
 Download:
Download:




HTML
-
Introduction:Brucellosis is an important zoonotic infectious disease with its main mode of transmission from livestock to humans. The study analyzed epidemiological characteristics of human brucellosis from 2016 to 2019 in China, aiming to understand progress of the National Program of Brucellosis Prevention and Control.
Methods:The research obtained data on human brucellosis cases reported through China’s National Notifiable Disease Reporting System (NNDRS) from January 1, 2016 to December 31, 2019 and described brucellosis epidemiological patterns by region, seasonality, age, sex, and occupation.
Results:The number of cases reported nationwide in China decreased from 47,139 (3.4/100,000) in 2016 to 37,947 (2.7/100,000) in 2018, and then increased to 44,036 (3.2/100,000) in 2019, with an average annual incidence of 3.0/100,000 during the four study years. Brucellosis in Xinjiang declined from 35.6/100,000 in 2016 to 16.3/100,000 in 2019 — an average annual decrease of 22.9%. Brucellosis in Inner Mongolia increased from 23.8/100,000 in 2016 to 54.4/100,000 in 2019 — an average increase of 31.8% per year and accounting for 22% of all reported cases. Northern China reported 95.2% of cases during this period and still had an incidence of 7.2/100,000 and 87.0% of counties being affected by brucellosis in 2019. In this region in 2019, males aged 45-64 years old had an incidence of over 15.9/100,000, compared with over 7.0/100,000 among females aged 45-64 years old.
Conclusions:Although there was progress in prevention and control of human brucellosis in some provincial-level administrative divisions (PLADs) in 2016 through 2019, progress was limited nationwide and there was an overall resurgence of brucellosis in 2019. The resurgence was primarily in Inner Mongolia. An One Health approach should be strengthened to ensure successful and sustainable brucellosis prevention and control in China.
-
Brucellosis is a zoonotic disease caused by various Brucella species (1). Humans are infected most often though contact with sick animals, especially goats, sheep, and cattle, and through consumption of contaminated milk and milk products such as fresh cheese (1–2). In China, the main mode of transmission is contact with sick livestock such as sheep, goats, and cattle (3). Clinical features during the acute phase of human brucellosis are fever, hyperhidrosis, fatigue, and joint and muscle pain. If timely and effective treatment is not available during the acute phase, the infection can become chronic, which causes great suffering (4-5).
More than 170 countries and regions in the world have reported human and animal brucellosis (6). In the 1950s, brucellosis was widespread in China, with infection rates of human and animal brucellosis as high as 50% in severely affected areas. Following strengthened prevention and control measures based on the One Health approach, the brucellosis epidemic declined (7). However, at the beginning of the 21st century, human brucellosis had a resurgence in China, with sharply increasing incidences and widely expanded affected areas in the north and the south (8-9). In 2014 and 2015, the number of reported cases exceeded 50,000 per year, and the annual incidence rates were 4.22/100,000 and 4.18/100,000, which were historically high levels (8,10). To prevent and control human brucellosis, China’s Ministry of Agriculture and the National Commission of Health and Family Planning in 2016 co-issued a National Brucellosis Prevention and Control Plan (2016–2020) (11). The study analyzed the epidemiological characteristics of human brucellosis from 2016 to 2019 in China to evaluate progress of the national plan.
-
The study obtained data on human brucellosis cases reported through China’s National Notifiable Disease Reporting System (NNDRS) from January 1, 2016 to December 31, 2019. NNDRS is an Internet-based national passive surveillance system that covers all township health centers and all levels of hospitals across the country. The research compared numbers of annual cases and incidences by region, age, gender, and occupation. This study evaluated the time trend of human brucellosis of all the provincial-level administrative divisions (PLADs) with average annual growth of annual incidence. The average annual growth rate of annual incidence from 2016 to 2019 was defined as:
$ \sqrt[3]{\dfrac{annual \;incidence\; in\; 2019}{annual\; incidence \;in\; 2016}}-1) \times 100\% $ . The research compared the number and percent of affected counties, number of reported cases, incidence, and median number of cases at the county level between southern and northern China. Southern PLADs including Jiangsu, Shanghai, Zhejiang, Anhui, Hunan, Hubei, Sichuan, Chongqing, Guizhou, Yunnan, Guangxi, Guangdong, Hainan, Fujian, and Jiangxi; northern PLADs included Heilongjiang, Jilin, Liaoning, Beijing, Tianjin, Inner Mongolia, Shaanxi, Hebei, Henan, Ningxia, Shanxi, Shandong, Gansu, Qinghai, Xinjiang, and Tibet. All statistical analyses were performed using SAS (version 9.4, SAS Institute Inc., Cary, USA) and the figures was drawn using Microsoft Excel (version 2007). -
From 2016 to 2019, a total of 167,676 cases of human brucellosis was reported to NNDRS in the mainland of China, for an average annual incidence of 3.02/100,000 population. The annual number of cases reported nationwide was 47,139 (3.43/100,000) in 2016 and decreased to 38,554 (2.79/100,000) in 2017 and 37,947 (2.73/100,000) in 2018. Reported cases increased to 44,036 (3.15/100,000) in 2019. The peak season for human infections (by date of illness onset) was from March to August, accounting for 64.5% of cases in 2016–2019. The north and south had similar seasonal distributions (Figure 1).
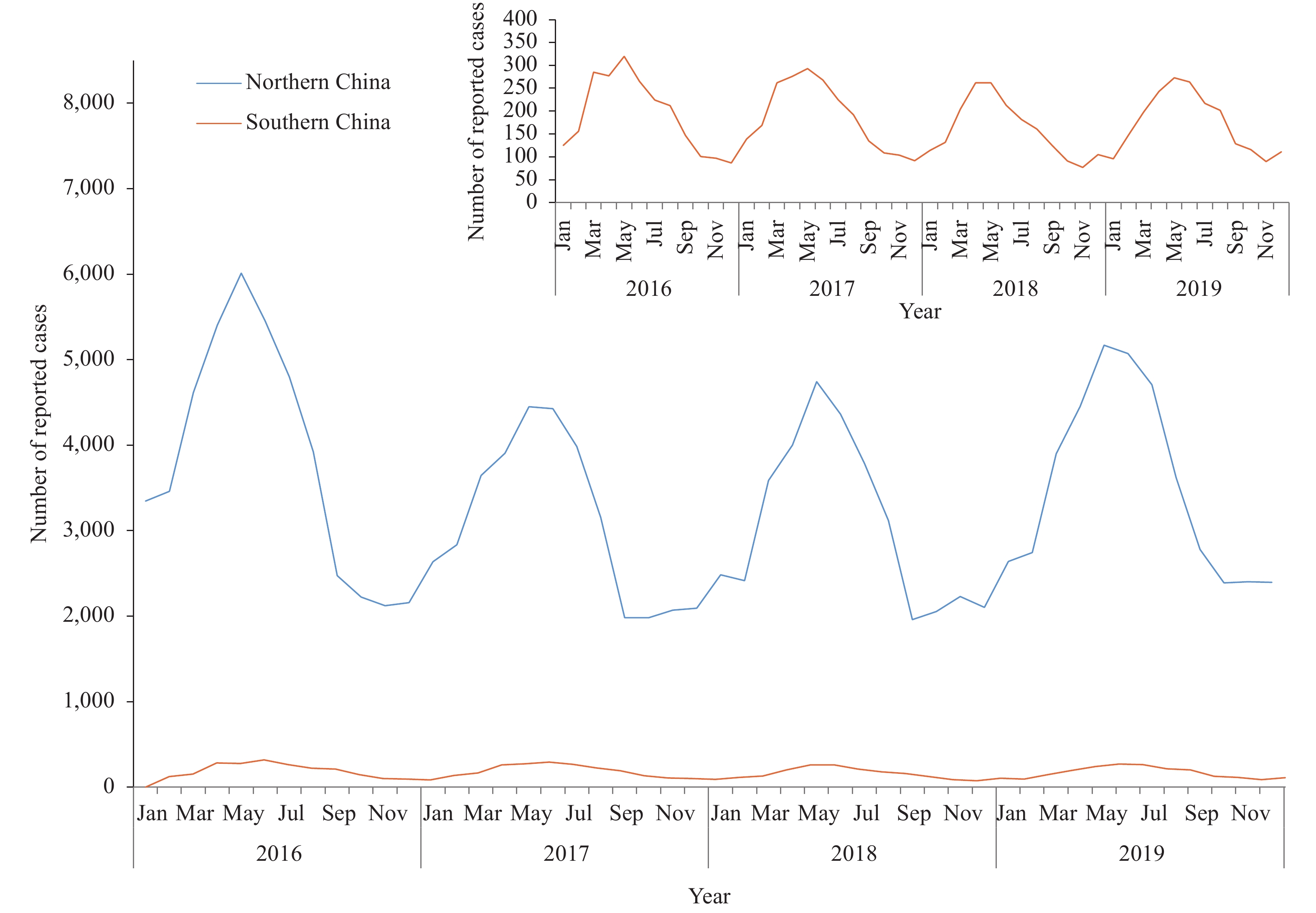 Figure 1.
Figure 1.Monthly distribution of human brucellosis in northern and southern China, 2016–2019.
Human brucellosis was reported in all 31 PLADs of the mainland of China; 95.2% (159,667) were reported from northern PLADs. Inner Mongolia reported the most cases (36,805 cases; 22.0% of all reports) and had an average annual incidence of 36.5/100,000. The other 10 PLADs with the highest number of cases were located in northern PLADs — Ningxia, Heilongjiang, Shanxi, Gansu, Liaoning, Jilin, Hebei, Henan, and Shandong (Figure 2), with average annual incidences ranging from 3.1/100,000 to 28.2/100,000. The incidence of human brucellosis was less than 1.0/100,000 in all southern PLADs; in Shanghai, the incidence was less than 0.1/100,000.
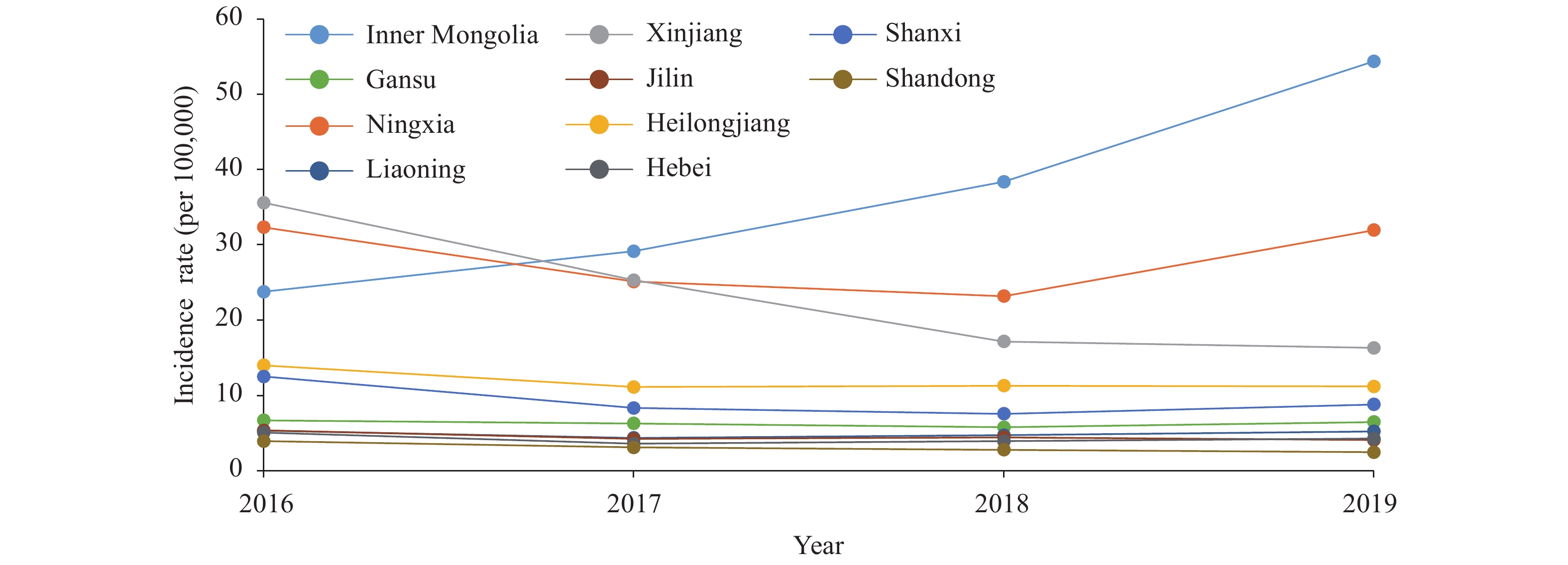 Figure 2.
Figure 2.Human brucellosis in the ten provincial-level administrative divisions (PLADs) with the highest incidence rate of cases reported from 2016 to 2019.
High-burden PLADs differed in annual incidence patterns (Figure 2). Inner Mongolia had an upward trend with an annual incidence increasing from 23.8/100,000 in 2016 to 54.4/100,000 in 2019 — an average annual increase of 31.8%. Ningxia, Shanxi, Gansu, Shaanxi, Liaoning, and Hebei’s annual incidences declined and then increased. In Ningxia, brucellosis increased more than 8/100,000 from 2018 to 2019. In Heilongjiang, Jilin, and Henan, incidences declined in 2017 and remained relatively stable in 2018 and 2019. Xinjiang’s annual incidence decreased from 35.6/100,000 in 2016 to 16.3/100,000 in 2019 — an average annual decrease of 22.9% (Figure 2, Supplementary Table S1). Several provinces in southern China had significant annual increases in incidence, including Hainan (39.7%), Fujian (23.8%), Anhui (19.2%), and Hunan (7.5%) (Supplementary Table S1).
The percent of counties affected by brucellosis increased from 63.7% in 2016 to 65.9% in 2017 and decreased to 64.3% in 2019. Most affected counties were in northern PLADs. The percent of affected counties in southern PLADs increased from 40.4% in 2016 to 41.2% in 2019. The annual incidence of human brucellosis varied by county, with median incidences (interquartile range [IQR]) of 2.0 (0.5, 7.3)/100,000 in 2016 and 1.7 (0.5, 5.7)/100,000 in 2019. Counties in northern PLADs had higher median incidences than counties in southern PLADs: 4.4 (IQR: 1.6, 13.1)/100,000 vs. 0.4 (0.2, 0.7)/100,000 in 2016, and 3.4 (1.4, 10.9)/100,000 vs. 0.3 (0.2, 0.6)/100,000 in 2019. The 10 counties with the highest average annual incidence had incidences ranging from 124.5/100,000 to 265.0/100,000; among these, 6 were in Inner Mongolia, 3 in Xinjiang, and 1 in Ningxia. In 2019, the median of cases reported by county was 7 and was higher in northern China than in southern China (13 vs. 2) (Table 1, Supplementary Table S2).
Year Region Affected counties Incidence* (per 100,000) Number Percentage (%) 2016 South 591 40.4 (591/1,463) 0.3 North 1,286 86.8 (1,286/1,482) 7.8 Total 1,877 63.7 (1,877/2,945) 3.4 2017 South 657 44.9 (657/1,462) 0.3 North 1,286 86.6 (1,286/1,485) 6.3 Total 1,943 65.9 (1,943/2,947) 2.8 2018 South 597 40.9 (597/1,461) 0.2 North 1,298 87.3 (1,298/1,487) 6.2 Total 1,895 64.3 (1,895/2,948) 2.7 2019 South 603 41.2 (603/1,462) 0.2 North 1,294 87.0 (1,294/1,488) 7.2 Total 1,897 64.3 (1,897/2,950) 3.2 * Incidence was calculated as the total number of cases in each region divided by the total population in the same region. Table 1. Comparison of human brucellosis between northern and southern China PLADs by numbers of affected counties and incidence (1/100,000), 2016–2019.
Farming and herding were the most common occupations of reported cases, accounting for 83.8% of reports. Houseworkers and unemployed individuals, students, and migrating individuals and kindergarten children accounted for 4.5%, 1.9%, and 1.1% of cases, respectively. The incidence among males was higher than that among females in all age groups and in the south and north, except for those aged 0–4 years and 5–9 (Figure 3 and Supplementary Table S3). People aged 45-64 years old had higher risk of infection than younger people. Those aged 45-64 years old had an incidence over 15.9/100,000 in the north in 2019, compared with over 7.0/100,000 among females (Figure 3 and Supplementary Table S3).
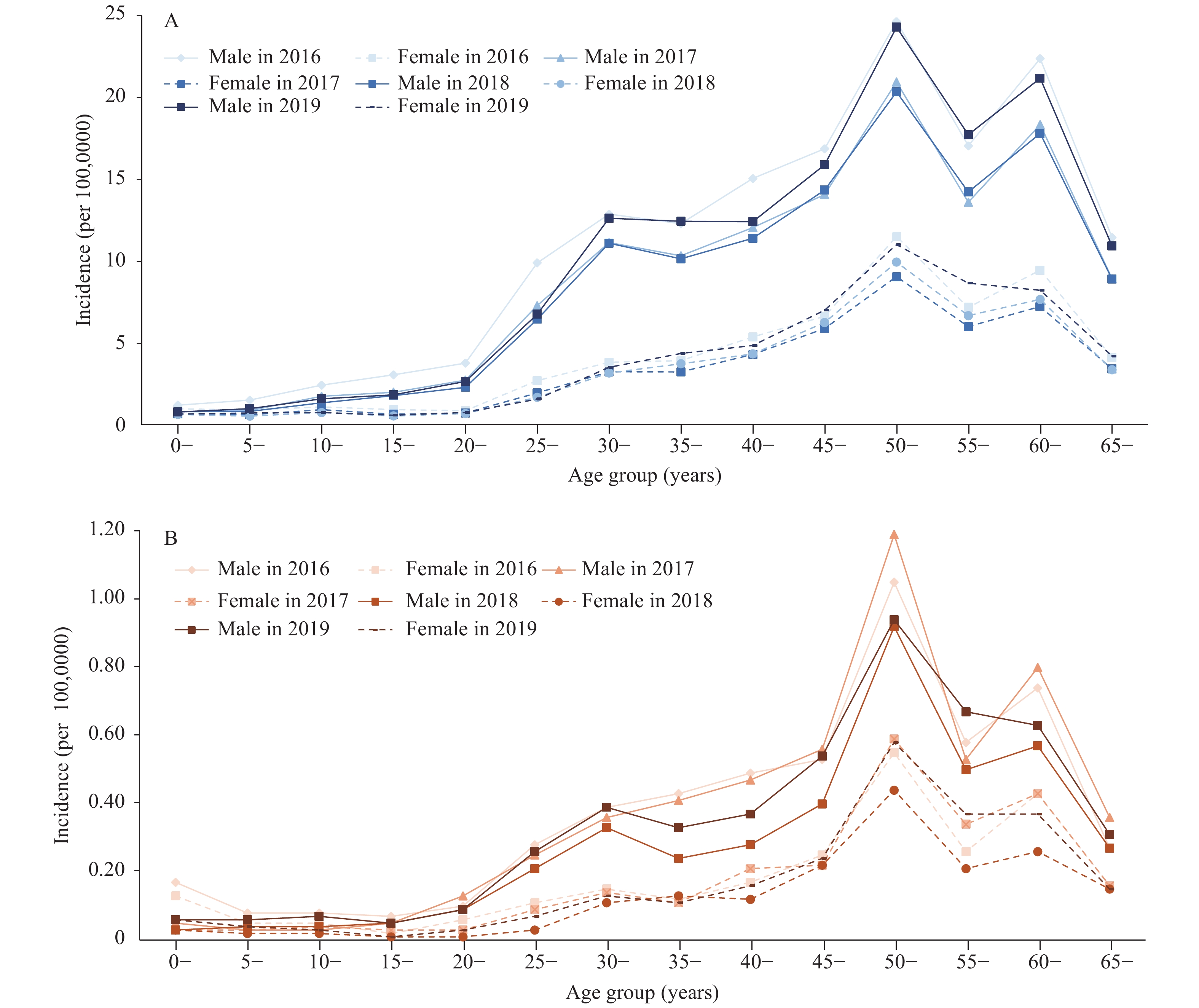 Figure 3.
Figure 3.Age and sex distribution of annual incidence (1/100,000) of human brucellosis by north and south from 2016 to 2019 in China. (A) Age and sex distribution of human brucellosis in northern China, 2016−2019. (B) Age and sex distribution of human brucellosis in southern China, 2016−2019.
-
Our study found that human brucellosis had a resurgence in 2019 in China, although the overall epidemic level was nearly 30% lower in 2019 than in the peak year of 2014. Inner Mongolia had a rapid increase that started in 2017, and its surrounding provinces experienced a subsequent resurgence. Northern China reported the vast majority of cases and had a much higher incidence than did southern China. Older male farmers and herders were the highest risk populations.
According to the National Brucellosis Prevention and Control Plan (2016–2020), the targets of brucellosis control by the end of 2020 include: 1) counties in 11 PLADs including Hebei, Shanxi, Inner Mongolia, Liaoning, Jilin, Heilongjiang, Shaanxi, Gansu, Qinghai, Ningxia, Xinjiang, should have reached and maintained control standards (an indicator is that new human cases decrease compare with the previous year); 2) counties in Hainan Province should have reached the elimination standard (an indicator is that there should be no new confirmed human cases for 3 consecutive years); and 3) counties in the other PLADs should have reached near-elimination standard (an indicator is that there were no new confirmed human cases for 2 consecutive years). Our study showed that in 2019, all PLADs in the mainland of China, including Hainan, still had reported human brucellosis cases, and that nearly 90% of northern counties and more than 40% of southern counties were affected. We found that the national program had limited progress and did not achieve these objectives by the end of 2019.
Animal brucellosis control is the most effective strategy for human brucellosis control (1). In addition to health education, early detection, and proper treatment for high-risk populations, the national program required highly endemic areas to implement a mass animal vaccination strategy and used a “quarantine-vaccination-slaughter” policy in the less-affected areas (i.e. to vaccinate the negatives and safely slaughter the animals testing positive based on quarantine results). Some areas succeeded, with Xinjiang as a good example. As one of the endemic regions in China, Xinjiang implemented a mass animal vaccination campaign against brucellosis starting in 2016 (12) and has seen a dramatical decrease in the incidence of human brucellosis. A study in Hami Prefecture of Xinjiang showed that the brucellosis infection rate among local cattle and sheep dropped significantly from 2017 to 2019 (13).
There are several possible reasons for the increasing incidence in Inner Mongolia and the subsequent rebound in the surrounding provinces. First, the market price of beef and lamb has been rising since 2016 and the number of people engaged in breeding, purchasing, selling, and trading has increased. Second, the movement of livestock increased with the growing demand and has led to spread of brucellosis via sick animals due to the lack of proper quarantine and inspection. For example, a genotype study showed that Brucella strains in Inner Mongolia were related to those in neighboring provinces (14). Third, the investment of resources for controlling brucellosis might have been reduced, and activities based on One Health principles decreased after consecutive declines in previous years — a possible reason based on impressions during field visits to endemic areas.
Northern China had a more severe epidemic, which is consistent with previous studies (8–9). This may be because husbandry of goats, sheep, and cattle is more common in rural areas in northern China. The main pastoral areas and the historically epidemic zone of brucellosis are both located in northern China. Although the southern PLADs had a small proportion of cases, the affected areas in the south expanded and some had rapid increases in incidence. This expansion may be related to trading and movement of livestock from north to south, which is a phenomenon deserving more attention.
The incidence of brucellosis has clear seasonal characteristics with peaks in the late spring and summer, which was consistent with previous studies (8–9). Farmers and herders remain high-risk occupations. Continuous effort is needed to promote proper use of personal protection equipment to prevent infection. The incidence among males was higher than among females, which was also found in previous research (8-10,15), but the incidence of males under 10 years of age was similar to the incidence of same-age females. This may represent lower exposure risk of brucellosis in children under 10 years old, while older-age men are more likely to have occupational exposures through breeding livestock.
Our study has limitations. The data were obtained from NNDRS and may be impacted by the case finding ability of different areas. Our incidence estimates may underestimate the true incidence of brucellosis, as it is a globally underreported disease due to its typical symptoms and signs at the early stage. However, surveillance data can still reflect trends of the epidemic, something that is supported by the stability and even quality of NNDRS in China. NNDRS has the highest quality and most complete data that are currently available for evaluation of the epidemiological characteristics and progress towards national program goals.
In conclusion, from 2016 to 2019, although human brucellosis prevention and control showed progress in some PLADs, progress was limited nationwide and brucellosis had a resurgence in 2019. The resurgence was most prominent in Inner Mongolia. An One Health approach should be strengthened to ensure successful and sustainable brucellosis prevention and control in China. Health education campaigns should be focus on middle- and older-age groups of farmers and herders in northern China.
Acknowledgements:Dr. Lance Rodewald, senior advisor of China CDC; health staff of CDCs at the provincial, prefecture, and county levels in all PLADs in the mainland of China.
Conflicts of interest: No reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Funding:This work was supported by National Science and Technology Major Project of China (2018ZX10101002-003-002).

| Citation: |

|