
 Download:
Download:




-
Transmission of coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), by aerosol has been confirmed in many studies (1-4), but transmission usually occurs in a confined space. In the epidemic that occurred in Guangzhou City of Guangdong Province in May 2021 (5), the index case and a close contact (later diagnosed as infected) arrived on international flights and were located in 2 different buildings in the hospital at the same time before diagnosis. The buildings were close to each other and formed a relatively enclosed space due to the exterior ceiling between the two buildings; buildings in this layout are sometimes informally referred to as handshake buildings due to their extremely close proximity—in this case, approximately 50 cm separated the handshake buildings.
Epidemiological investigation and viral gene sequencing showed that there was a temporal and spatial crossover between the two individuals and their genetic sequences were highly homologous, so aerosol transmission may be likely. We used fluorescence microspheres with similar aerodynamic characteristics to the SARS-COV-2 spike pseudovirus to investigate the transmission path and influencing factors of the virus aerosol through field experiment simulation. The results showed that there was clear aerosol transmission path from the location of the close contact and the index case, and its transmission was mainly affected by the airflow layout that resulted from switching the air conditioner on and off as well as opening and closing doors and windows. In the future, more attention should be paid to the risk of aerosol transmission in close-proximity buildings and to the influence of air distribution layout on aerosol diffusion in isolation wards.
We investigated the hospital and selected 6 sites for the field experiment (Figure 1). Site 1 and 2 were in the fever clinic building. Site 1 was the isolation ward where the infected person stayed; Site 2 was the corridor with windows that could open to an enclosed space, and each window faced the windows of a corresponding room in the clinic building; Sites 3–6 were in the routine clinic building opposite the fever clinic building. Site 3 was a traditional Chinese medicine clinic where the index case saw the doctor and its window was opened; Site 4 was a waiting area for patients with an opened window; Sites 5 and 6 were a doctor’s office and a consulting room, respectively, with closed windows. Considering the influence of the airflow layout, 6 simulation scenarios were set according to switching on and off the air conditioner (A) of Ward 1, (B) the opening and closing door of Ward 1, and (C) the window of Corridor 2 (Supplementary Table S1). Polystyrene fluorescent microspheres (supplied by the Beijing Institute of Metrology) with similar aerodynamic characteristics as SARS-CoV-2 spike pseudovirus were selected. The Collison Nebulizer (BGI, INC.) was used at Ward 1 to simulate the respiration of the infected person for 1–1.5 hours (exhalation of fluorescent microspheres was 1012–1013/hour), cough or sneeze (exhalation of fluorescent microspheres was 1011–1012 each cough or sneeze) (6-7). Meanwhile, the concentration of different particle sizes and some meteorological conditions were monitored at 6 sites every 10 minutes. PM10 samplers and bioaerosol samplers were used to collect aerosol samples, and samples of sedimentation were collected with cotton swabs. After the field experiment, the yellow and green fluorescent particles in different samples were observed by fluorescence microscope (Nikon DS-RI) in the laboratory, and the data directly read from the field were analyzed by OriginPro 8 SR3 (OriginLab Company, Northampton, United States).
 Figure 1.
Figure 1.Exterior and interior layout of the fever clinic building and the routine clinic building. (A) Exterior layout of the buildings. (B) Interior room layout of the buildings.
Note: In the exterior layout of the buildings, the two-storied building was the fever clinic building, and the five-storied building was the routine clinic building. The distance between the external walls of the 2 buildings is 51 cm. The corridor window had a distance of 77 cm from the window of the opposing traditional Chinese medicine clinic. The isolation area on the second floor and the traditional Chinese medicine clinic on the opposite side formed a relatively enclosed space through the exterior ceiling between the two buildings. In the interior room layout of the buildings, Sites 1–6 were where field experiments were conducted. Triangles (a–c) were influencing factors on airflow distribution: (a) an air conditioner; (b) a door; (c) a window. Red dot was where the Collison Nebulizer was located. Fan symble () showed the air conditioner was switched on. Green particles were fluorescent microspheres to simulate exhaled virus aerosol of the imported infected person and transmission diffusion path. Scenario Site 1 Site 2 Air conditioner Door Window 1 × × × 2 √ × × 3 √ √ × 4 √ × √ 5 × √ √ 6 √ √ √ Note: √: open or switch on; ×: close or switch off. Table S1. The six ventilation layout scenarios according to the air conditioner, door, and window status.
A total of 7,411 data from the field and 304 samples were obtained in the simulation experiment, including 210 cotton swab samples for wiping the object surface, 54 aerosol liquid samples, 40 aerosol filter membrane samples. In Ward 1, aerosolized fluorescent microspheres were used to simulate the respiration of the infected person and observe the diffusion in Corridor 2 and the opposite of Room 3 through the variation in concentration of aerosol particles, the results were shown in Figure 2. In Ward 1, the concentration of particles in 0.3 µm increased significantly and remained stable after rising to the highest level as well as particles in 0.5, 1, 2.5, 5, and 10 µm. After aerosolization of fluorescent microspheres, the concentration of particles in the Corridor began to rise immediately and remained unchanged after reaching its highest value. Compared with the change at Ward 1, the peak time of particle concentration was relatively delayed. For the opposite of Room 3, particle concentration began to rise 20–40 minutes after aerosolization of fluorescent microspheres. During the monitoring time, only the peak concentration was detected, but no plateau of high concentration was detected. In some scenarios, particle concentration did not change significantly in Room 3. At the same time, fluorescent microspheres were detected in aerosol filter membrane samples, aerosol liquid samples, and swab samples that were collected at the above 3 sites (Figure 3). The results showed that the complete aerosol transmission chain could be obtained from Ward 1 to the Corridor to the opposite of Room 3.
 Figure 2.
Figure 2.The changes of particle concentration over time at 0.3 μm in 6 different scenarios at different sites (Site 1, Site 2, and Site 3).
Note: The abscissa axis represents time (minutes); the ordinate axis represents the particle concentration (particle/L); the number behind the dash represents different simulation scenarios, i.e., Site 1-1 refers to the changes of particle concentration in 0.3 μm with time at Site 1 in Scenario 1.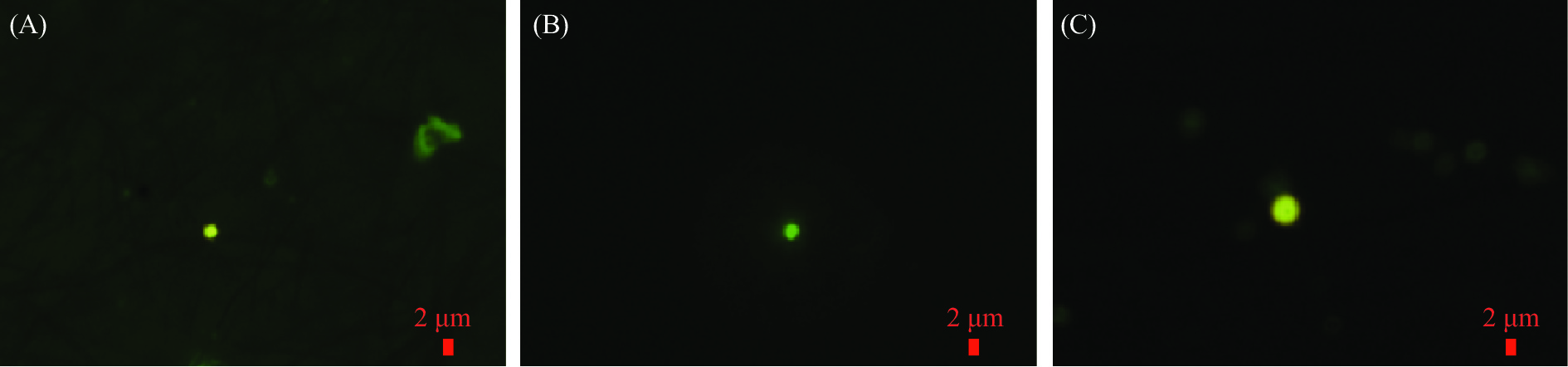 Figure 3.
Figure 3.Representative photos of fluorescent microspheres tracked by different sampling methods in different sites. After the aerosolization of fluorescent microspheres at Site 1, fluorescent microspheres (yellow and green) were detected in (A) the aerosol filter membrane sample using PM10 samplers (100 L/min) under fluorescence microscopy; (B) the aerosol liquid sample using biological aerosol samplers (100 L/min) under fluorescence microscopy; and (C) an air sample using natural sedimentation on table, door handle, windowsill, chair, etc., under fluorescence microscopy.
The effects of (A) air conditioners, (B) doors, and (C) windows on aerosol transmission was investigated through 6 different scenarios. The results showed that under the conditions that air conditioners, doors, and windows were all switched off or closed, no fluorescent microspheres were found in the air filter membrane samples and liquid samples collected in Room 3 after aerosolization of fluorescent microspheres in Ward 1. This showed that when airflow was poor, fluorescent microspheres were not easily to spread to Room 3. When air conditioners, doors, and windows were all switched on or opened, fluorescent microspheres quickly spread to Room 3. As long as air conditioners were switched on, the air current circulated in the ward and the particle concentration in the Corridor and Room 3 rose slowly even if doors and windows were closed. Once a door was opened, particles in the Corridor could rise to the highest concentration in 5 minutes, but the change of particle concentration in Room 3 was less affected. Once a window was opened, particle concentration in Room 3 changed rapidly and significantly even if the door was closed.
In addition, the influence of doors, windows, and personnel movement on aerosol transmission to Office 5 and Room 6 which were adjacent to Room 3 was investigated under the condition that air conditioner was switched on. During the experiment, people left Room 3 and entered the Waiting Area and Room 6 every 10 minutes. The results showed that no fluorescent microspheres were detected in aerosol filter membrane samples and liquid samples collected in the Waiting Area, Office 5, and Room 6 when window was closed. Once a window was opened, fluorescent microspheres were detected in the samples in the Waiting Area and Room 6, but no fluorescent microspheres were detected in Office 5 because no personnel enter and exit from Office 5. It can be found that the risk of aerosol transmission was low when the opposing window of the handshake building was closed.
HTML
-
Aerosol field simulation experiments can observe the concentration change of aerosol particle in air in real time to determine the transmission path of aerosol. Through the settings of different scenes, the influencing factors of transmission can be determined. In addition, when people walked around, they will influence the airflow and spread fluorescent microspheres to other places. It has also been confirmed that human activities can affect bacteria-carrying particles in a study (8). After simulating breathing and coughing or sneezing of infected persons, fluorescent microspheres can persist in the air and the particle sizes were mainly between 0.3 μm and 0.5 μm. Under a certain air distribution layout, they can spread to handshake buildings in 20–40 minutes. The better the ventilation, the faster the transmission. Some fluorescent microspheres can settle to the surface of tables, windowsills, and other objects after coagulation. Presently, the research on SARS-CoV-2 transmission usually focused on the simulation cabin experiment or computational fluid dynamic model (9-10). This result provided a basis for epidemic prevention and control and experimental support for future research.
Although some results were obtained, this study was subject to some limitations. First, real SARS-CoV-2 could not be used in real environments due to hazardous risk, so the virus aerosol could not be properly quantified. Second, there was no way to recover the meteorological conditions when the index case stayed in the hospital, so the analysis may be subject to some biases.
The above aerosol simulation experiments for tracing the index case not only supported aerosol transmission but also found key factors affecting transmission. Therefore, adequate space should be maintained between isolation wards and routine outpatient areas in hospitals, and air distribution layouts should be examined in isolation wards. Furthermore, disinfections in the isolation area need be strengthened. COVID-19 aerosol transmission risk exists in many handshake buildings in Guangzhou due to centralized isolation and home isolation and is highly concerning.
-
No conflicts of interest.
-
Guangdong Provincial Center for Disease Control and Prevention; and Cubic Sensor and Instrument Co., Ltd.
| Citation: |

|