
 Download:
Download:




-
Introduction: Preterm birth (PTB) is a major public health concern. Noise exposure and gestational hypertension (GH) are recognized risk factors for PTB; however, few studies have examined their independent and combined effects on PTB among female workers.
Methods: A cross-sectional survey was conducted among female manufacturing and mining workers in Gansu, Chongqing, Hebei, and Beijing. Propensity score matching (PSM) at a 1∶1 ratio balanced baseline characteristics between noise-exposed and non-exposed groups, yielding 7,886 matched participants (3,943 per group). Univariate logistic regression estimated the independent associations of noise exposure and GH with PTB, while multivariate logistic regression assessed their additive interaction, quantified by relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (S).
Results: After PSM, the overall PTB prevalence was 9.3%, with higher rates in manufacturing (10.9%) than in mining (7.7%). Occupational noise [odds ratio (OR)=2.26, 95% confidence interval (CI): 1.93, 2.66] and GH (OR=1.83, 95% CI: 1.24, 2.68) independently elevated PTB risk. A significant positive additive interaction was detected, with the highest risk in the co-exposed group (aOR=4.06, 95% CI: 2.14, 7.70; RERI=1.11, AP=27.34%, S=1.57).
Conclusion: Occupational noise exposure and GH are independent risk factors for PTB among female workers, with a synergistic additive effect when co-present. Integrated interventions targeting both exposures may help reduce the PTB burden in this population.
-
Preterm birth (PTB), defined as delivery before 37 weeks of gestation, represents a major global public health challenge, contributing substantially to neonatal morbidity, mortality, and long-term developmental impairment (1). Global estimates indicate that 13.4 million preterm births occurred in 2020 (9.9% of live births), with notable regional disparities (2), while in China, PTB rates rose from 5.13% in 2017 to 6.56% in 2022 (3). The burden may be disproportionately heavy among female workers — who account for 45% of China's workforce — owing to cumulative reproductive risks from occupational stressors. PTB is multifactorial, with modifiable risk factors including occupational environmental exposures and pregnancy-related complications (4). Excessive occupational noise, prevalent in industrial settings (31.2% of Chinese manufacturing workers were exposed to >85 dB(A) in 2020) (5), and gestational hypertension (GH, affecting 5.6%–9.4% of pregnancies in China) (6) have each been independently linked to PTB through mechanisms such as hypothalamic-pituitary-adrenal (HPA) axis activation, placental dysfunction, and endothelial injury (7–8).
To date, most studies have focused on the independent effects of noise or GH, overlooking potential interactive effects that may amplify PTB risk. In addition, confounding factors (e.g., age, lifestyle) are often inadequately controlled in observational studies, leading to biased effect estimates. Moreover, large-scale evidence specifically targeting female workers — a high-risk occupational population — remains scarce, hindering the development of context-specific occupational health policies. To address these gaps, this cross-sectional survey aimed to investigate the independent associations of occupational noise exposure and GH with PTB among female workers and to evaluate their additive interaction on PTB risk.
A cross-sectional survey was conducted from 2024 to 2025 across four provincial-level administrative divisions (PLADs) — Gansu, Chongqing, Hebei, and Beijing — targeting female workers aged 20–50 years with ≥1 year of work experience and a pregnancy history in the mining and manufacturing industries (selected for their high proportion of female employees). Exclusion criteria included confirmed organic diseases affecting reproductive health, a personal or family history of reproductive system tumors, other malignant tumors, and severe mental or cognitive impairment precluding independent questionnaire completion. Of 9,345 initially recruited workers, 20 with incomplete basic information were excluded, leaving 9,325 participants for analysis. Propensity score matching (PSM) was performed using a 1∶1 nearest-neighbor algorithm with a caliper width of 0.2 standard deviations of the propensity score — a widely recommended threshold to balance baseline comparability and reduce matching bias. The matching model included the following covariates: age, marital status, smoking, alcohol consumption, and industry type, selected based on published evidence and data accessibility. Characteristics of unmatched participants were summarized (
Supplementary Table S1 ), and covariate balance was rigorously evaluated before and after matching using standardized mean differences (SMD). Robust standard errors were employed in subsequent regression models to improve estimation accuracy. Sensitivity analyses using alternative caliper values (0.1 and 0.3) were conducted to verify the robustness of the main findings. After PSM, the final matched sample comprised 7,886 participants (3,943 in the noise-exposed group and 3,943 in the non-exposed group) (Supplementary Figure S1 ).A standardized questionnaire developed by the research team was used for data collection (9), capturing the following variables: demographic and lifestyle characteristics (industry type, gestational age, marital status, smoking, and alcohol consumption) (10); occupational noise exposure, based on self-report during pregnancy and verified against enterprise occupational hazard detection reports [8-hour equivalent continuous A-weighted sound pressure level (LEX,8h)] to reduce recall bias (11); gestational hypertension (GH), defined per international guidelines as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg after 20 weeks of gestation with no pre-pregnancy history of hypertension, validated through self-reported medical records and prenatal examination data; and PTB, defined as delivery at <37 completed weeks of gestation, determined by self-reported gestational age at delivery (1).
All statistical analyses were performed using R (version 4.5.1, R Foundation for Statistical Computing, Vienna, Austria). Standardized mean differences (SMD) assessed covariate balance after PSM, with SMD<0.1 indicating adequate balance. Univariate logistic regression estimated odds ratios (OR) and 95% confidence intervals (CI) for the independent associations of noise exposure and GH with PTB. Multivariate logistic regression evaluated the additive interaction between noise exposure and GH on PTB risk, quantified by relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (S). The 95% CIs for additive interaction indices were calculated using the delta method. Pairwise association analyses informed the study's conceptual framework. Statistical significance was set at a two-sided α=0.05.
Table 1 presents the baseline characteristics of the 7,886 matched participants (3,943 per group). After PSM, SMD values for all covariates — age, marital status, smoking, alcohol consumption, and industry type — were below 0.1, confirming adequate balance between groups. The overall GH prevalence was 2.6%, and PTB prevalence was 9.3%. Among all participants, 21.3% had noise exposure levels (LEX,8h) exceeding 85 dB(A), with a higher proportion observed in the noise-exposed group than in the non-exposed group.
Variables Total (n=7,886)
n (%)Noise group (n=3,943) n (%) Non-noise group (n=3,943) n (%) SMD LEX,8h ≥85 [dB(A), %] Prevalence of GH (%) Prevalence of PTB (%) Age (years) 0.002* <25 1,658 (21.0) 828 (21.0) 830 (21.0) 21.8 1.3 9.3 25–29 3,388 (43.0) 1,695 (43.0) 1,693 (42.9) 20.0 2.0 9.0 ≥30 2,840 (36.0) 1,420 (36.0) 1,420 (36.0) 22.4 4.2 9.6 Marital status 0.006* Unmarried 38 (0.5) 19 (0.5) 19 (0.5) 10.5 5.3 15.8 Married 7,635 (96.8) 3,816 (96.8) 3,819 (96.9) 21.4 2.6 9.2 Divorced/widowed 213 (2.7) 108 (2.7) 105 (2.7) 17.8 1.4 12.2 Smoking status 0.012* Yes 59 (0.7) 28 (0.7) 31 (0.8) 18.6 5.1 8.5 No 7,827 (99.3) 3,915 (99.3) 3,912 (99.2) 21.3 2.6 9.3 Alcohol consumption 0.007* Yes 171 (2.2) 87 (2.2) 84 (2.1) 24.0 4.1 14.6 No 7,715 (97.8) 3,856 (97.8) 3,859 (97.9) 21.2 2.6 9.2 Industry 0.016* Manufacturing 3,961 (50.2) 1,965 (49.8) 1,996 (50.6) 25.2 2.4 10.9 Mining 3,925 (49.8) 1,978 (50.2) 1,947 (49.4) 17.3 2.8 7.7 Total 7,886 (100.0) 3,943 (100.0) 3,943 (100.0) 21.3 2.6 9.3 Abbreviation: SMD=standardized mean difference; LEX,8h=8-hour equivalent continuous A-weighted sound pressure level; GH=gestational hypertension; PTB=preterm birth; dB(A)=A-weighted decibel.
* SMD<0.1, indicating good balance of confounding factors between the two groups.Table 1. Epidemiological characteristics of participants in noise and non-noise groups after propensity score matching (n=7,886).
Univariate logistic regression (Figure 1) examined the pairwise associations among noise exposure, GH, and PTB to establish the basis for subsequent interaction analyses. In Model 1, noise exposure was significantly associated with increased PTB risk (OR=2.26, 95% CI: 1.93, 2.66; P<0.01). In Model 2, no significant association was observed between noise exposure and GH (OR=1.23, 95% CI: 0.89, 1.69; P>0.05). In Model 3, GH was significantly associated with elevated PTB risk (OR=1.83, 95% CI: 1.24, 2.68; P<0.01). These results, summarized as a conceptual framework (Figure 1), indicate that both noise exposure and GH may independently contribute to PTB risk, whereas noise exposure itself was not associated with GH development.
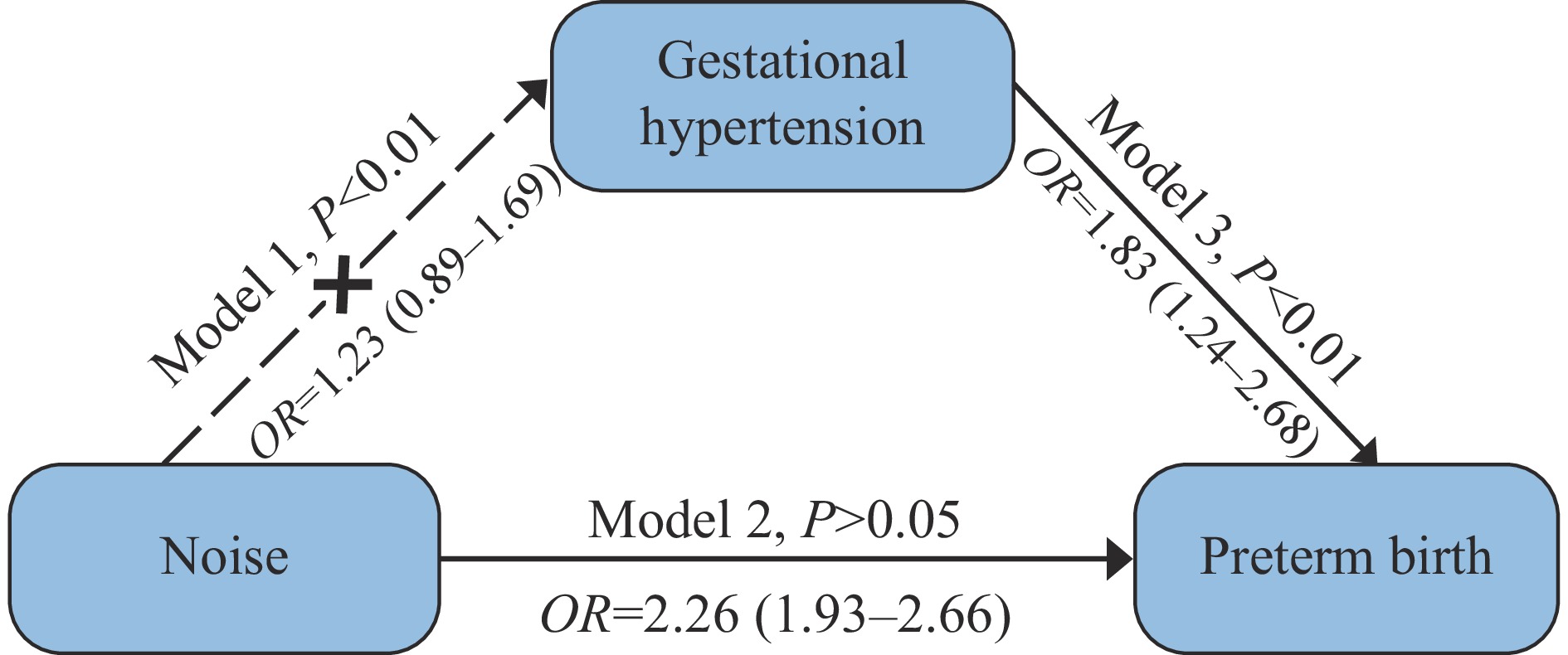 Figure 1.
Figure 1.A conceptual framework illustrating relationships among noise exposure, GH, and PTB using univariate logistic regression.
Abbreviation: GH=gestational hypertension; PTB=preterm birth; OR=odds ratio; CI=confidence interval.Table 2 presents the results of multivariate logistic regression, adjusted for maternal age, marital status, smoking, alcohol consumption, and industry type, with the “no noise exposure + no GH” group as the reference (OR=1.00). PTB risk was significantly elevated in both the GH-only group [adjusted odds ratio (aOR)=1.77, 95% CI: 1.09, 2.91; P=0.02] and the noise-only group (aOR=2.18, 95% CI: 1.85, 2.56; P<0.01), with the highest risk observed in the co-exposed group (aOR=4.06, 95% CI: 2.14, 7.70; P<0.01).
Group N (PTB cases) aOR (95% CI) P RERI (95% CI) AP (95% CI) S (95% CI) No noise + No gestational hypertension 6,055 (453) 1.00 Gestational hypertension 155 (19) 1.77 (1.09, 2.91) 0.02 Noise 1,625 (250) 2.18 (1.85, 2.56) <0.01 Noise + Gestational hypertension 51 (13) 4.06 (2.14, 7.70) <0.01 1.11 (0.02, 2.20) 27.34% (1.20%, 53.48%) 1.57 (1.03, 2.11) Note: Multivariate logistic regression adjusted for maternal age, marital status, smoking status, alcohol consumption, and industry type as independent variables.
Abbreviation: aOR=adjusted odds ratio; CI=confidence interval; RERI=relative excess risk due to interaction; AP=attributable proportion; S=synergy index; GH=gestational hypertension; PTB=preterm birth.Table 2. Interaction of noise exposure and GH on PTB using multivariate logistic regression.
Additive interaction analysis revealed a significant positive interaction between noise exposure and GH on PTB risk, with a RERI of 1.11 (95% CI: 0.02, 2.20), an AP of 27.34% (95% CI: 1.20%, 53.48%), and an S of 1.57 (95% CI: 1.03, 2.11), indicating that the combined effect of both exposures exceeded the sum of their individual effects (Table 2).
-
In this study, the independent association between occupational noise exposure and PTB (OR=2.26, 95% CI: 1.93, 2.66) was consistent with prior epidemiological evidence. Wing et al. demonstrated that combined stressors of noise and air pollution elevated PTB risk (OR=1.15, 95% CI: 1.03, 1.28) in Los Angeles (12). Our large sample size strengthens the reliability of these findings within the study population, providing a preliminary reference for occupational health protection among female workers in manufacturing and mining in similar settings (13). The underlying mechanisms may involve chronic noise-induced psychological stress that disrupts the hypothalamic-pituitary-adrenal axis, elevates cortisol levels, impairs placental blood flow, and triggers oxidative stress and inflammation (14–15).
Gestational hypertension was independently associated with a 1.83-fold increased risk of PTB (95% CI: 1.24, 2.68), consistent with global epidemiological data and recent studies. A systematic review and meta-analysis by Jin et al. confirmed a significant association between GH and elevated PTB risk (OR=1.58, 95% CI: 1.35, 1.85) (16). Similarly, Hu et al. evaluated the 2017 American College of Cardiology/American Heart Association (ACC/AHA) hypertension guideline and found that standardized GH diagnosis was associated with a 1.72-fold higher risk of preterm delivery (95% CI: 1.28, 2.31), underscoring the consistency of this association and the clinical importance of rigorous diagnosis. GH contributes to PTB through mechanisms including placental dysfunction, endothelial injury, and reduced uterine-placental perfusion, and may also necessitate iatrogenic preterm delivery to safeguard maternal and fetal health.
A key novel finding of this study is the significant positive additive interaction between noise exposure and GH on PTB risk, with a RERI of 1.11, an AP of 27.34%, and an S of 1.57. These results indicate that 27.34% of PTB cases in the co-exposed group were attributable to the interaction effect, and the combined exposure exceeded the sum of individual effects. To our knowledge, this is among the first studies to quantify this additive interaction using PSM, thereby addressing confounding bias that has limited previous observational research. The interaction mechanism may involve synergistic amplification of oxidative stress and inflammation: noise exposure induces systemic inflammation and placental vascular damage, while GH further impairs endothelial function and uterine-placental perfusion. Together, these pathways create a "double burden" on fetal development, increasing the likelihood of preterm delivery.
This study has several limitations. First, as a cross-sectional design, it cannot establish definitive causal relationships among noise exposure, GH, and PTB, although PSM reduces confounding bias. Second, occupational noise exposure was primarily based on self-report, with only partial validation through enterprise-level data rather than individual objective monitoring, potentially resulting in exposure misclassification bias. Similarly, data on GH and PTB (including gestational age at delivery) partially relied on self-reported information, which may introduce recall bias. These biases could affect the accuracy of effect estimates and should be considered when interpreting the findings. Third, important potential confounders — including pre-pregnancy body mass index (BMI), gravidity and parity, history of preterm birth, frequency of prenatal care, psychological stress, physical workload, and co-exposure to other occupational hazards — were not adjusted for, which may lead to residual confounding. Fourth, the study population was restricted to female workers in manufacturing and mining industries from four PLADs in China, which may limit the external validity and generalizability of the findings. Therefore, the results should be interpreted with caution and should not be extrapolated to other populations.
In conclusion, occupational noise exposure and GH are independent risk factors for PTB among female workers in manufacturing and mining industries, and their co-occurrence exerts a synergistic additive effect on PTB risk. These findings underscore the need for integrated interventions, including workplace noise control, enhanced GH screening, and targeted care for high-risk subgroups. Future studies employing prospective cohort designs, objective noise measurements, and biological markers are needed to confirm causal relationships and elucidate the underlying mechanisms.
-
Approval by National Institute of Occupational Health and Poison Control, Chinese Center for Disease Control and Prevention (IRB-NIOHP202013).
HTML
| Citation: |

|