
 Download:
Download:




-
Coal worker pneumoconiosis (CWP) results from prolonged dust inhalation by miners and remains incurable. Despite a decline in the overall incidence of pneumoconiosis, it remained the most prevalent occupational disease in 2022, accounting for 68% of cases and 9,613 deaths, according to the National Health Commission statistical bulletin.
Evidence suggests a strong link between lipid metabolism and pulmonary fibrosis. For instance, mice deficient in the Elovl6 gene exhibit altered lung lipid profiles and an exacerbated fibrotic response to bleomycin (1). Phospholipids, the primary constituents of pulmonary surfactants, demonstrate cell type-specific distributions within the lung: phosphatidylglycerol (PG) and phosphatidylcholine (PC) predominate in alveolar cells, phosphatidylethanolamine (PE) in macrophages, and phosphatidylinositol (PI) in bronchial epithelial cells. Dysregulation of phospholipid homeostasis can trigger myofibroblast activation, extracellular matrix deposition, and ultimately, fibrosis (2). Moreover, oxidized phospholipids may contribute to inflammation following lung injury. Impaired phosphatidylcholine secretion, for example, has been shown to promote M2 macrophage reprogramming and fibrosis (3). Similarly, knockdown of autotaxin in bronchial epithelial cells or macrophages attenuates collagen accumulation after bleomycin exposure (4). Collectively, these findings underscore the multifaceted roles of phospholipids in cellular structure, inflammatory responses, and the regulation of oxidative stress.
Studies have shown that phospholipids are closely linked to the inflammatory process of pulmonary fibrosis and may serve as potential diagnostic biomarkers (5-6). However, the literature on phospholipid alterations in CWP and their potential as CWP biomarkers remains limited.
In summary, this study conducted targeted lipidomics analysis of 22 disease-related phospholipids using UPLC-MS/MS to evaluate their potential as serum biomarkers for CWP (7).
-
A total of 217 subjects were recruited, including 62 stage I CWP patients (PN group) from a Beijing coal mine, 50 healthy volunteers (HT group), and 105 environmental control group members (EX group). All subjects were aged 40–55 years with a BMI of 18.5–30.0 kg/m2. Pneumoconiosis diagnoses were confirmed by three occupational physicians according to the "Diagnostic Criteria of Pneumoconiosis" in China. The EX group consisted of coal mine dust-exposed workers sharing the same environment as the PN group and at high risk for pneumoconiosis, while healthy volunteers were matched to the patients by age and sex. Exclusion criteria included COPD, asthma, tuberculosis, or cancer. Lung function tests (FVC, FEV1, MMEF) for the PN and EX groups were conducted following Chinese Thoracic Society guidelines. Subjects with hypertension, arthritis, or gastritis were categorized as having chronic conditions. Serum was separated from 5 mL blood samples and then stored at −80 °C.
-
Our research team established a targeted lipidomics approach using a UPLC-MS/MS system (Waters Corp., USA) with electrospray ionization (ESI). The mobile phase consisted of methanol/water (5:95, v/v) with 10 mmol/L ammonium formate (Solvent A) and methanol (Solvent B), at a flow rate of 0.4 mL/min and an injection volume of 5 μL. Details of the mobile phase gradient and multiple reaction monitoring (MRM) parameters are available in our previous study (7). Quality control (QC) samples were analyzed every 30 samples during the run.
-
Statistical analyses were performed using IBM SPSS Statistics 25 (International Business Machines Corporation, New York, USA.) and R 4.3.2 (supported by The R Foundation for Statistical Computing, Vienna, Austria). The Student’s t-test and Mann-Whitney U test were used for continuous variables, depending on data distribution, while Pearson’s χ2 test assessed categorical variables. P values were adjusted for the False Discovery Rate (FDR) using the Benjamini-Hochberg method and reported as q values. Data are presented as means±standard deviation (SD), percentages, or medians (25th, 75th percentiles). Box-Cox transformation was applied to normalize the data before multifactorial analysis. Multivariate analysis included PCA and PLS-DA, with model fit assessed by R2 and Q2. Differential lipid metabolites were identified based on q<0.05, variable importance in the projection (VIP)>1, and fold change (FC)>1.2. Receiver operating characteristic (ROC) curves evaluated the sensitivity, specificity, and the area under the curve (AUC) of these metabolites in distinguishing groups. Spearman’s rank correlation was used to test correlations, and 10-fold cross-validation was performed to assess model generalization. Statistical significance was set at q<0.05. To further investigate these differential metabolites, differential phospholipid pathway analysis was performed using MetaboAnalyst 6.0 (McGill University, Montreal, Canada).
-
A total of 217 all-male subjects were included in the study: 62 with pneumoconiosis (PN group), 105 dust-exposed workers (EX group), and 50 healthy individuals (HT group). There were no significant differences in age, BMI, smoking status, alcohol consumption, or chronic disease prevalence across the three groups; however, the PN group had a significantly longer dust exposure duration than the EX group. Lung function tests were conducted on the PN and EX groups, with no significant differences observed (Table 1). After removing phospholipids with >30% missing values, the quantitative values for each group are listed in Table 2. In univariate analysis, significant differences in phospholipids were identified between the PN and HT groups, except for Lyso-PC (18:0), PC (14:0), and PI (16:0). Aside from PC (16:0, 18:0, 18:0/18:1) and PE (16:0,18:0), other phospholipids showed significant differences between the EX and HT groups. Excluding Lyso-PC (18:1,18:0), PE (18:0,18:0/18:1), PS (18:1), and PG (18:0/18:1), phospholipids displayed significant differences between the PN and EX groups.
Variable PN (n=62) EX (n=105) HT (n=50) P Male (%) 100 100 100 1.000 Age (years) 45.03±3.30 45.16±3.14 46.64±6.66 0.084 BMI (kg/m2) 24.01±2.70 23.62±2.13 24.16±2.62 0.371 Duration of exposure (years) 10.00 (7.00,12.25) 5.81 (4.47,7.21) − <0.001 Smoking (yes, %) 26 (41.9) 48 (45.7) 25 (50.0) 0.695 Drinking (yes, %) 40 (64.5) 66 (62.9) 34 (68.0) 0.822 Chronic disease (yes, %) 11 (17.7) 10 (9.5) 6 (12.0) 0.297 FEV1 (predicted %) 91±11.51 93.22±12.37 − 0.595 FEV1/FVC (%) 88.32±6.79 87.00±7.11 − 0.560 MMEF (L/S) 85.32±24.42 82.35±21.91 − 0.650 MEF75% (predicted %) 73.05±22.55 69.73±21.55 − 0.445 MEF50% (predicted %) 76.92±22.69 75.80±20.49 − 0.839 MEF25% (predicted %) 85.23±31.71 81.25±27.83 − 0.554 Note: “−” Lung function tests were not conducted for the HT group; "predicted" The predicted value in lung function testing; "±" The range of standard deviation.
Abbreviation: PN=patients with pneumoconiosis (PN group); EX=dust-exposed workers (EX group); HT=healthy individuals (HT group); BMI=body mass index; FEV1=forced expiratory volume in one second; FEV1/FVC=ratio of forced expiratory volume in one second to forced vital capacity; MMEF=maximum mid-expiratory flow; MEF75%=maximum expiratory flow at 75% of vital capacity; MEF50%=maximum expiratory flow at 50% of vital capacity; MEF25%=maximum expiratory flow at 25% of vital capacity.Table 1. Characteristics of subjects.
Phospholipid PN EX HT Lyso-PC (16:0) 54.324 (45.654, 64.642)*† 32.926 (27.371, 40.985)§ 62.401 (55.161, 71.883) Lyso-PC (18:1) 6.979 (4.665, 8.276)† 6.108 (4.065, 8.273)§ 4.497 (3.439, 7.125) Lyso-PC (18:0) 22.725 (14.433, 47.347)* 31.006 (24.933, 31.791)§ 22.085 (17.760, 25.959) PC (14:0) 0.058 (0.028, 0.090)* 0.106 (0.060, 0.191)§ 0.051 (0.031, 0.055) PC (16:0) 6.576 (5.679, 7.637)*† 3.856 (3.290, 4.687) 3.950 (3.399, 5.091) PC (18:0) 0.989 (0.802, 1.203)*† 0.686 (0.596, 0.934) 0.630 (0.487, 0.864) PC (16:0/18:1) 34.978 (28.596,42.964)*† 15.347 (12.679, 19.452)§ 19.362 (16.214, 22.895) PC (18:0/18:1) 23.470 (13.399, 38.674)*† 33.208 (26.150, 46.561) 35.626 (26.832, 44.475) PE (16:0) 0.012 (0.005, 0.018)*† 0.019 (0.015, 0.027) 0.024 (0.017, 0.031) PE (18:0) 0.579 (0.449, 0.750)† 0.516 (0.361, 0.073) 0.448 (0.183, 0.749) PE (18:0/18:1) 1.616 (1.167, 2.290)† 1.393 (0.980, 2.102)§ 1.010 (0.723, 1.943) PI (16:0) 0.063 (0.042, 0.084)* 0.120 (0.040, 0.175)§ 0.027 (0.021, 0.041) PI (16:0/18:1) 0.746 (0.513, 1.109)*† 0.319 (0.218, 0.432)§ 0.206 (0.144, 0.266) Lyso-PS (18:0) 0.055 (0.038, 0.109)*† 0.151 (0.062, 0.264)§ 0.196 (0.120, 0.437) PS (16:0) 0.008 (0.005, 0.011)*† 0.012 (0.008, 0.018)§ 0.008 (0.004, 0.011) PS (18:1) 0.030 (0.024, 0.037)† 0.027 (0.016, 0.046)§ 0.014 (0.007, 0.027) PG (16:0) 0.137 (0.114, 0.170)*† 0.067 (0.046, 0.085)§ 0.028 (0.023, 0.035) PG (18:0/18:1) 0.159 (0.121, 0.194)† 0.148 (0.115, 0.179)§ 0.066 (0.052, 0.093) Abbreviation: PN=patients with pneumoconiosis (PN group); EX=dust-exposed workers (EX group); HT=healthy individuals (HT group); Lyso-PC=lyso-phosphatidylcholine; PC=phosphatidylcholine; PE=phosphatidylethanolamine; PI=phosphatidylinositol; Lyso-PS=lyso-phosphatidylserine; PS=phosphatidylserine; PG=phosphatidylglycerol.
* q<0.05 between PN and EX group.
† q<0.05 between PN and HT group.
§ q<0.05 between EX and HT group.Table 2. Quantitative values of phospholipids in each group [median (25th, 75th percentile) mg/L].
-
A total of 22 phospholipids were quantified. After removing data with > 30% missing values, 18 phospholipids were analyzed. The remaining missing values were imputed using the detection limit divided by √2. Principal component analysis (PCA) was used to evaluate significant overall differences in phospholipids among the three groups (Figure 1AB). PCA successfully separated the PN group from the other two groups but did not fully distinguish them. Partial least squares discriminant analysis (PLS-DA) revealed a distinct separation of serum phospholipid metabolism profiles between the PN and HT groups (Figure 1C– with R2Y=0.924, Q2Y=0.915) and between the PN and EX groups (Figure 1E–F, with R2Y=0.922, Q2Y=0.902). Scatter plots of R2Y and Q2Y values for the actual and simulated models after random permutation (
Supplementary Figure S1 ) demonstrated no overfitting.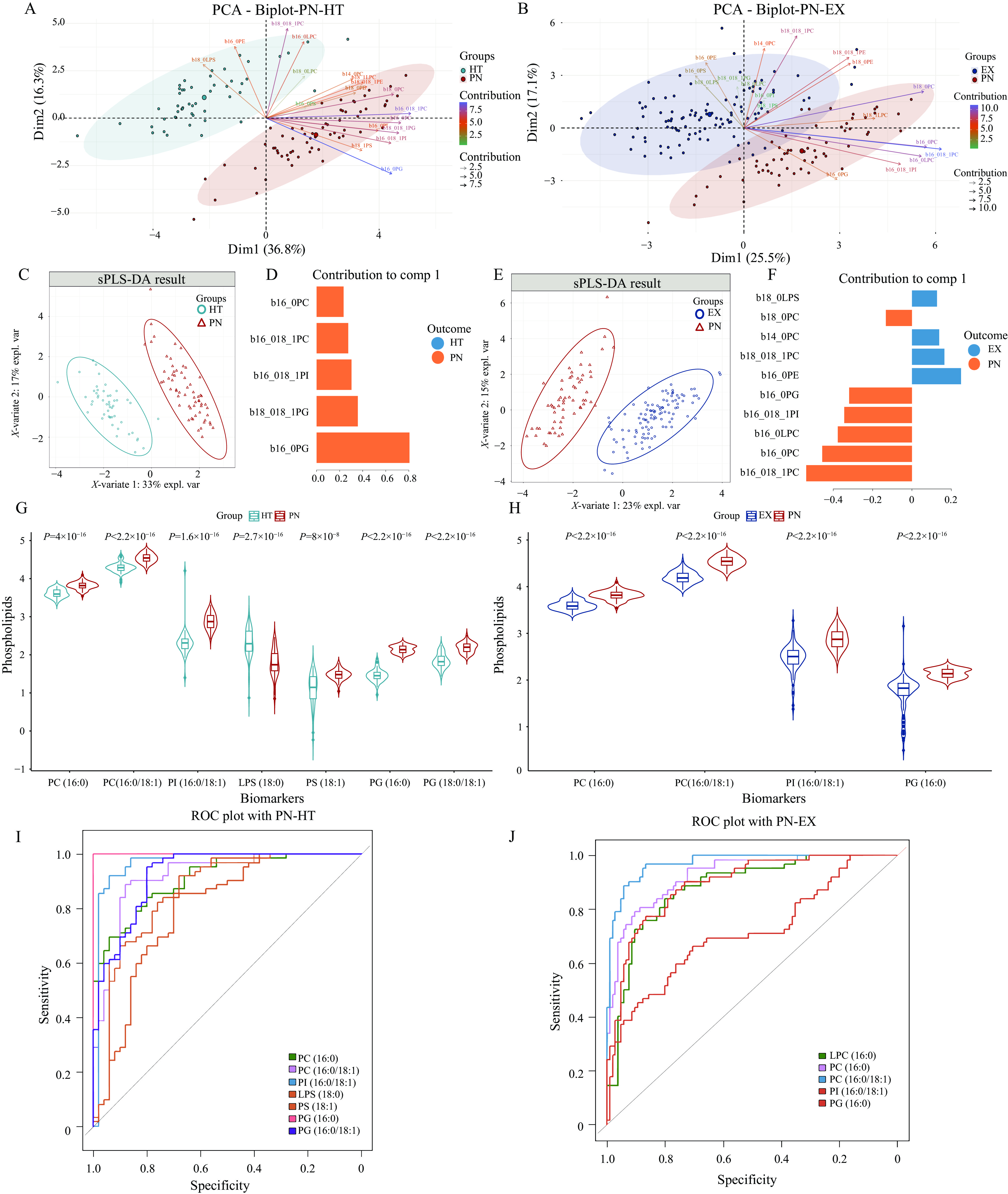 Figure 1.
Figure 1.The results of univariate and multivariate analyses between two groups. (A) PCA mode between the PN and HT groups. (B) PCA model between the PN and EX groups. (C) PLS-DA results for the PN and HT groups, with R2Y=0.924, Q2Y=0.915. (D) Principal component contribution to differentiate between PN and HT group. (E) PLS-DA results for the PN and EX group, with R2Y=0.922, Q2Y=0.902. (F) Principal component contribution to differentiate between PN and EX group. (G) Violin plot showing differential phospholipids in the PN and HT groups. (H) Violin plot showing differential phospholipids in the PN and EX groups. (I) ROC curve for differential phospholipids in the PN and HT groups. (J) ROC curve for differential phospholipids in the PN and EX groups.
Abbreviation: PN=patients with pneumoconiosis (PN group); EX=dust-exposed workers (EX group); HT=healthy individuals (HT group); PC=phosphatidylcholine; LPC=lyso-phosphatidylcholine; PI=phosphatidylinositol; LPS=lyso-phosphatidylserine; PS=phosphatidylserine; PG=phosphatidylglycerol; CWP=coal worker's pneumoconiosis; PCA=principal component analysis; ROC=receiver operating characteristic. -
In this study, we screened for metabolite differences between groups using univariate and multivariate statistical analyses (
Supplementary Tables S1–S2 ). Based on a q<0.05, FC>1.2, and VIP>1, we identified five phospholipids that differed significantly between the EX and HT groups: lyso-PC (16:0), PC (14:0), PS (18:1), PG (16:0), and PG (18:0/18:1). These were generally higher in the EX group than in the HT group.Furthermore, eight distinct phospholipids were identified when comparing the PN and HT groups, and their potential to discriminate between CWP patients and healthy individuals was verified using receiver operating characteristic (ROC) curve analysis. These phospholipids included PC (16:0), PC (16:0/18:1), PI (16:0/18:1), Lyso-PS (18:0), PS (18:1), PG (16:0), and PG (18:0/18:1), with AUCs and sensitivities greater than 0.7. Violin plots illustrated the distribution of these potential biomarker levels by group. Except for Lyso-PS (18:0), which showed a decrease, the levels of the other differential phospholipids all exhibited elevation in the PN group (Figure 1G, 1I).
To differentiate patients with pneumoconiosis from exposed individuals, ROC curves were analyzed for seven differential phospholipids after filtering with the established criteria. Among these, Lyso-PC (16:0), PC (16:0), PC (16:0/18:1), PI (16:0/18:1), and PG (16:0) exhibited good results. All differential phospholipids were consistently higher in the pneumoconiosis group than in the exposed group (Figure 1H, 1J).
-
To seek clues for early diagnostic biomarkers, it is necessary to distinguish phospholipid alterations occurring during the dust-exposure period from those present when the criteria for pneumoconiosis are met. In comparing the PN with the HT and EX groups, PC (16:0), PC (16:0/18:1), PI (16:0/18:1), and PG (16:0) were common differential metabolites with a consistent direction of regulation (Figure 2A). As this study is a preliminary investigation, we developed a support vector machine (SVM) model between the PN and EX groups to enhance discriminative power, selecting the four overlapping phospholipids as potential biomarkers. We assessed the model’s generalization ability using ten-fold cross-validation, randomly dividing the subjects into 10 groups, with nine serving as validation sets and one as the training set. As shown in Figure 2B, the model demonstrated highly satisfactory efficacy metrics. The mean values for AUC, sensitivity, specificity, and accuracy were 0.956, 0.934, 0.783, and 0.911, respectively. This combination is more effective at distinguishing between groups than most individual phospholipids.
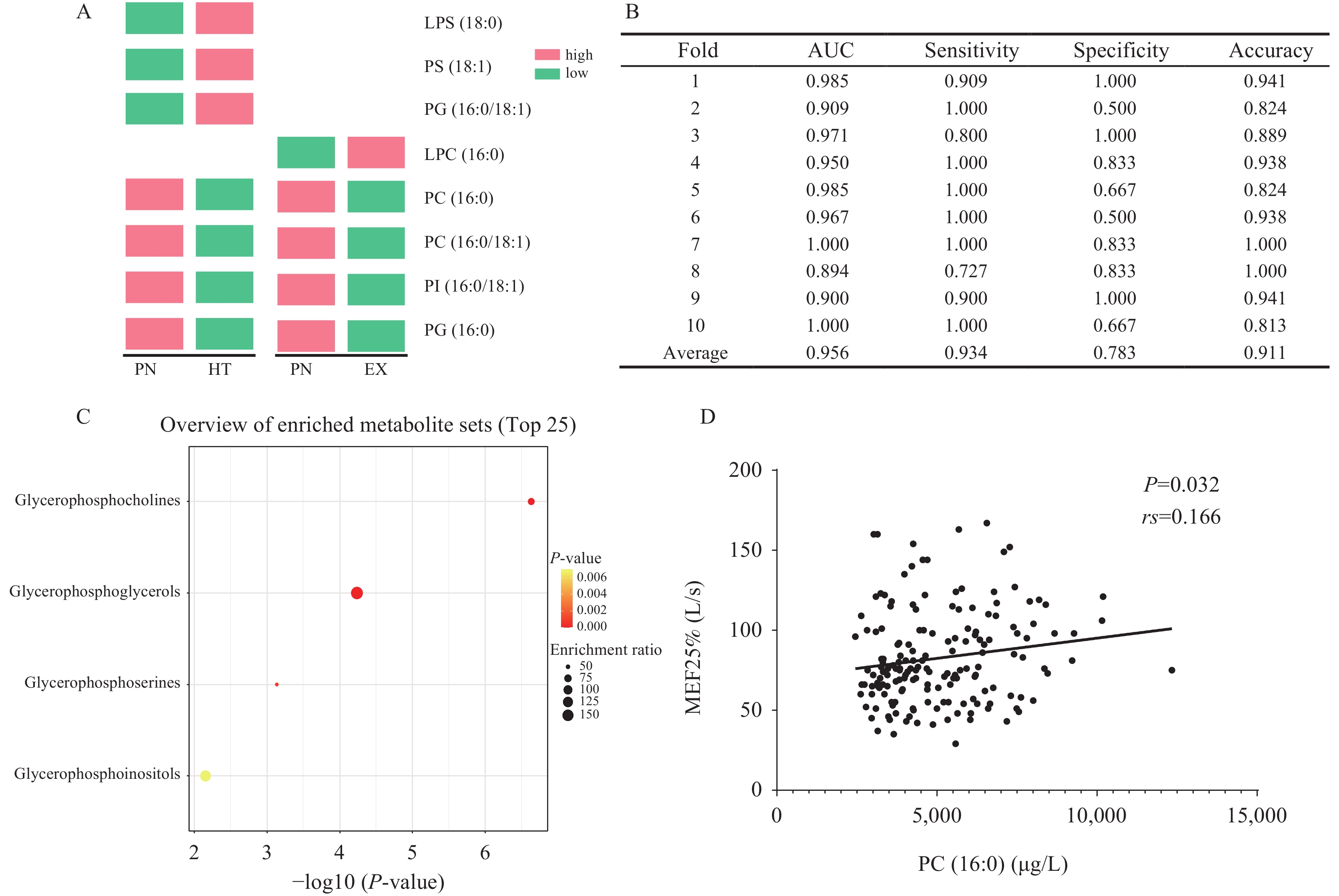 Figure 2.
Figure 2.Validation of differential phospholipids as potential biomarkers for pneumoconiosis. (A) Regulation of overlapping phospholipids. (B) Ten-fold cross-validation for potential biomarkers. (C) Pathway enrichment analysis of differential phospholipids. (D) Scatter plot illustrating the correlation between PC (16:0) and pulmonary function.
Abbreviation: PN=patients with pneumoconiosis (PN group); EX=dust-exposed workers (EX group); HT=healthy individuals (HT group); LPS=lyso-phosphatidylserine; PS=phosphatidylserine; LPC=lyso-phosphatidylcholine; PC=phosphatidylcholine; PI=phosphatidylinositol; PG=phosphatidylglycerol; AUC=area under the curve; MEF25%=maximum expiratory flow at 25% of vital capacity. -
As shown in Figure 2C, four pathways were identified, with the majority enriched in glycerophosphocoline metabolism. Figure 2D illustrates that only PC (16:0) was positively correlated with MEF25% (L/s), although the correlation coefficients were modest.
-
In this study, we applied our team’s UPLC-MS/MS phospholipid-targeted quantification method to investigate CWP. Unlike previous untargeted metabolomics studies, this targeted approach provided precise phospholipid quantification, offering specific insights into CWP-associated metabolic changes. Our findings showed that coal dust exposure significantly altered serum phospholipids, with variations effectively distinguishing patients with CWP. PC, PI, Lyso-PS, PS, and PG differentiated the PN and HT groups, while Lyso-PC, PC, PI, and PG distinguished the PN and EX groups. A model including PC (16:0), PC (16:0/18:1), PI (16:0/18:1), and PG (16:0) demonstrated strong discriminatory power between coal dust-exposed individuals and patients with CWP, suggesting these lipids as potential early diagnostic biomarkers and providing a valuable reference for auxiliary diagnosis. These phospholipids were primarily involved in glycerophospholipid metabolism and could serve as reliable biomarkers for pneumoconiosis if their biological roles are confirmed.
Lipids are a significant component of lung surfactant, and phospholipids, particularly PC, are the major constituents (8-9). Research has demonstrated a pivotal role for PCs in the inflammatory response. Studies, including our own, have revealed an association between elevated PC levels and coal dust exposure. Phospholipase A2 hydrolyzes PC to produce lyso-PC, which plays an important role in the onset and progression of inflammation and is potentially associated with pulmonary fibrosis. Lyso-PC metabolism via phospholipase A2 (10) or autotaxin (11) in bronchial epithelial cells or macrophages is implicated in pulmonary fibrosis. These findings suggest that alterations in PC and lyso-PC metabolism may contribute to lung fibrosis development.
PG has been implicated in the anti-inflammatory process. Consistent with other studies (12), PG levels were elevated at earlier time points and remained elevated in comparisons between pneumoconiosis patients and dust-exposed individuals. Therefore, we considered the potential for PG to serve as an early biomarker. PI-associated endoplasmic reticulum stress (13) and the downstream PIP3-AKT pathway (14) have also been implicated in pulmonary fibrosis.
Our findings indicate that the identified potential biomarkers are primarily associated with the glycerophosphorylcholine (GPC) pathway. GPC binding to aldehydes induces macrophage apoptosis, leading to airway damage and inflammation (15). However, no published studies have investigated GPC metabolism in CWP. Therefore, further research is warranted.
This study has some limitations. First, the sample size for each group was relatively small, and no validation set was used for sample verification. Future studies will expand the sample size to verify these findings. Second, this study did not consider the potential impact of dietary habits on metabolic profiles. However, because all participants reside in the same region and are predominantly local, their dietary and lifestyle habits are likely very similar. Third, the range of phospholipids examined in this study was limited. Expanding the number of targeted phospholipid species in future studies would broaden the scope and further screen for potential lipid biomarkers for pneumoconiosis. Furthermore, additional functional validation studies on these phospholipids would help identify biomarkers for coal worker’s pneumoconiosis.
HTML
Study Subjects and Sample Collection
Detection of Lipidomics in UPLC-MS/MS
Statistical Analysis
Characteristics of Subjects
Changes in Serum Phospholipids
Differential Metabolite Screening
Cross-Validation for Potential Biomarkers
Enrichment Analysis of Differential Phospholipids and Correlation Analysis with Lung Function.
| Citation: |

|