
 Download:
Download:




-
Introduction: This study investigated the prevalence, patterns, and risk factors of multi-site work-related musculoskeletal disorders (WMSDs) among workers in key industries across China.
Methods: A total of 88,609 workers from 441 enterprises across 29 industries were surveyed using stratified cluster sampling (2018–2023). The Chinese Musculoskeletal Disorders Questionnaire assessed symptoms. WMSDs were classified as single-site (1 body part), dual-site (2 body parts), triple-site (3 body parts), and over-3-site (>3 body parts). Cross-classified multilevel generalized linear mixed models identified associated factors.
Results: The prevalence of multi-site WMSDs was 26.4%, exceeding that of single-site disorders (11.3%), with multi-site cases comprising 69.9% of all WMSDs. Packaging and printing (28.0%), healthcare (20.5%), and nonferrous metal smelting (20.5%) exhibited the highest prevalence of multi-site WMSDs. Female sex was an independent risk factor for all WMSD types. Higher education levels correlated with increased risk, with a master's degree or above showing the strongest association with triple-site WMSDs. Prolonged standing, prolonged sitting, and fixed postures demonstrated dose–response relationships with WMSD severity. Insufficient rest was associated with the highest risk of multi-site WMSDs.
Conclusion: Multi-site WMSDs represented the predominant pattern among Chinese workers. Prevention strategies should prioritize high-risk industries and target modifiable factors, particularly insufficient rest and prolonged static postures.
-
Work-related musculoskeletal disorders (WMSDs) are conditions involving injuries or dysfunctions of muscles, bones, nerves, joints, tendons, ligaments, and cartilage that are induced or aggravated by occupational hazards such as adverse ergonomic factors during work activities, manifesting as pain, numbness, burning, tingling, limited movement, and related discomfort, thereby seriously threatening worker health (1). According to the Global Burden of Disease study, WMSDs account for 21.30% of disability-adjusted life years (DALYs), ranking third among all diseases (2). Compared with single-site involvement, patients with multi-site WMSDs are more prone to developing severe dysfunction, occupational absenteeism, increased medical burden, and reduced quality of life (3). Although low back pain and neck pain have been identified as major contributors to DALYs in the Global Burden of Disease Study (4), the prevalence pattern of multi-site WMSDs is often underestimated or overlooked in routine epidemiological surveillance. Previous studies have mostly focused on single-site WMSDs or specific high-risk industries, and epidemiological data on multi-site WMSDs based on nationally representative samples remain lacking. Using cross-sectional survey data from 88,609 workers at 441 enterprises across 29 industries provided in
Supplementary Table S1 , this study systematically described the prevalence and distribution characteristics of multi-site WMSDs among occupational populations in China, providing a scientific basis for formulating precise hierarchical and classified intervention strategies.A multistage stratified cluster random sampling approach was adopted. We selected 23 provincial-level administrative divisions (PLADs) across 7 regions, stratified industries by WMSD relevance, workforce size, and economic importance, and then sampled enterprises by size (large/medium/small/micro). Within each enterprise, all eligible frontline workers were cluster-sampled at the workshop level. From 2018 to 2023, 91,560 workers completed the questionnaire (Cronbach's α=0.86) via Quick Response (QR) code, yielding 88,609 valid responses (96.8% response rate). The survey employed a 1∶N format in which one investigator organized N respondents to scan the QR code of the electronic questionnaire and complete the survey online, with further elaboration provided in
Supplementary Figure S1 .The Chinese Version of the Musculoskeletal Disorders Questionnaire, embedded in the Ergonomic Assessment and Analysis System for WMSDs developed by the Department of Occupational Protection and Ergonomics at the National Institute of Occupational Health and Poison Control, was used. The electronic questionnaire included items on general information, musculoskeletal symptoms, and work conditions. The WMSD criteria followed the National Institute for Occupational Safety and Health (NIOSH) definition: the presence of discomfort such as pain, stiffness, burning, numbness, or tingling. Exclusion criteria included congenital spinal deformities and non-WMSD conditions due to trauma, infectious diseases, or malignant tumors, with further elaboration provided in
Supplementary Material . WMSDs were categorized as single-site (1 body part) and multi-site, including dual-site (2 body parts), triple-site (3 body parts), and over-3-site (>3 body parts). All participants provided informed consent, and the study was approved by the Medical Ethics Review Committee of the National Institute of Occupational Health and Poison Control of the Chinese Centers for Disease Control and Prevention (NIOHP202122).SPSS (version 29.0, SPSS Inc, Chicago, IL, USA) was used to characterize the basic demographic and occupational features of the surveyed population. Cross-classified multilevel generalized linear mixed models (CCMM) were employed to examine associations between potential risk factors and WMSDs, accounting for unobserved clustering at both regional and industrial levels. Statistical significance was set at a two-tailed α level of 0.05.
Among the 83,006 respondents, 31,314 had WMSDs (37.7%), including 9,418 with single-site (11.3%) and 21,896 with multi-site (26.4%) disorders. Among multi-site WMSDs, 6,574 were dual-site (20.99%), 4,779 were triple-site (15.26%), and 10,543 were over-3-site (33.67%). Patients with multi-site WMSDs accounted for 69.9% of all WMSD cases, indicating that multi-site involvement represents the predominant manifestation of WMSDs among occupational populations in China (Table 1).
Category n Proportion of total population (%) Proportion of all WMSDs patients (%) Single-site WMSDs (1 body part) 9,418 11.3 30.08 Multi-site WMSDs (≥2 body parts) Dual-site (2 body parts) 6,574 7.9 20.99 Triple-site (3 body parts) 4,779 5.8 15.26 Over-3-site (>3 body parts) 10,543 12.7 33.67 Total 31,314 37.7 100.00 Note: 5,603 non-frontline workers (logistics, office, and management) were excluded from the analysis.
Abbreviation: WMSDs=work-related musculoskeletal disorders.Table 1. Distribution of musculoskeletal disorders by number of affected body parts among occupational populations in China (N=83,006).
Significant variations in multi-site WMSD prevalence were observed across industries. The top three industries for dual-site WMSDs were packaging and printing (20.00%), general aviation services (11.26%), and electricity, heat, gas, and water production and supply (9.30%). For triple-site WMSDs, the top three were packaging and printing (28.00%), healthcare (10.84%), and animal husbandry (10.20%). For over-3-site WMSDs, the leading four were toy manufacturing (26.77%), packaging and printing (26.00%), nonferrous metal smelting and pressing (20.54%), and healthcare (20.54%). Packaging and printing ranked among the high-prevalence industries across all multi-site categories, representing a key high-risk industry for multi-site WMSDs (Figure 1).
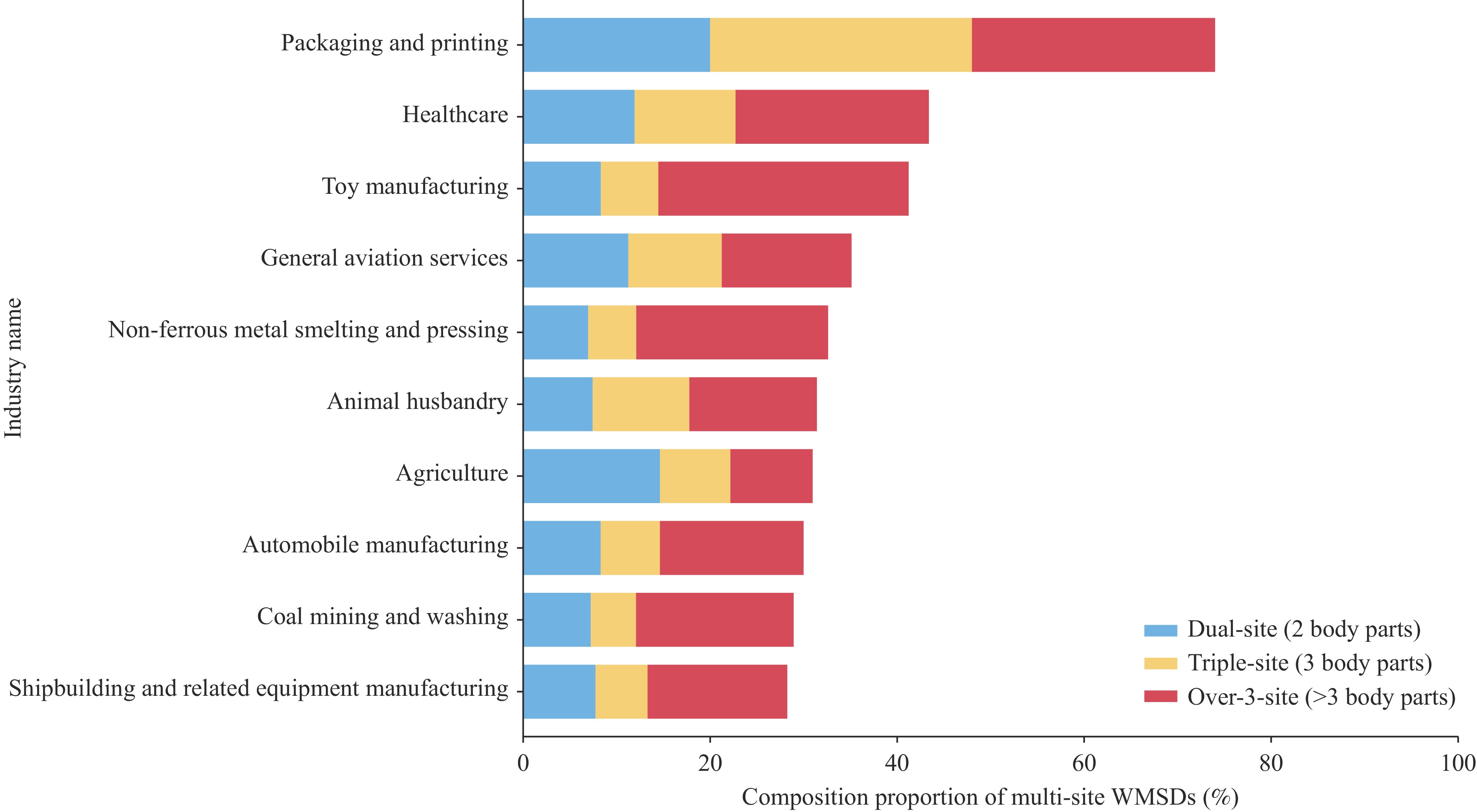 Figure 1.
Figure 1.Top 10 industries with the highest prevalence of multi-site musculoskeletal disorders (n=83,006).
Abbreviation: WMSDs=work-related musculoskeletal disorders.The prevalence of WMSDs by site number is presented in
Supplementary Tables S2–S3 . Cross-classified multilevel generalized linear mixed model (CCMM) analysis revealed that the industry-level intraclass correlation coefficient (ICC) increased with the number of affected body sites, suggesting that the risk of multi-site WMSDs was more strongly influenced by industrial factors. The city-level ICC remained below 4% across all subgroups, reflecting a minor impact of regional disparities. The median odds ratio (MOR) results were consistent with the ICC trends. In addition, sex, age, education, physical exercise, ergonomic exposure, and work organizational factors were significantly associated with WMSD risk at different severity levels, with varying trends in effect strength as the number of affected sites increased (Table 2). Female sex was identified as an independent risk factor for all WMSD types. Using males as the reference group, females had a significantly higher risk for all WMSD types, and the protective effect of male sex increased gradually with disease severity. Age showed a non-linear association with WMSD risk. Using the <30-year group as the reference, the 30–39-year group showed a significantly elevated risk for all WMSDs. Education showed a significant positive correlation with WMSD risk. Using junior high school and below as the reference group, the risk progressively increased with education level. Physical exercise demonstrated protective effects.Variable aOR (95% CI) Single-site
(1 body part)Dual-site
(2 body parts)Triple-site
(3 body parts)Over-3-site
(>3 body parts)Fixed effects Gender Male 1 1 1 1 Female 1.19 (1.12, 1.27) 1.50 (1.40, 1.62) 1.66 (1.52, 1.82) 1.71 (1.60, 1.84) Age (years) <30 1 1 1 1 30–34 1.06 (1.00, 1.13) 1.18 (1.10, 1.27) 1.17 (1.07, 1.28) 1.11 (1.04, 1.19) 35–39 1.12 (1.04, 1.21) 1.15 (1.05, 1.25) 1.21 (1.09, 1.34) 1.17 (1.08, 1.26) 40–44 1.07 (0.98, 1.17) 1.10 (0.99, 1.22) 1.12 (0.99, 1.27) 1.12 (1.02, 1.23) 45–49 1.10 (1.01, 1.21) 0.99 (0.88, 1.11) 0.99 (0.86, 1.14) 1.08 (0.97, 1.19) 50–54 1.02 (0.91, 1.15) 1.05 (0.91, 1.20) 1.11 (0.94, 1.31) 1.04 (0.92, 1.18) 55–59 1.20 (1.01, 1.41) 1.17 (0.95, 1.45) 1.01 (0.77, 1.33) 0.98 (0.80, 1.20) ≥60 0.97 (0.83, 1.13) 1.03 (0.86, 1.23) 1.12 (0.92, 1.37) 1.12 (0.96, 1.30) Education Junior high and below 1 1 1 1 Senior high/technical 1.10 (1.04, 1.18) 1.10 (1.01, 1.19) 1.18 (1.07, 1.30) 1.12 (1.05, 1.20) College and undergraduate 1.29 (1.20, 1.40) 1.29 (1.17, 1.41) 1.43 (1.28, 1.60) 1.23 (1.13, 1.33) Master’s and above 1.44 (1.16, 1.79) 1.49 (1.18, 1.88) 1.60 (1.23, 2.08) 1.08 (0.86, 1.37) BMI (kg/m²) <18.5 1 1 1 1 18.5–23.9 1.00 (0.92, 1.09) 1.00 (0.90, 1.10) 1.09 (0.98, 1.23) 1.02 (0.94, 1.11) 24.0–27.9 1.04 (0.95, 1.14) 1.03 (0.93, 1.15) 1.16 (1.02, 1.31) 1.01 (0.92, 1.11) ≥28.0 1.06 (0.95, 1.19) 1.07 (0.94, 1.22) 1.16 (1.00, 1.35) 1.13 (1.01, 1.26) Physical exercise No 1 1 1 1 Occasionally 0.89 (0.85, 0.94) 0.91 (0.85, 0.96) 0.90 (0.84, 0.96) 0.97 (0.92, 1.03) 2–3 times/month 0.88 (0.78, 0.99) 0.97 (0.85, 1.10) 0.92 (0.79, 1.08) 0.95 (0.84, 1.07) 2–3 times/week 0.82 (0.74, 0.90) 0.85 (0.76, 0.95) 0.86 (0.76, 0.98) 0.89 (0.80, 0.98) >2 times/week 0.82 (0.73, 0.91) 0.84 (0.74, 0.96) 0.64 (0.54, 0.76) 0.84 (0.75, 0.95) Workplace risk factors Standing often at work No 1 1 1 1 Occasionally 1.00 (0.92, 1.09) 1.00 (0.90, 1.10) 1.02 (0.91, 1.14) 0.98 (0.89, 1.07) Frequent 1.10 (1.01, 1.18) 1.20 (1.09, 1.33) 1.13 (1.00, 1.28) 1.10 (1.01, 1.21) Very frequent 1.19 (1.08, 1.30) 1.54 (1.39, 1.72) 1.48 (1.31, 1.68) 1.48 (1.34, 1.63) Sitting often at work No 1 1 1 1 Occasionally 0.92 (0.87, 0.98) 0.92 (0.86, 1.00) 0.91 (0.83, 0.99) 0.88 (0.82, 0.94) Frequent 1.09 (1.01, 1.18) 1.28 (1.17, 1.40) 1.36 (1.23, 1.51) 1.30 (1.20, 1.40) Very frequent 1.19 (1.08, 1.30) 1.56 (1.40, 1.73) 1.80 (1.60, 2.02) 1.63 (1.49, 1.78) Fixed neck posture No 1 1 1 1 Yes 1.21 (1.15, 1.33) 1.50 (1.37, 1.64) 1.55 (1.38, 1.73) 1.40 (1.30, 1.53) Frequent repetitive lower limb/ankle movements No 1 1 1 1 Yes 0.99 (0.94, 1.05) 1.08 (1.02, 1.15) 1.15 (1.07, 1.24) 1.64 (1.56, 1.73) Lifting heavy loads (more than 20 kg) No 1 1 1 1 Occasionally 1.01 (0.95, 1.06) 1.03 (0.96, 1.10) 1.07 (0.99, 1.16) 1.32 (1.25, 1.40) Frequent 0.98 (0.90, 1.07) 1.13 (1.03, 1.25) 1.10 (0.98, 1.24) 1.49 (1.37, 1.61) Very frequent 1.03 (0.92, 1.16) 1.16 (1.02, 1.32) 1.06 (0.91, 1.24) 1.58 (1.43, 1.75) Trunk bending and twisting No 1 1 1 1 Yes 1.11 (1.05, 1.17) 1.09 (1.02, 1.16) 1.26 (1.17, 1.35) 1.49 (1.41, 1.57) Wrist bending No 1 1 1 1 Yes 1.02 (0.97, 1.07) 1.14 (1.07, 1.21) 1.24 (1.16, 1.33) 1.68 (1.59, 1.77) Prolonged fixed back posture No 1 1 1 1 Yes 1.14 (1.08, 1.21) 1.17 (1.09, 1.25) 1.21 (1.11, 1.32) 1.21 (1.14, 1.29) Work organizational factors Frequent overtime No 1 1 1 1 Yes 1.11 (1.05, 1.16) 1.15 (1.08, 1.22) 1.14 (1.06, 1.22) 1.24 (1.18, 1.32) Insufficient rest No 0.72 (0.69, 0.76) 0.63 (0.60, 0.67) 0.54 (0.50, 0.58) 0.44 (0.42, 0.47) Yes 1 1 1 1 Staff shortages No 1 1 1 1 Yes 1.14 (1.08, 1.19) 1.17 (1.10, 1.24) 1.17 (1.09, 1.25) 1.40 (1.33, 1.47) Do same working No 1 1 1 1 Yes 1.18 (1.10, 1.28) 1.12 (1.02, 1.23) 1.43 (1.28, 1.62) 1.36 (1.24, 1.49) Job rotation No 1.00 (0.95, 1.06) 1.03 (0.97, 1.10) 1.06 (0.98, 1.15) 1.14 (1.07, 1.21) Yes 1 1 1 1 Random effects City level ICC (%) 2.78 3.33 3.57 3.09 mOR 1.34 1.38 1.43 1.39 Industry level ICC (%) 1.09 2.15 11.52 10.34 mOR 1.20 1.30 1.89 1.82 Abbreviation: WMSD=work-related musculoskeletal disorders; aOR=adjusted odds ratio; BMI=body mass index; CI=confidence interval; ICC=intraclass correlation coefficient; mOR=median odds ratio. Table 2. Multilevel modeling analysis of WMSDs among frontline workers.
For ergonomic risk factors, very frequent prolonged standing, prolonged sitting, fixed neck posture, trunk bending and twisting, wrist bending, and fixed back posture significantly increased risk for all WMSDs, with the greatest risk amplification observed for multi-site WMSDs.
Among work organizational factors, frequent overtime, insufficient rest, and staff shortage were associated with elevated WMSD risk. Compared with insufficient rest, adequate rest reduced the risk of multi-site WMSDs. Performing the same work repeatedly increased the risk of all WMSDs, whereas job rotation showed a protective effect against over-3-site WMSDs.
-
From 2018 to 2023, all annual surveys adopted a standardized research protocol and questionnaire. Therefore, all valid data were pooled for comprehensive analysis to enhance statistical power. The prevalence of multi-site WMSDs among occupational populations in China reached 26.4%, substantially exceeding the single-site prevalence (11.3%), with multi-site cases accounting for 69.9% of all WMSDs. This finding indicates that multi-site WMSDs are highly prevalent and cause functional impairment, medical burden, and productivity loss that exceed those of single-site disorders.
Regarding industry distribution, packaging and printing ranked among the high-prevalence industries for dual-site, triple-site, and over-3-site WMSDs, suggesting that high-intensity repetitive operations and prolonged fixed postures characterize this industry. The healthcare and nonferrous metal smelting and pressing industries displayed over-3-site WMSD prevalence exceeding 20.5%, likely related to occupational characteristics (5) that contribute to cumulative multi-site musculoskeletal damage. In toy manufacturing, the prevalence of over-3-site WMSDs reached 26.77%. Given the relatively small sample size of this industry, these results cannot be generalized.
Based on CCMM analysis, female sex was identified as an independent risk factor for all WMSD types, and the sex difference became increasingly pronounced with a greater number of affected body sites. Compared with males (reference group), the adjusted odds ratios (aOR) for females were 1.19, 1.50, 1.66, and 1.71 for single-site, dual-site, triple-site, and over-3-site WMSDs, respectively. This finding aligns with the Global Burden of Disease study and previous occupational health surveys (2,6) and may relate to lower spinal load-bearing capacity in females, hormonal differences, and the dual burden of domestic labor. Accordingly, strengthening gender-targeted protection strategies for female workers is critical, with focused attention on the prevention and intervention of multi-site musculoskeletal disorders in high-risk female populations. Education was positively correlated with WMSD risk, with the strongest dose–response relationship observed for triple-site WMSDs (master’s degree and above: aOR=1.60), possibly because highly educated individuals more frequently engage in sedentary work, experience greater psychological stress, and hold higher occupational expectations (7). Highly educated employees predominantly engage in prolonged sedentary work with long-term static loading, causing sustained tension of the cervical, shoulder, lumbar, and wrist muscles, local microcirculation disturbance, metabolic by-product accumulation, and chronic fascial strain, thereby increasing physiological susceptibility to multi-site musculoskeletal injuries. They also face heavy work pressure; chronic stress alters somatic nerve excitability, induces muscle contraction, and reduces pain tolerance, while higher career expectations reduce recovery time, leading to cumulative adverse occupational exposure.
Ergonomic factors demonstrated significant dose–response relationships between adverse posture exposure and WMSD risk. Very frequent prolonged standing and sitting exhibited the strongest effects for multi-site WMSDs (≥2 body parts) (aOR>1.4), while prolonged fixed neck and back postures displayed the most prominent effects for over-3-site WMSDs (aOR=1.55 and 1.21, respectively). This confirms that multi-site WMSDs are not simple additions of single-site disorders but result from systemic ergonomic load accumulation, with cumulative adverse ergonomic exposure serving as the core driver of multi-site damage (8). Frequent repetitive lower limb/ankle movements shifted from protective for single-site WMSDs (aOR=0.99) to a risk factor for over-3-site WMSDs (aOR=1.64), further confirming the unique pathogenic pattern of multi-site WMSDs.
Among work organization factors, sufficient rest was the strongest protective factor for all WMSDs, with the most pronounced association identified for over-3-site WMSDs (aOR=0.44). Adequate rest can effectively relieve musculoskeletal strain and reduce cumulative occupational physical damage (9). Physical exercise also served as a protective factor against WMSDs. Therefore, increasing physical activity is recommended to reduce the incidence of WMSDs.
This study has two major strengths. The large sample size ensures good representativeness of the occupational population, and the use of validated standardized tools fills the domestic multi-site WMSD data gap with sound external validity.
In conclusion, future interventions should prioritize the following: first, industry-specific interventions for printing and toy manufacturing should reduce repetitive motions through automation while optimizing ergonomic design; for healthcare, mandatory implementation of rest break systems and proper patient-handling technique training are essential; and finally, multi-site WMSDs should be incorporated into China’s occupational disease surveillance system to dynamically monitor high-risk industry trends and precisely target prevention priorities.
The findings in this report are subject to at least three limitations. First, the cross-sectional design cannot establish causal relationships between risk factors and WMSDs; it captures only associations at a single point in time, which may introduce temporal ambiguity regarding exposure and outcome sequences. Second, retrospective self-reporting of symptoms may involve recall bias, potentially leading to underestimation or overestimation of symptom severity and affecting the accuracy of associations between exposures and outcomes. Finally, the study focused on frontline operational personnel, which may limit generalizability to other occupational populations such as administrative staff or management personnel.
These findings highlight that multi-site WMSDs constitute the predominant pattern of WMSDs among occupational populations in China. Targeted prevention strategies should prioritize high-risk industries, including packaging and printing, toy manufacturing, and healthcare. This study suggests that implementing standardized rest break policies and reducing prolonged static postures can effectively prevent multi-site WMSDs. Workplace interventions should focus on modifiable ergonomic risk factors, with key protective measures tailored for female workers. In line with International Labour Organization occupational safety guidelines, China should integrate multi-site WMSDs into the national occupational disease surveillance system and strengthen legal safeguards for targeted preventive interventions.
-
We sincerely thank all participants involved in this study from the Centers for Disease Control and Prevention of Shanghai, Jiangsu, Zhejiang, Tianjin, Beijing, Hubei, Ningxia Hui Autonomous Region, Sichuan, and Shaanxi; Yunnan Provincial Hospital of Integrated Chinese and Western Medicine, Guangzhou Twelfth People's Hospital Affiliated to Guangzhou Medical University, Liaoning Provincial Health Supervision Center, Shenyang, Liaoning, China, Guizhou Province Occupational Disease Prevention and Control Hospital, Shandong Academy of Occupational Health and Occupational Medicine, Civil Aviation Medical Center of China Civil Aviation Administration, Tianjin Occupational Disease Prevention and Control Hospital, Fujian Province Occupational Disease and Chemical Poisoning Prevention and Control Center, Guangdong Province Hospital for Occupational Disease Prevention and Treatment, and Institute of Occupational Medicine of Jiangxi.
HTML
| Citation: |

|