 DownLoad:
DownLoad:
 Download:
Download:




-
An in-depth analysis of the correlation between cereal consumption and type 2 diabetes (T2D) risk has significant implications for public health, particularly in nations where staples include white rice and wheat products and where the incidence of T2D is rising. Dietary cereal intake in China is dynamic and changes over time. Thus far, no longitudinal study has been conducted to identify trajectories of cereal intake within the Chinese population or to investigate the secular trend of cereal consumption with T2D risk. This study incorporated data from 4,464 adults 18 years and above, sourced from seven distinct waves of the China Health and Nutrition Survey (CHNS) from 1997 to 2018. A group-centric multi-trajectory modeling approach was employed to discern cereal-intake trajectories (individual trajectories for rice, wheat, and other grains intake and multi-trajectories of overall cereal-intake patterns) across 21 years. To examine the correlation between cereal intake and T2D risk, multivariate Cox proportional hazard and restricted cubic spline (RCS) models were employed. Four distinct multi-trajectory groups of cereal intake, identified from 1997 to 2018 within the Chinese population, were associated with varying levels of T2D risk. Compared to the group with “balanced cereal intake”, a higher subsequent risk of T2D was noted in the group with “high white rice intake without other grains”. Notably, daily intakes of white rice exceeding 240 grams for men and 280 grams for women could potentially act as threshold points for T2D development.
T2D continues to pose a significant public health issue worldwide. In the past few decades, China has witnessed an incremental rise in T2D prevalence, with an adult ratio of 11.2% between 2015 and 2017, exemplifying a stark public health quandary (1). Previous epidemiological studies have suggested an increased risk of T2D linked with consuming refined grains, such as white rice. In contrast, whole grains pose a reduced risk (2-5). However, these studies primarily used single time point assessments for dietary exposure.
Moreover, dietary data were either partially available or absent in each follow-up round. Limited studies have explored the potential impact of long-term cereal intake trends and their subsequent changes while considering the heterogeneity of the population. Traditional Chinese grain classifications typically comprise rice, wheat, and other grain varieties. Understanding the long-term intake trajectories of these specific cereal subtypes is crucial for assessing the risk of T2D, especially in a nation like China where cereals contribute to nearly half of the total energy intake and T2D incidence is rapidly rising.
The present analysis uses data from seven waves (1997 to 2018) of the CHNS. An exploration of the long-term trajectories of cereal intake was conducted, designating the period from 1997 to 2018 as the “track identification period.” A potential confounder, changes in diet following the development of T2D, was mitigated by using dietary information obtained prior to the diagnosis of T2D in prospective analyses. However, since fasting blood samples were only available from the waves of 2009, 2015, and 2018, our cohort analysis on the association between cereal intake and incident T2D is confined to these three waves, termed the “survival analysis period.”
This study selected participants aged 18 years or over who were neither pregnant nor breastfeeding and had participated in the surveys conducted in 2009, 2015, and 2018 (n=24,372). Participants with insufficient dietary data, abnormal daily energy intake, incomplete blood samples, or missing demographic information were excluded from the selection. Out of the remaining participants (n=19,499), those who were involved in at least two follow-up waves from 2009 to 2018 and were not diagnosed with T2D upon initially entering the “survival analysis period” were chosen (n=8,886). From this group, participants with fewer than three waves of available dietary data before being diagnosed with T2D were discarded. The final analysis also excluded individuals who reported having diabetes in the survey from 1997 to 2006 to ensure that all participants were non-diabetic upon commencement of the “survival analysis period.” Ultimately, 4,464 participants were included in the final analysis. Supplementary Figure S1 provides a flow chart that depicts the participant selection process for the present study. The survey was approved by the institutional review committees of the National Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention (No. 201524), and the informed consent forms were signed by all participants.
In this study, food consumption data was gathered via three consecutive 24-hour dietary recalls, which included two weekdays and one weekend day. The evaluation of cereal intake included the consumption of rice, wheat, and other grains. “Rice” was defined as white rice and its associated products, such as rice cakes and rice noodles. “Wheat” was categorized as refined wheat and its products, including white bread, noodles, and mantou (steamed buns). Lastly, “other grains” encompassed corn, barley, oats, millet, and similar grains. The average per capita daily intake of various foods and nutrients and total energy intake (TEI) were calculated, using the China Food Composition Table as a reference (6).
Fasting plasma glucose (FPG) and glycated hemoglobin A1c (HbA1c) were measured in surveys conducted in 2009, 2015, and 2018. T2D was defined, in accordance with the diagnosis criteria set by the World Health Organization and China’s guidelines (7-8), by fulfilling at least one of the three following conditions: a) FPG ≥7.0 mmol/L; b) HbA1c ≥6.5%; c) administration of diabetes treatments, such as oral hypoglycemic medications or insulin injections.
A population-based multi-trajectory model was applied to identify multiple consumption trajectories of rice, wheat, and others, distinguishing between males and females (9). Multi-trajectory modeling was executed utilizing a STATA plug-in, employing a continuous norming distribution for continuous data, with follow-up years serving as the timescale for these trajectories. The selection of the most suitable model adhered to strict statistical criteria: a) Models with a smaller Bayesian information criterion were regarded as superior fits; b) Each trajectory class encompassed at least 2% of the sample population; c) Average posterior probability of membership within each group with values exceeding 0.7 served as an indicator of adequate internal reliability; d) The odds of correct classification within each group were ascertained, with a recommended minimum ratio of 5 to 1 per group (10).
The risk of T2D concerning the trajectories was evaluated using the multivariate Cox proportional hazards regression model. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated accordingly. In the analysis, three models were created. Model 1 did not account for any covariates, whereas Model 2 included adjustments for lifestyle features and demographic characteristics. Model 3 was built upon Model 2 by adjusting for dietary factors such as initial rice/wheat/other grains intake, overall energy intake, waist circumference, and systolic blood pressure. In a supplemental analysis, potential dose-response relationships were scrutinized via an RCS. The relationship between continuous variable cereal intake and T2D risk was examined here. To accurately represent the participant’s long-term cereal consumption, the cumulative average of cereal intake was computed as a continuous variable, considering the period from the participant’s entry into the cohort to the point immediately before their T2D diagnosis. All analyses were conducted using SAS (version 9.4, SAS Institute, Inc., Cary, NC, USA), Stata 15SE (StataCorp, College Station, TX, USA), and R software (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was determined by a P-value of less than 0.05.
The analysis encompassed 4,464 participants, consisting of 2,044 males and 2,420 females, reflecting a fundamental gender balance. The mean age, with standard deviation (SD), was 42.23 (12.00) for males and 43.02 (11.31) for females. The baseline characteristics of the participants are delineated in Supplementary Table S1.
Cereal consumption was analyzed by gender. Figure 1 illustrates individual trajectories of rice, wheat, and other grain intake, with separate plots for males (Figure 1A, C, E) and females (Figure 1B, D, F). Four intake trajectories were identified in terms of rice and wheat consumption for both genders, namely: “low stability” (Group 1), “normal stability” (Group 2), “median decrease” (Group 3), and “high-level decline” (Group 4). In regards to other grains, three intake trajectories were noted in both genders: “no intake” (Group 1), “low increase” (Group 2), and “moderate fluctuation” (Group 3). Among the 4,464 participants, 422 (9.45%) developed T2D during follow-up, with the total person-years amounting to 33,659. In males, lower T2D risk was associated with other grain intake trajectories in Groups 2 and 3 as compared to Group 1, with an HR (95% CI) of 0.60 (0.45–0.81) for Group 2 and 0.52 (0.33–0.84) for Group 3. Similarly, in females, lower T2D risk was associated with Group 3’s other grain intake trajectory compared to Group 1 [HR=0.56 (0.34–0.90)]. See Supplementary Table S2 for the Cox proportional hazards analysis results exploring the association between cereal intake trajectories and T2D risk in males and females.
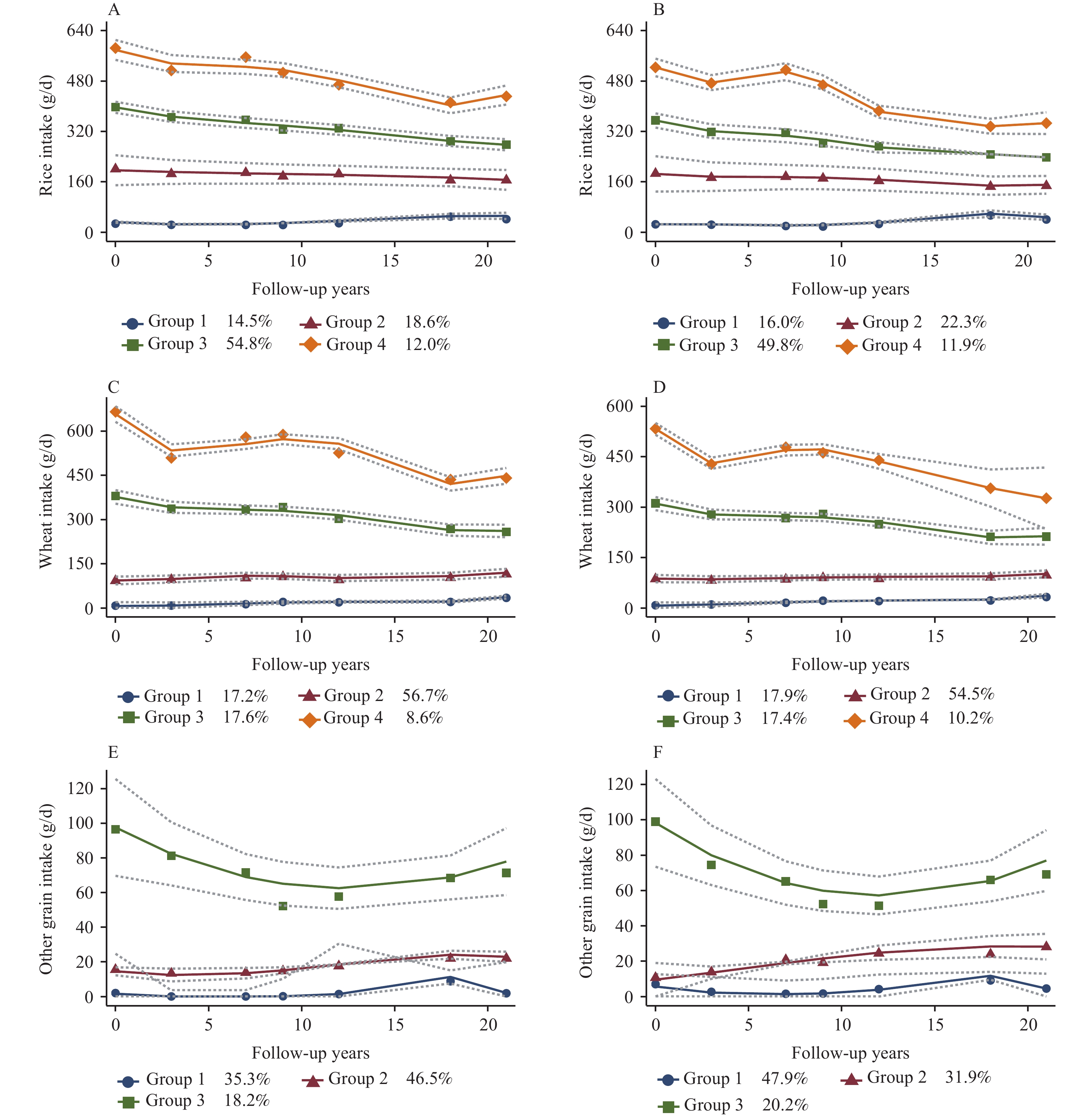 Figure 1.
Figure 1.Trajectory of rice, wheat, and other grain intake in China from 1997 to 2018 among male and female participants. (A) Rice among males; (B) Rice among females; (C) Wheat among males; (D) Wheat among females; (E) Other grain among males; (F) Other grain among females.
Note: The solid lines depict the average estimated intake of rice, wheat, and other grains over time, while the dashed lines represent 95% confidence intervals. The data points represented by dots are weighted based on each individual’s responses and the posterior probabilities of group membership. Cereal intake, measured in grams per average day, is shown on the vertical axis. The horizontal axis represents the follow-up time in years. The different colored lines correspond to distinct trajectory groups identified within the study population, with the legend indicating the groups and the proportion of people represented by each color.Four distinct gender-specific multi-trajectory patterns of cereal consumption (rice, wheat, and other grains) were identified (Figure 2): Group 1 (both genders) exhibited a decrease in very high rice intake, maintained low stable wheat intake, and exhibited deficient intake of other grains. Group 2 (both genders) showcased a decrease in high rice intake, moderate stable wheat intake, and deficient intake of other grains. Group 3 (men) and Group 4 (women) had a balanced cereal intake. In contrast, Group 4 (men) and Group 3 (women) displayed very low rice intake, a decrease in high wheat intake, and moderate intake of other grains.
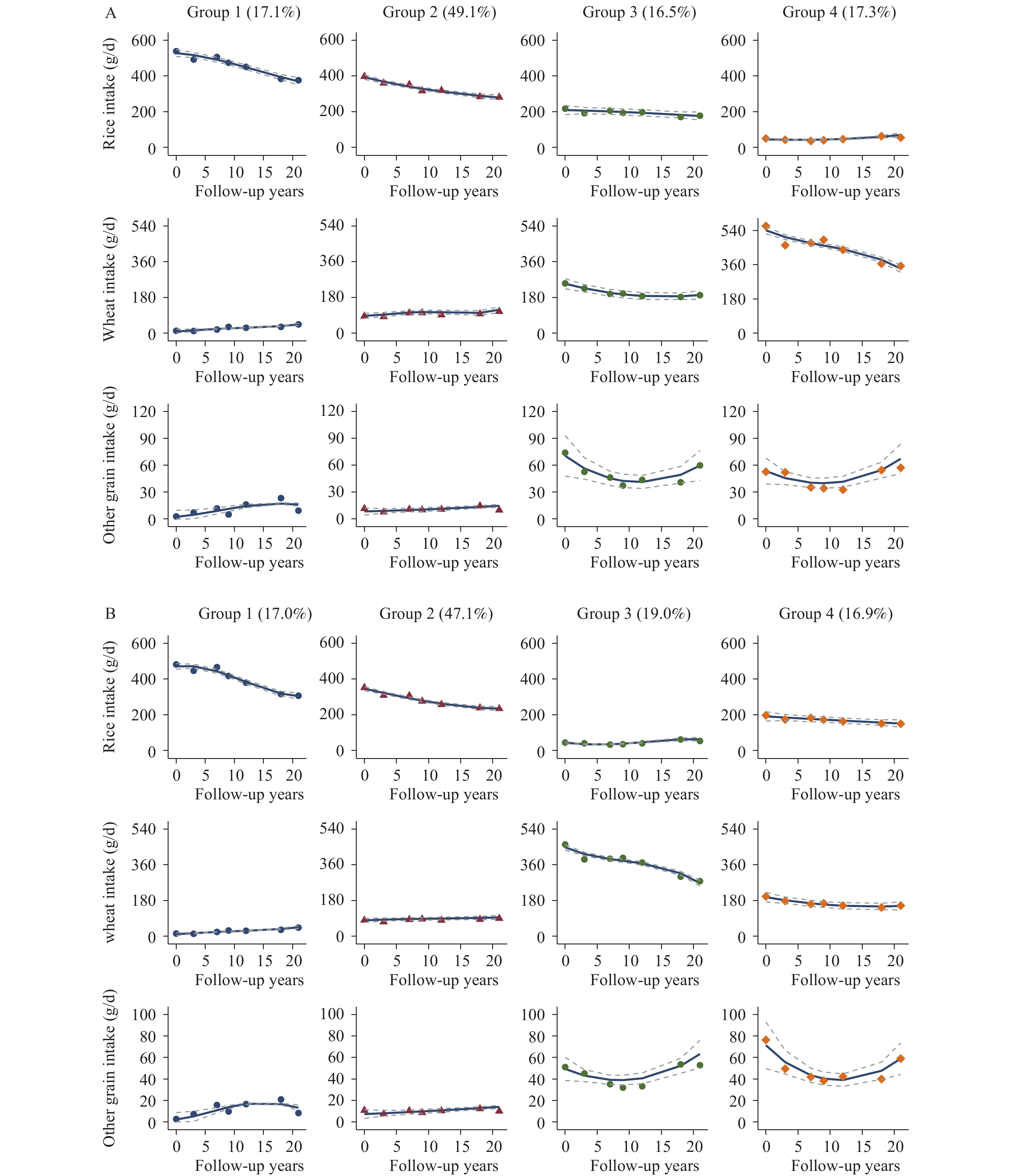 Figure 2.
Figure 2.Multivariate trajectories of rice, wheat, and other grain consumption among (A) males and (B) females in the Chinese population, 1997–2018.
Note: The solid lines within the graph depict the average estimated intake of rice, wheat, and other grains over time. The dashed lines, on the other hand, represent the 95% confidence intervals. The individual data points, represented by dots, are individually weighted based on the posterior probabilities associated with each group membership. On the vertical axis, cereal intake measurements (including intake of rice, wheat and other grains) are represented in grams per average day. The horizontal axis, however, denotes follow-up time measured in years. Various trajectory groups identified within the study population are represented with distinctive color lines. Each color set of lines illustrates the intake trajectory of rice, wheat, and other grains for the identified population. The legend provides corresponding group associations and the percentage of individuals within each group.In female Groups 1 and 2, characterized by a high white rice intake without other grains, the HRs (95% CIs) for T2D were 1.70 (1.01–2.85) and 1.56 (1.01–2.40), respectively, when compared with Group 4 (the “balanced cereal intake” group). Supplementary Table S3 indicates the average rice, wheat, and other grain intake among the different multi-trajectory groups for both males and females at follow-up. Our findings suggest that group-based multi-trajectory modeling is an effective tool for identifying cereal-intake trajectory groups.
The RCS analysis (Figure 3) indicated a statistically significant correlation and nonlinear relationship between cereal consumption and T2D risk (P<0.05). For men, a negative correlation was observed between rice intake (ranging from 100 to 280 grams/day) and T2D risk; however, risk increased when consumption exceeded 280 grams/day. A significant increase in T2D risk was noted for women when rice intake rose above 240 grams/day. Consumption of other grains, ranging between 20 and 100 grams/day, demonstrated a protective effect (HR<1) among women.
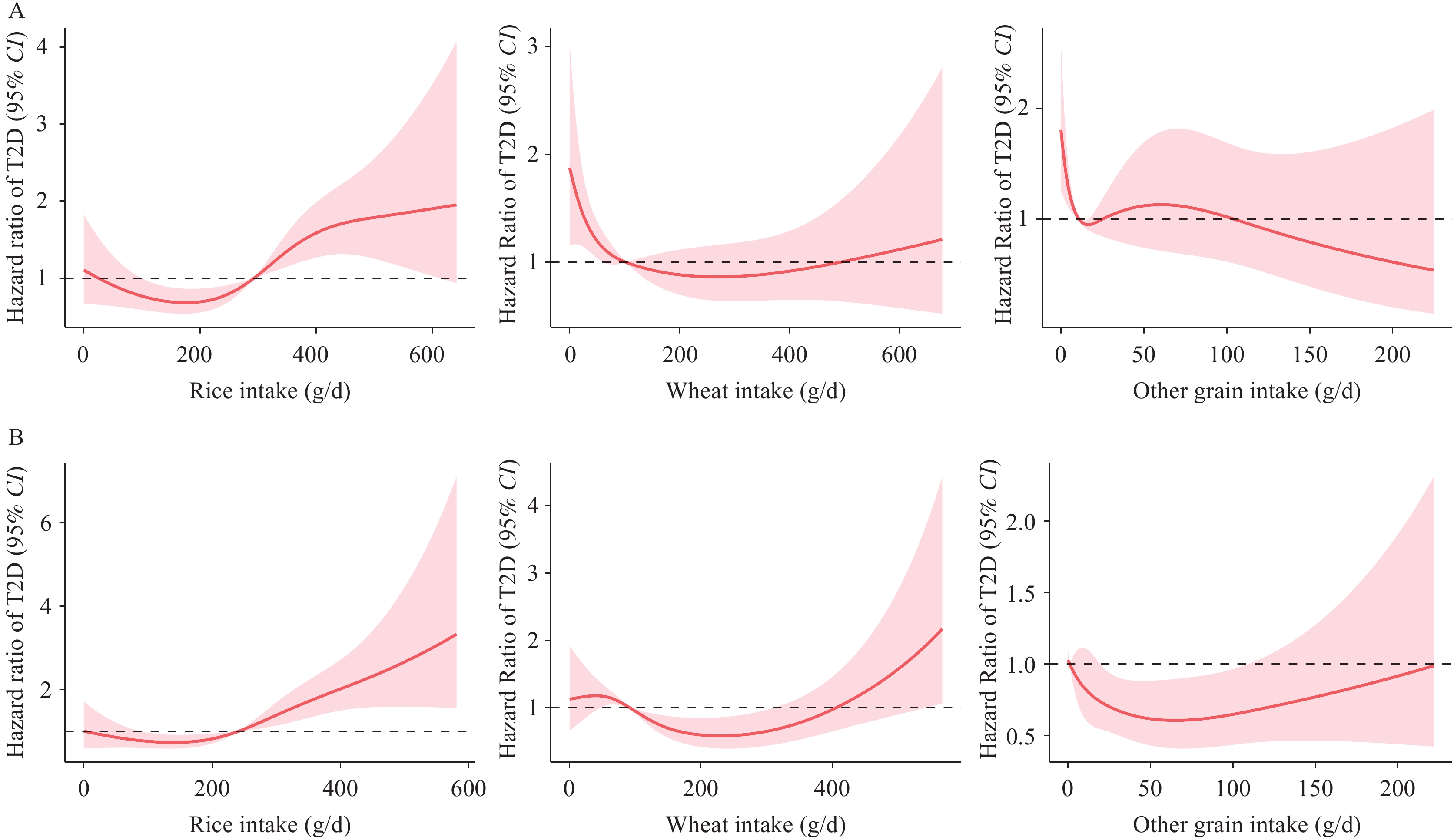 Figure 3.
Figure 3.Exposure-response relationships between intake of rice, wheat, or other grains and risk of type 2 diabetes as determined by adjusted Cox proportional hazards analyses with restricted cubic splines among (A) male and (B) female participants.
Note: The y-axis represents the logarithm of the hazard ratios obtained from the multi-variable Cox model. The adjusted hazard ratio pertaining to the risk of T2D is illustrated by the red line. The shaded area depicts the 95% CI of these adjusted hazard ratios.
Abbreviation: T2D=type 2 diabetes; RCS=restricted cubic spline; CI=confidence interval.
-
This cohort study involving Chinese adults examined the link between different consumption patterns of rice, wheat, and other grains and the risk of developing T2D. The research discovered that a balanced intake of cereals, particularly one characterized by a high consumption of white rice without the inclusion of other grains, corresponds to a heightened risk of developing T2D. On the contrary, a moderate intake of coarse grains is inversely related to this risk. However, the correlation between cereal consumption and T2D risk might diverge based on gender. Our study suggests that daily intake above 240 grams and 280 grams of white rice may be a threshold for T2D development in men and women, respectively. To the best of our knowledge, this is the first report detailing the evolution of cereal consumption in Chinese adults over a continuous 21-year period (1997–2018). This research is unique due to using a group-based trajectory model for partitioning cereal consumption into groups with similar changing features, enabling an investigation of the health outcomes associated with different cereal consumption patterns.
In China, the term “coarse grains” is typically used to refer to grains excluding refined rice and wheat products. Western diets more commonly incorporate whole grains, defined by a fiber-to-carbohydrate ratio equal to or greater than 0.1. Notably, an inverse correlation was identified for other grains, confirming an association across singular and multiple trajectories. Consistently aligning with prior studies on whole grain consumption, it was determined that trajectory groups consuming a specific volume of other grains exhibited a reduced risk of T2D compared to the “no/deficient intake group.” This conclusion is supported by a significant body of scholarly research.
No statistically significant associations were found between various trajectories of rice intake and the risk of T2D. Interestingly, however, the group that did not supplement their diet with rice but had a high white rice consumption, exhibited a higher T2D risk in the multi-trajectory analysis. A parallel observation was noted in a Japanese study, where a similar association between T2D risk and white rice consumption was discerned. Although participants with a higher rice intake tended to have a lower body mass index, according to this study, they nonetheless displayed a heightened risk of T2D. This suggests that other mechanisms besides obesity might increase T2D risk due to high rice intake (1). The underlying mechanism for high white rice consumption and increased T2D risk remains uncertain. One plausible explanation for this could be the higher glycemic index (GI) of white rice, a dietary staple in Asian populations, significantly contributing to the glycemic load (GL). Moreover, the processing of polished rice strips away beneficial nutrients such as dietary fiber and magnesium, which have been proven to mitigate diabetes risk.
Differences in basal metabolism, physical activity, and lifestyle exist between genders. From this study’s standpoint, we posit that cereals, serving as the primary source of carbohydrates and a significant contributor to GL, have a more pronounced influence on women than men. Our research findings support the view that cereal ingestion, encompassing rice and other grain consumption, has a more significant impact on T2D risk among women than their male counterparts. In our dose-RCS analysis, substantial distinctions were observed between men and women, with women’s intake of coarse grains in the quantity of 20–80 grams inversely correlated with T2D risk. Accordingly, we advocate for a more intensive investigation of women’s consumption behaviors and cereal intake patterns.
Products made from refined wheat, such as bread, white noodles, and steamed buns, vary considerably between Western and Asian countries. Although several studies have explored the relationship between the consumption of refined bread and the risk of T2D, the conclusions drawn from these studies are inconsistent. Compared to the extensive research on wheat consumption and the risk of obesity or being overweight, studies focusing on T2D risk are quite limited. In this study, no significant correlation was found between wheat intake and T2D risk in either gender. According to research on Geographic Variations in Dietary Patterns in China (11), wheat products are often consumed with other grains such as corn, rye, and millet, resulting in a mixed coarse and fine grain consumption pattern. On the other hand, white rice is generally accompanied by cooked vegetables and meat and rarely combined with other grains.
Our study contains numerous limitations worth noting. First, employing three consecutive 24-hour dietary recalls may lead to an underestimation of sporadic coarse grain intake. Second, identifying trajectories necessitates a minimum of three rounds of data. To fulfill the trajectory model fitting requirements, we imposed stringent inclusion criteria on our study design, potentially diminishing the representativeness of the samples analyzed and limiting the generalizability of our findings. Third, due to the inherent characteristics of observational studies, there is a potential for residual confounding, even after adjusting for various potential covariates.
This study was conducted to identify long-term trends in cereal consumption among Chinese adults and assess their corresponding risk of developing T2D. The objective was to provide fresh insights into T2D prevention by modifying risk factors. Findings suggest that the association between cereal intake patterns and diabetes onset has the potential to inform future dietary guidelines aimed at chronic disease prevention.
-
The authors declare no conflict of interest.
HTML
Conflicts of interest
| Citation: |

|