million cases and over 610,000 deaths reported worldwide by 2024, despite decades of progress in control and prevention efforts. Millions of people in Pakistan are affected annually (1). The global disease burden of malaria is particularly high in sub-Saharan Africa and parts of Asia, where environmental and geographical conditions strongly influence the transmission dynamics of Plasmodium parasites (2). Malaria control strategies in Pakistan focus on optimal resource allocation to enhance surveillance and reduce disease burden, particularly in the context of population vulnerability, displacement, and climate change (3).
Despite intensive efforts to eliminate malaria since the 1960s, the disease resurged in the 1970s and has remained endemic in several regions because of multiple factors, including environmental and socioeconomic conditions that contribute to transmission (4). Topography is an important determinant of malaria transmission, as regions with high elevation and low temperatures generally exhibit low transmission risk (5). However, recent advances in spatial modeling, remote sensing, and Geographic Information Systems have enhanced malaria risk assessment by producing high-resolution risk maps (6).
Malaria is recurrent across all provinces of Pakistan; however, the country remains a low-resource setting and bears a high burden of malaria-related morbidity, mortality, and prevention costs. Topographic variations in Khyber Pakhtunkhwa (KP) have not been adequately considered in previous analyses. Therefore, this study analyzed malaria transmission patterns in KP from 2019 to 2022.
Secondary data on malaria incidence were obtained from the Provincial District Health Information System and District Health Offices across multiple districts. These data included the number of malaria cases reported in each district. Case records were initially verified by a district medical entomologist and subsequently approved by a provincial medical entomologist. Blood smear microscopy was used for malaria diagnosis (1). Data on latitude, longitude, and altitude were obtained from the Provincial Meteorological Department, Peshawar.
KP is located in northwestern Pakistan and is the third most populous province in the country. The study population included all districts of KP, while the target population comprised malaria-sensitive districts. The province was categorized into three zones to assess the impact of topography on malaria transmission:
Southern KP: Bannu, Tank, Karak, and Dera Ismail Khan.
Northern KP: Haripur, Abbottabad, Dir, Kohistan, Swat, and Chitral.
Central KP: Peshawar, Charsadda, Nowshera, and Mardan.
Districts were further classified as low-altitude (<0.46 km), mid-altitude (0.46–1.22 km), and high-altitude (>1.22 km;
Supplementary Table S1 ).The topographic distribution of KP highlighting high-altitude regions, such as Chitral and Swat, and low-altitude regions, such as Bannu and Dera Ismail Khan.
Statistical analyses were performed using SPSS (version 25.0, Armonk, NY, USA: IBM Corp.). Pearson’s correlation analysis was used to assess the association between altitude and malaria incidence. QGIS software was used to generate maps and figures. A time-series analysis was conducted to examine malaria trends across KP districts. Space–time permutation scan statistics were applied to identify malaria hotspots in the region.
The incidence of malaria varies across the topography of KP from 2019 to 2022. Between 2019 and 2022, the confirmed malaria cases varied significantly across the KP districts (Table 1). Charsadda had the highest cumulative burden (303,900 cases), followed by Dera Ismail Khan (292,070 cases), Bannu (241,640 cases), and Mardan (233,749 cases). By contrast, districts, such as Kohistan Lower (423 cases), Kolai Palas (606 cases), and Kohistan Upper (1,637 cases), recorded the lowest number of cases. Districts with low altitudes, such as Dera Ismail Khan (0.18 km) and Lakki Marwat (0.17 km), reported high case numbers, whereas high-altitude regions, such as Kolai Palas (2.56 km) and Kohistan Upper (1.91 km), showed markedly fewer cases. Malaria incidence per 10,000 population is shown in
Supplementary Table S1 , which indicates that northern districts have a lower incidence than southern districts with low altitude.District 2019 (n) 2020 (n) 2021 (n) 2022 (n) Latitude (º N) Longitude (º E) Altitude (km) Bannu 32,640 68,284 70,983 69,733 32.986 70.604 0.36* Dera Ismail Khan 51,209 78,252 75,800 86,809 31.862 70.901 0.18* Lakki Marwat 34,240 50,705 48,114 85,480 32.613 70.901 0.17* Tank 25,734 22,807 25,132 33,576 32.216 70.389 0.26* Abbottabad 1,861 190 923 474 34.168 73.221 1.26§ Haripur 7,263 3,530 3,996 5,019 33.994 72.910 0.52† Kohistan Upper 402 133 412 690 34.250 73.500 1.91§ Mansehra 1,901 1,087 1,586 1,756 34.331 73.198 1.09† Battagram 419 632 279 2,352 34.672 73.024 1.04† Tor Ghar 1,821 525 266 1,907 34.449 70.199 2.44§ Kohistan Lower 20 62 169 172 35.250 73.500 1.68§ Kolai-Palas 20 24 100 462 35.100 73.000 2.56§ Karak 13,243 17,306 17,084 25,813 33.111 71.091 0.55† Kohat 22,048 24,612 25,746 40,640 33.589 71.443 0.49† Hangu 13,073 17,598 21,335 31,138 33.522 71.062 0.81† Buner 21,096 18,184 32,177 48,014 34.394 72.615 0.80† Chitral Lower 6,621 3,327 5,445 4,143 35.370 71.740 1.49§ Dir Lower 27,721 27,640 39,994 47,309 35.370 71.740 0.97† Malakand 16,711 11,886 14,543 20,104 34.503 71.905 0.45* Swat 21,085 23,280 17,684 14,066 35.223 72.426 0.98† Dir Upper 12,883 11,434 12,011 7,234 35.208 71.875 1.84§ Shangla 14,419 20,157 26,066 41,316 34.802 72.757 1.52§ Chitral Upper 679 332 484 453 35.833 71.783 1.50§ Mardan 45,446 48,968 57,322 82,013 34.199 72.040 0.28* Swabi 7,182 4,589 4,527 4,230 34.117 72.281 0.34* Charsadda 53,718 74,692 87,219 88,271 34.149 71.743 0.30* Nowshera 29,467 20,780 29,518 43,286 34.011 71.988 0.55† Peshawar 8,852 7,274 10,713 37,370 34.026 71.560 0.37* * means low altitude (<0.46 km);
† means mid-altitude (0.46–1.22 km);
§ means high altitude (>1.22 km).Table 1. District-wise confirmed malaria cases in Khyber Pakhtunkhwa.
Districts, such as Bannu, Dera Ismail Khan, and Lakki Marwat, are located at low altitude but accounted for more than 60% of cases; similarly, in central KP, Peshawar, Mardan, Charsadda, and Nowshera recorded higher confirmed malaria cases compared with those of other districts of KP (Figure 1). A negative correlation was observed between altitude and malaria incidence rates from 2019 to 2022 (Figure 2). Space–time permutation analysis was used to identify hotspot districts based on incidence (
Supplementary Figure S1 ). Lakki Marwat and Tank, located at low altitudes, exhibited the highest incidence rates, indicating persistent spatial hotspots, whereas Shangla, Hangu, and Bannu demonstrated emerging and expanding temporal risks. Districts located at low altitudes (<1,500 ft) had a high malaria burden, whereas high-altitude districts (>4,000 ft) consistently reported low case counts.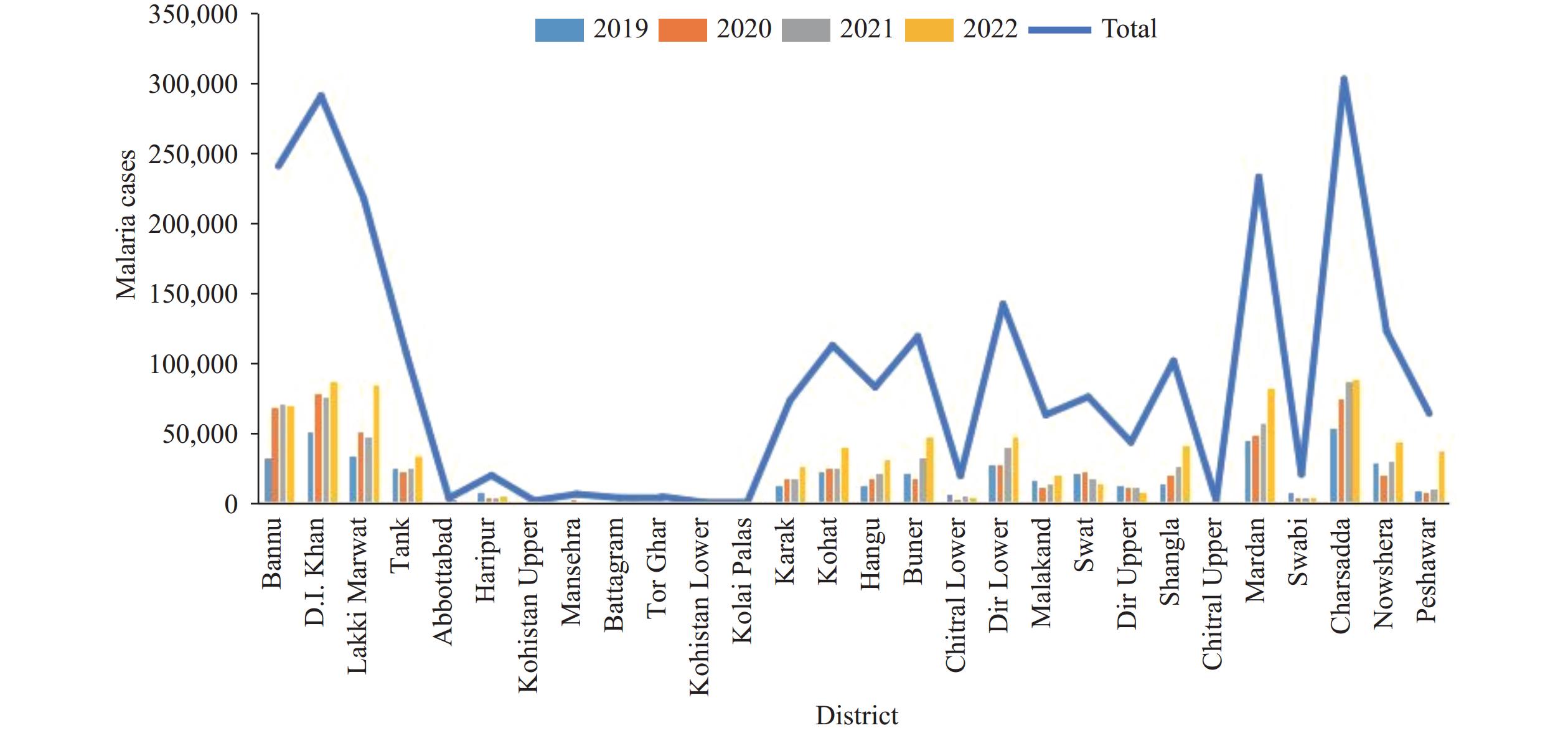 Figure 1.
Figure 1.Confirmed malaria cases in various districts of Khyber Pakhtunkhwa, Pakistan.
Note: Low-altitude districts [including Bannu and Dera Ismail (D.I) Khan] accounted for more than 60% of total cases.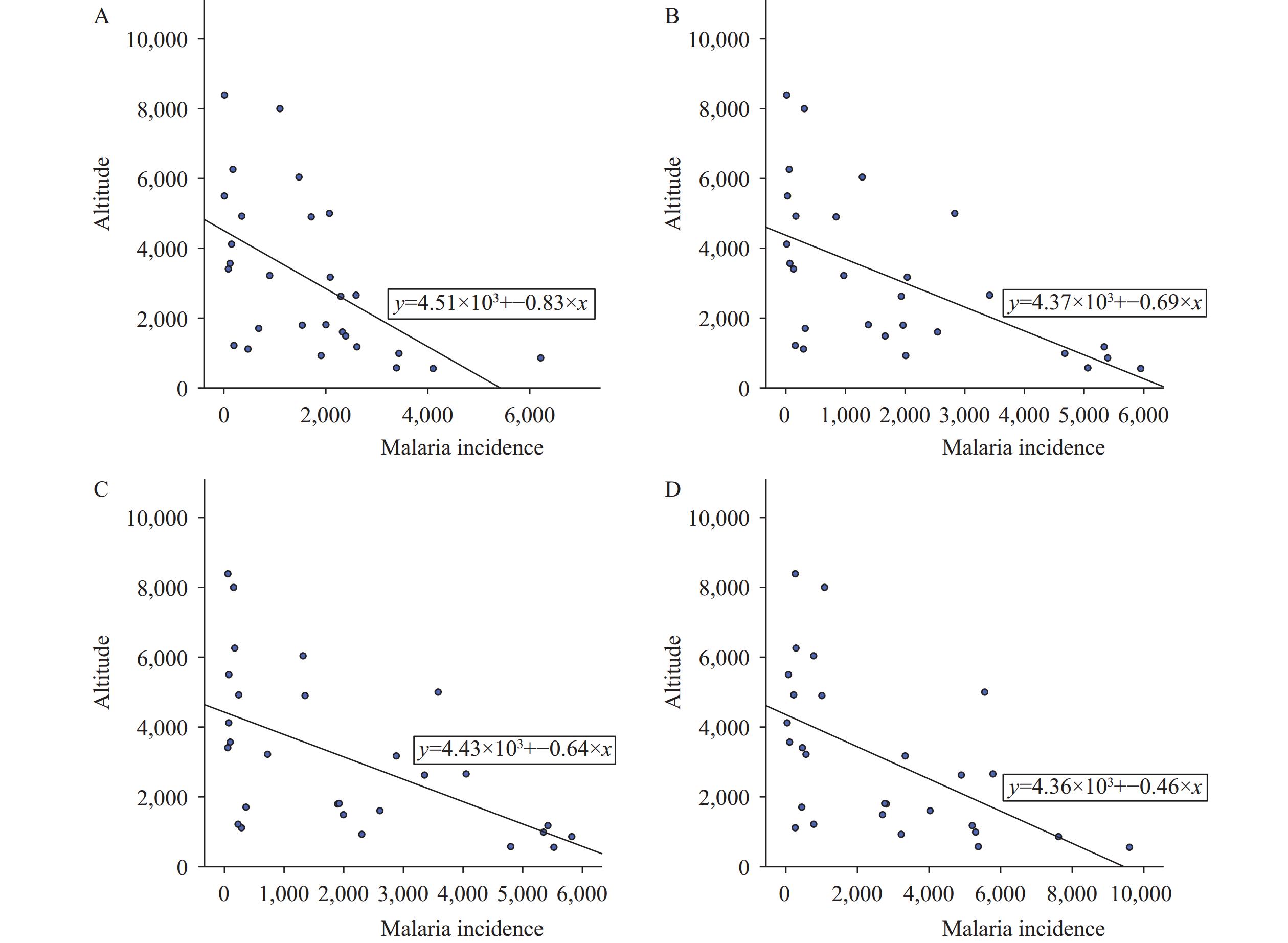 Figure 2.
Figure 2.Scatter plot of altitude versus malaria incidence rates in Khyber Pakhtunkhwa. (A) 2019; (B) 2020; (C) 2021; (D) 2022.
Note: There was a negative correlation between altitude and malaria incidence across the study period; the altitude was measured in feet. -
This study investigated the spatial distribution of malaria incidence based on topographic features across several districts of KP, Pakistan. The findings demonstrate a strong association between malaria incidence and topographic factors.
Spatial heterogeneity in vector density and disease risk has emerged as a major concern. Kouame et al. showed that even within the same region, the relation between vector abundance and malaria incidence may differ because of local geographical and environmental factors (7). This insight is particularly important in the context of KP, where variable topography creates localized transmission patterns that cannot be addressed using uniform control approaches. In our study, malaria incidence hotspot districts were identified, showing that low-altitude areas had high malaria case counts. This pattern suggests that altitude plays a modifying role in malaria transmission within provinces. There is evidence that malaria transmission declines with increasing altitude, as highland areas report significantly fewer cases than those of low-altitude areas (8). Previous studies have developed high-resolution malaria models incorporating population density, climate, and surface hydrology (9). In our study, districts with seasonal flooding and irrigation infrastructure had high malaria incidence, which is consistent with these findings. Furthermore, our results align with those of studies from Africa that identified significant associations between malaria frequency and topographic variables, such as elevation and slope. Their spatial modeling approaches informed the analytical framework of our study, underscoring the need to incorporate topography into disease surveillance systems. High topographic features restrict malaria transmission from highland areas to lowlands, where malaria-related morbidity is high (2).
Geographical highlands influence vector density. Bannu District, a southern district, has a low altitude but high mosquito density, which leads to elevated malaria prevalence. Malaria transmission is higher in KP than in other provinces, such as Punjab and Sindh (3). Punjab may have more effective vector control strategies. In addition to altitude, increased temperature (≥22.4 °C) enhances vector density and, consequently, malaria transmission (10). Climatic factors, such as high rainfall, humidity, and flooding, promote habitat development, vector population growth, vector longevity, and breeding site availability, thereby facilitating malaria transmission. Several studies have examined malaria incidence in parts of KP; however, these efforts have largely been limited to district-level analyses or have focused primarily on environmental factors (3,10). These studies assessed the effects of temperature, humidity, and rainfall on malaria incidence in Pakistan. By contrast, there remains a lack of systematic topographic evaluations assessing how elevation, slope, and terrain influence malaria transmission across Pakistan, particularly in KP. Furthermore, no previous study has specifically examined spatial trends using province-wide data from KP.
This study has some limitations. First, data were obtained from the District Health Information System and district health offices. Malaria cases are often underreported because of poor communication or because hospital and facility staff are engaged in competing responsibilities. Second, at the district level, there is typically only one medical epidemiologist responsible for multiple facilities, which further contributes to data limitations.
In conclusion, this study highlighted the importance of topography in malaria transmission. High altitudes were associated with few cases, whereas low altitudes were associated with high malaria transmission in KP. Altitude was negatively correlated with malaria incidence throughout the study period. Low-altitude districts with a high malaria burden require weekly surveillance, including hotspot mapping and the allocation of up to 150,000 rapid diagnostic tests (RDTs) per year. Mid-altitude districts require biweekly monitoring, hotspot mapping, and the allocation of up to 70,000 RDTs per year. High-altitude districts with a low malaria burden require monthly surveillance, hotspot monitoring, and the allocation of up to 10,000 RDTs per year. Policymakers should consider altitude-related risks in hotspot areas when designing malaria prevention strategies in the region.
-
The Deanship for Scientific Research, King Faisal University, Saudi Arabia, for funding this study.
-
Ethical approval for this study was obtained from the Ethics Review Board of the University of Agriculture, Pakistan.
HTML
| Citation: |

|