
 Download:
Download:




-
Rubella is a highly contagious viral illness characterized by fever, rash, and lymphadenopathy, typically occurring among unvaccinated children and young adults (1-2). Clinical manifestations are generally mild and self-limiting; however, infection during pregnancy, especially in the first trimester, can cause fetal infection, resulting in miscarriage, stillbirth, or congenital rubella syndrome (CRS). CRS is characterized by a constellation of malformations, including hearing impairment, congenital heart defects, and eye anomalies (3-4).
In 2004, rubella became a notifiable infectious disease reportable to China’s National Notifiable Diseases Reporting System (NNDRS). In 2014, rubella surveillance was integrated into the case-based, laboratory-supported Measles Surveillance System (MSS) (5). As the surveillance system improved, the sensitivity and specificity of rubella detection increased, and surveillance quality indicators were routinely met.
High rubella-containing vaccine (RCV) coverage is essential for eliminating rubella and preventing CRS. RCV was licensed in China in 1993 and introduced nationwide into the Expanded Program on Immunization (EPI) in 2008 in response to the World Health Organization’s (WHO) goal of rubella elimination (5). The Western Pacific Regional Committee endorsed the “Regional Strategy and Plan of Action for Measles and Rubella Elimination in the Western Pacific” and urged Member States to eliminate rubella as soon as possible (6). After RCV introduction in China, rubella incidence declined and is now approaching elimination.
Rubella epidemiology over 20 years of surveillance and 16 years of RCV inclusion and vaccination histories of cases were analyzed to estimate rubella incidence and trends, so as to understand the potential drivers of rubella incidence and identify remaining challenges in rubella control and elimination.
-
RCV vaccination data from 2008 to 2021 were obtained from the National Immunization Program Information Management System; rubella case data and incidence reported from 2004 to 2023 were obtained from NNDRS. All cases were confirmed rubella and included laboratory-confirmed, clinically compatible, and epidemiologically linked cases (case definitions are detailed in
Supplementary Table S1 ). The vaccination status of cases reported from 2014 to 2023 was obtained from MSS. Demographic data were extracted from the China Information System for Disease Control and Prevention. Data sources covered all 31 provincial-level administrative divisions (PLADs) in China [excluding Hong Kong Special Administrative Region (SAR), Macau SAR, China; and Taiwan, China]. -
Descriptive statistics were used to describe RCV coverage during 2008–2021, annual incidence during 2004–2023, and the distribution of vaccination status of cases. Joinpoint regression was used to estimate rubella incidence trends by sex and age group during 2004–2023 and to identify segment trends and turning points (7). Age was divided into nine age groups (0–9 years, 10–19, 20–29, …, 70–79, and ≥80 years). Annual percent change (APC), average annual percent change (AAPC), and corresponding 95% confidence intervals (CIs) described incidence trends. AAPC was used to describe trends during the study period; APC was used to describe trends in each segment. Analyses were performed with the Joinpoint Regression Program (version 5.0.2, National Cancer Institute, Bethesda, MD, USA). P<0.05 was considered statistically significant.
-
There were 584,758 rubella cases reported during 2004–2023; annual incidences are shown in Figure 1. Rubella incidence was 18.5 per million population in 2004 and increased rapidly, reaching a peak of 91.1 per million population in 2008. From 2009 to 2017, the annual incidence trended downward from 52.6 to 1.2 per million population, although there was a peak of 48.9 per million population in 2011. During a resurgence in 2019, incidence increased to 23.3 per million population, subsequently decreasing to 1.6 per million population in 2020. During 2021–2023, the incidence fell below 1.0 per million population, reaching a historic low of 0.4 per million population in 2023.
 Figure 1.
Figure 1.Rubella incidence and routine immunization coverage from 2004 to 2023.
Abbreviation: NNDRS=National Notifiable Diseases Reporting System; EPI=Expanded Program on Immunization; MSS=M easles Surveillance System.RCV was introduced nationwide in 2008. Figure 1 shows RCV coverage from 2008 to 2021. Coverage was lowest in the first year of RCV inclusion: 51.5% for the first dose and 39.0% for the second dose. The vaccination rate gradually increased in subsequent years. First-dose RCV coverage fluctuated and declined to 62.1% in 2010, from 68.1% in 2009, then gradually increased and remained stable. By 2012, two-dose vaccine coverage stabilized at 95% or greater.
-
Figure 2A shows joinpoint analysis results by sex for 2004–2023. For males, the incidence initially increased, peaked in 2008 (APC2004–2008=59.52%, P<0.05), and then decreased (APC2008–2016=−29.74%, P<0.05). A subsequent increase and decrease peaked in 2019 (APC2016–2019=54.28%, P>0.05; APC2019–2023=−75.60%, P<0.05). For females, there was one joinpoint in 2008 (APC2004–2008=46.45%, P<0.05; APC2008–2023=−19.37%, P<0.05). During the study period, the AAPC showed decreasing trends (AAPCmale=–24.33%, P<0.05; AAPCfemale=−8.58%, P<0.05).
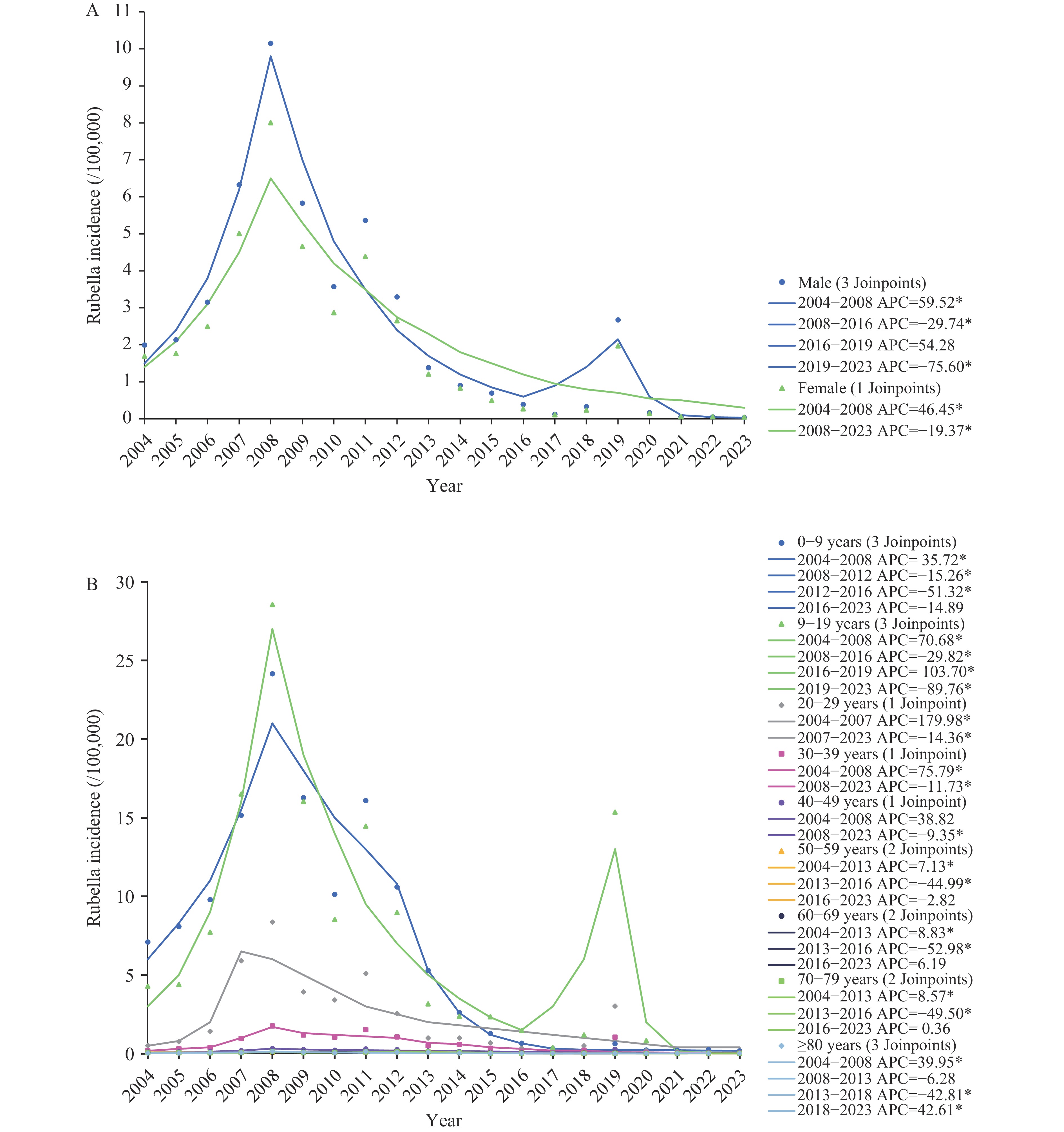 Figure 2.
Figure 2.Temporal trends of rubella incidence from 2004 to 2023. (A) Temporal trend of rubella incidence by sex; (B) Temporal trend of rubella incidence by age group.
Abbreviation: APC=annual percentage change.
* P<0.05.
Figure 2B shows age group analyses. Age group trends were similar to overall trends. Starting in 2004, rubella incidence increased in all age groups but decreased after 2008. There were statistically significant incidence decreases in the 0–9, 10–19, 50–59, 60–69, and 70–79 year age groups during the entire study period, with AAPCs of –16.60%, –33.24%, –6.98%, –5.54%, and –6.79%, respectively. Among all age groups, decreases among 0–9-year-olds and 10–19-year-olds were most prominent. Unlike the monotonic and sustained decline in the 0–9 year age group after 2008 (APC2008–2012=–15.26%; APC2012–2016=–51.32%; APC2016–2023=–14.89%), a peak appeared in 2019 in the 10–19 year age group (APC2008–2016=–29.82%; APC2016–2019=103.70%; APC2019–2023=–89.16%).
For total rubella incidence, there was a statistically significant joinpoint in 2008 (APC2004–2008=47.12%, P<0.05; APC2008–2023=–18.95%, P<0.05), and AAPC showed decreasing trends (AAPC=–8.11%, P<0.05). The APC and AAPC values for each group and each period are shown in
Supplementary Table S2 andSupplementary Table S3 . -
Rubella vaccination status was included in the case-based surveillance system in 2014. As Figure 3 shows, 75.25% of rubella cases 8 months or older were unvaccinated or had unknown vaccination status; 0.07% had 1 dose; 18.01% had ≥2 doses. The percentage of cases with zero or an unknown number of RCV doses was highest in 2014 (84.18%) and lowest in 2022 (53.33%). Among 8-month-to-9-year-olds, the percentage with zero or an unknown number of RCV doses decreased from 74.83% in 2014 to 8.43% in 2023. Among 10-to-19-year-olds and those ≥20 years old, zero or unknown RCV dose rates were above 50% and 90%, respectively. The number of rubella cases reported in 2019 was the highest reported in the most recent 10 years, with 10-to-19-year-olds accounting for most (67.3%) of the reported cases that year, and with a 77.8% rate of zero or an unknown number of RCV doses.
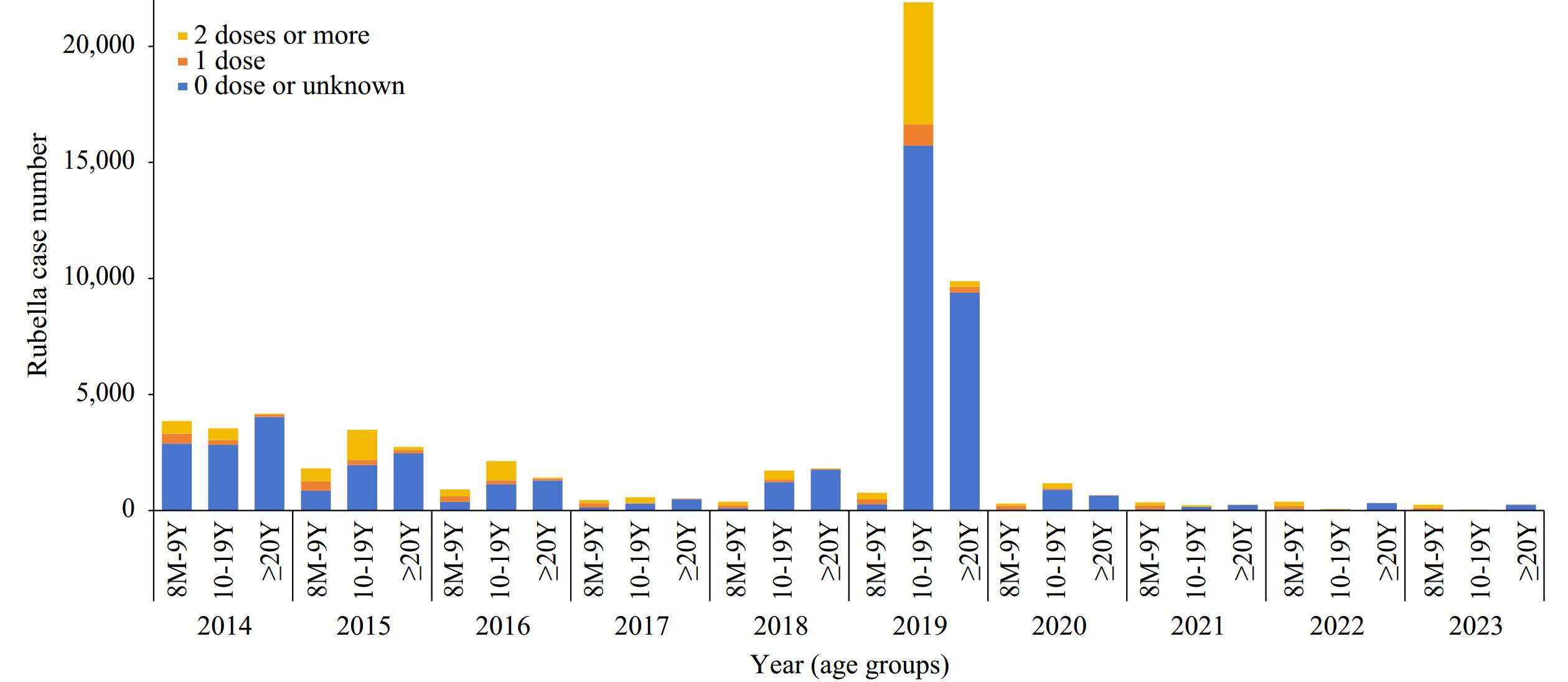 Figure 3.
Figure 3.Rubella vaccination status of rubella cases from 2014 to 2023.
-
This study used surveillance data from the 20 years since rubella’s inclusion in the NNDRS and the 10 years since its inclusion in the MSS, and vaccination data from the 16 years since nationwide rubella vaccination promotion, to comprehensively assess progress toward rubella control and elimination in China from both epidemiological and immunization strategy perspectives.
After rubella was included in the NNDRS, strengthening the surveillance system and improving its sensitivity led to an initial increase in reported rubella cases. After rubella was subsequently included in the MSS, surveillance sensitivity further improved and met WHO requirements (8). In 2008, China included RCV in the EPI, with the measles-rubella vaccine administered at 8 months and the measles, mumps, and rubella (MMR) vaccine at 18 months (5). Initially, low RCV uptake due to vaccine shortages impeded the decline in rubella incidence, indicating a cumulative susceptible population and a high risk of rubella, likely contributing to a resurgence of cases in 2011. Coverage stabilized above 95% by 2012, and the number of rubella cases decreased markedly, reaching its lowest annual level by 2023. Joinpoint analysis showed that 2008 was an inflection point for incidence in both males and females. Decreases were most pronounced in the 0–9-year-old RCV target population, demonstrating direct vaccine protection. Decreases in non-RCV target age groups demonstrated indirect vaccine protection (9).
It is important to note that while incidence declined after nationwide RCV inclusion, a significant rubella resurgence occurred in 2019. This case increase coincided with a rise in rubella-related public health emergencies. In 2019, 187 public health emergencies were reported nationwide, involving 7,032 cases (10). During 2018–2019, coincident with the resurgence, the rubella virus genotype shifted from lineage 2B-L1 to lineages 1E-L2 and 2B-L2c (11). Joinpoint analysis revealed that incidence increased most among 10–19-year-olds, with a statistically significant joinpoint in this age group. Analysis of rubella case vaccination status demonstrated that the largest number of 2019 cases occurred among 10–19-year-olds, most of whom had zero or an unknown number of RCV doses. Affected individuals were born before 2008 and lacked protective immunity due to the combination of no RCV vaccination and no rubella exposure, given the low rubella incidence (5). As students, they were active and in close quarters. This immunity gap may have facilitated a rubella increase spread by both indigenous and imported rubella virus (10,12-13). Concerningly, this age group is entering or has entered reproductive age, posing a risk of CRS (5,14-15).
Eliminating and controlling rubella and preventing CRS depends on high-quality surveillance and effective immunization strategies. Therefore, strengthening sensitive rubella detection (16) and establishing CRS surveillance to augment rubella surveillance is critically important. Meanwhile, promoting vaccination can effectively reduce CRS occurrence (5,17). Rubella vaccination has been comprehensive and effective in China. In addition to maintaining high routine immunization coverage among children, unvaccinated, rubella-susceptible individuals, especially seronegative, non-pregnant young women, are also a key target population. However, joinpoint analysis by sex revealed an inflection point in 2008 for both sexes and another in 2019 for males, suggesting that male cases contributed to rubella transmission. Therefore, emphasizing the importance of rubella and CRS prevention for both women and men is crucial to reducing circulation risk. Vaccination should target the entire population, not just women. PAHO’s success in eliminating rubella was based on accelerated campaigns among 5–39-year-olds and follow-up campaigns every four years among 1–4-year-olds. Several countries followed PAHO’s lead by conducting supplemental immunization activities (SIAs) in children up to 15 years of age or older. For China, combined with the goal of measles elimination, targeted catch-up MMR vaccination can be conducted in middle schools and universities to consolidate rubella immunity. However, considering that women of childbearing age are directly associated with CRS occurrence, unvaccinated women of childbearing age should be advised to receive one dose of rubella vaccine at least three months before pregnancy.
This study has limitations. First, detailed analyses of surveillance system quality indicators were not conducted, precluding adjustment for surveillance sensitivity. Second, regional analyses, which could identify consistently high-risk areas requiring intervention, were not performed. Third, the identification and characterization of the immunization gap were based on epidemiological and vaccination data. More conclusive evidence could be obtained by identifying gaps in population immunity through serological surveys.
This study has three fundamental conclusions. First, China’s rubella surveillance system gradually improved, and now it detects rubella cases sensitively. Second, rubella vaccination has had a major positive impact on the prevention and control of rubella in China, directly protecting the vaccinated age group and indirectly protecting unvaccinated age groups. Third, the 2019 rubella resurgence exposed an immunity gap among adolescents that warrants close monitoring. Targeted measures should be implemented to address this immunity gap among adolescents and young adults. Targeted catch-up vaccination of susceptible populations and maintaining high surveillance sensitivity are essential to achieve and sustain rubella elimination.
HTML
Data Sources
Statistical Analysis
Rubella Cases, Incidence, and Routine RCV Coverage
Temporal Trends
Vaccination Status of Cases
| Citation: |

|