
 Download:
Download:




-
Introduction: From September 2023 to November 2025, a cluster outbreak of active tuberculosis (TB) was identified at a university in Changsha City, Hunan Province, China.
Methods: Contacts were screened, and patients with positive etiological results underwent sputum culture and drug susceptibility testing. Environmental samples (from air conditioners and air) were collected after terminal disinfection for polymerase chain reaction testing. A quantitative analysis of the infection risk was performed using linear regression models. Preventive intervention treatment effectiveness was evaluated using the log-rank test and Cox proportional hazards regression model.
Results: Of 671 contacts [110: latent tuberculosis infection (LTBI); 25: new active TB], all 26 cases, including the index case, were students. Whole-genome sequencing of five culture-positive cases showed high homology with ≤3 single nucleotide polymorphisms for four of them. For each additional hour of contact with the index patient, the prevalence of LTBI among contacts increased by 0.48%, and the TB incidence among individuals with LTBI increased by 0.20%. Developing active TB among individuals with LTBI who received Mycobacterium vaccae immunotherapy was 0.10 times that of the control group, the cumulative incidence within 2 years remained as high as 10.67%. Terminal disinfection of the epidemic sites was incomplete, and M. tuberculosis was detected in the air conditioner filters and air samples from the index case classroom and dormitory.
Conclusion: Contributing factors were failure to detect the index case during the new student entrance health examination, incomplete terminal disinfection of epidemic sites, and lack of follow-up monitoring of individuals with LTBI who received preventive immunotherapy.
-
Tuberculosis (TB) is a chronic infectious respiratory disease that poses a serious threat to public health. In 2024, the number of new TB cases worldwide reached 10.7 million, with 1.23 million deaths, ranking as the leading cause of death among infectious diseases (1). In crowded school settings with enclosed spaces, students have frequent close contact, which can facilitate the transmission of TB on campus (2). China has long attached great importance to TB prevention and control in schools. A series of documents have been issued to promote standardized and systematic prevention and control efforts to achieve significant results (3). However, several weaknesses remain in the current practice: first, accreditation standards and quality evaluation mechanisms for institutions conducting TB screening during new student entrance health examinations are not yet robust (4); second, there is a lack of scientific evaluation of the effectiveness of terminal disinfection at epidemic sites after an outbreak occurs (5); and third, requirements for long-term follow-up and effective monitoring for individuals with latent tuberculosis infection (LTBI) who have completed preventive treatment are not clearly defined (6). Evaluating the effectiveness of terminal disinfection is important because M. tuberculosis can persist at overlooked sites (e.g., air conditioner filters) and continue to pose infection risks in enclosed spaces if disinfection is incomplete (7). Likewise, evaluating the long-term outcomes of preventive immunotherapy is necessary as the durability of protection remains unclear and individuals who complete preventive treatment may still develop active TB without adequate follow-up (8). Between September 2023 and November 2025, a prolonged, large-scale cluster outbreak of TB was reported at a university in Changsha City, Hunan Province, China. Through an in-depth investigation of the outbreak, this study aimed to systematically describe its epidemiological characteristics, evaluate the effectiveness of terminal disinfection at epidemic sites and preventive treatment, analyze the relationship between infection/incidence risk and exposure duration, use empirical evidence to reveal key issues in current school TB prevention and control, and provide scientific evidence and management recommendations for optimizing prevention and control strategies.
-
The index case was an 18-year-old male freshman majoring in physical education in class 2301, residing in room 419, Building 11 West. During his entrance health examination on September 10, 2023, the examination institution determined that his chest radiograph showed no abnormalities. However, upon re-reading by experts from the local municipal CDC and designated TB hospital, abnormal findings were identified on the chest radiographs.
He developed a productive cough on November 15, 2023, followed by progressive worsening of the cough and hemoptysis. From December 3 to December 18, 2023, he was treated for influenza A and pneumonia at two non-TB designated hospitals; however, his symptoms worsened. On December 19, 2023, he sought treatment at Hunan Provincial Chest Hospital and was diagnosed with cavitary pulmonary TB (sputum smear-positive 2+, rifampicin-susceptible), where his chest imaging findings revealed patchy high-density opacities in the dorsal segment of the right lower lobe, accompanied by a thick-walled cavity with smooth walls and no visible air-fluid level, surrounded by patchy satellite lesions. On December 22, 2023, the Centers for Disease Control and Prevention initiated an epidemiological investigation after receiving the report. The investigation revealed that he had classmates with TB in high school.
-
Among the 671 contacts, 110 individuals with LTBI were identified (Table 1), including 70 males, 40 females, 103 students, and seven staff members.
Screening Contact type Number of contacts (n) Number of LTBI (n) Prevalence of LTBI among contacts (%) Number of secondary cases (n) TB incidence among individuals with LTBI (%) Average exposure duration (hours) First-round Class 2301: Classmates of the index case 24 23 95.83 10 43.48 213.0 Class 2301: Teachers of the index case 8 2 25.00 0 0.00 14.8 Class 2302: Shared a classroom concurrently and self-study together 23 20 86.96 8 40.00 172.5 Second-round Class 2307: Shared a classroom concurrently 24 18 75.00 3 16.67 100.5 Class 2306: Shared a classroom concurrently 22 6 27.27 1 16.67 73.5 Class 2303: Shared a classroom concurrently 24 3 12.50 0 0.00 73.5 Third-round Same dormitory floor; Used the classroom later; Dormitory management staff 546 38 6.96 3 7.89 – Total 671 110 16.4 25 22.7 – Note: “–” means no direct contact with the index case.
Abbreviation: LTBI=latent tuberculosis infection; TB=tuberculosis.Table 1. Details of contact screening.
In total, 26 active TB cases (including the index case) were identified (13 confirmed pulmonary TB, 11 clinically diagnosed pulmonary TB, 2 extrapulmonary TB), all were students (18 males, 8 females), of whom 17 were asymptomatic (65.38%). The outbreak began with the first case identified in September 2023 and was followed by a gradual increase.
Two secondary case peaks occurred in January and April 2024. The outbreak subsided from August 2024 to July 2025 but resurged in August 2025, with a third peak in September 2025. The last case occurred in November 2025, with an outbreak duration of 28 months (Figure 1). The temporal distribution of cases was closely aligned with the timing of each screening round. Most individuals with LTBI and secondary cases were identified during the first and second rounds of screening, suggesting that contact identification was accurate. During the third round, the infection rate among contacts was only 6.96%, indicating that further expansion of screening is of limited necessity.
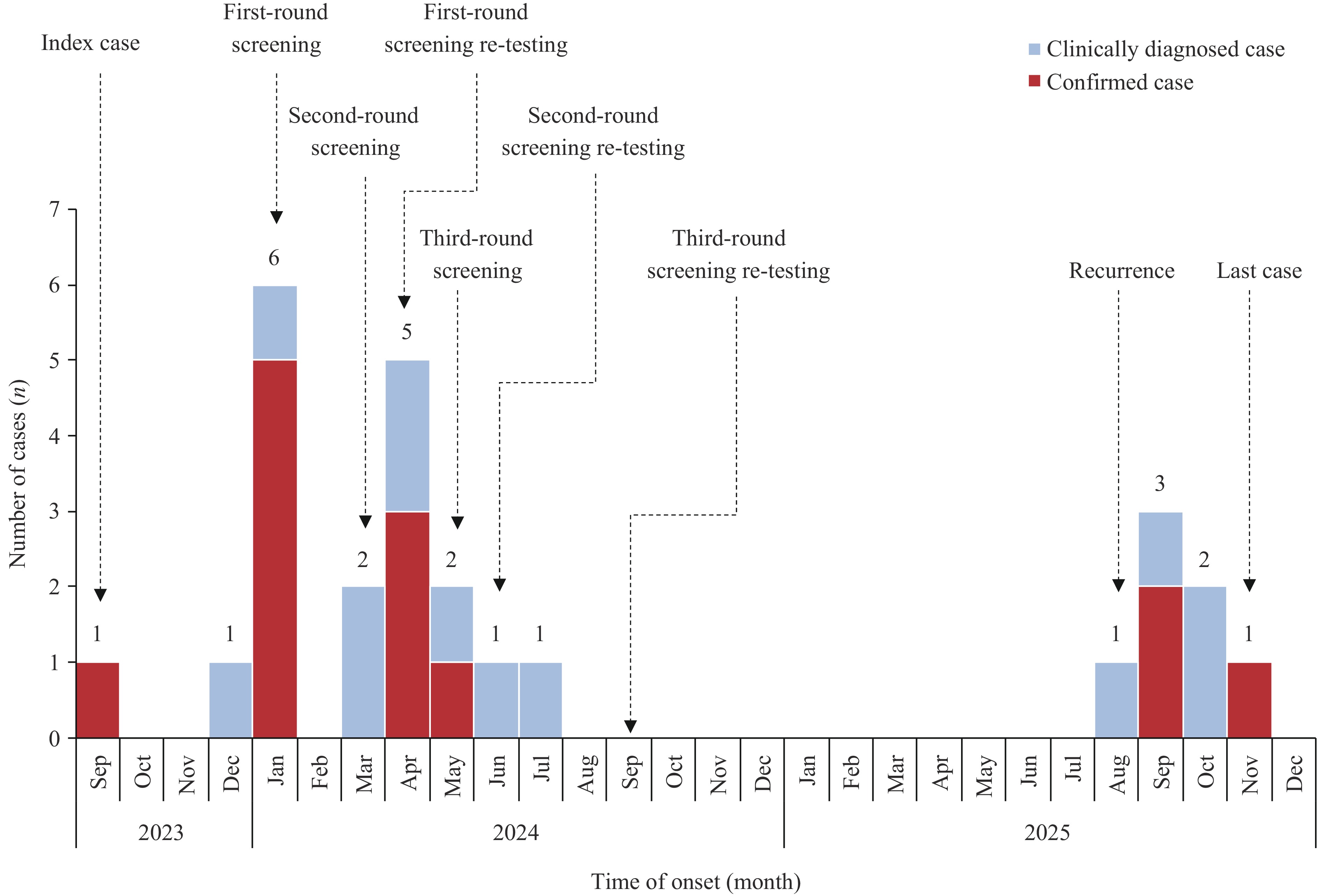 Figure 1.
Figure 1.Epidemiological curve of a TB outbreak in Changsha City, Hunan Province, China, September 2023–November 2025.
Abbreviation: TB=tuberculosis. -
Among individuals with LTBI, 35 did not receive preventive treatment (control group), with a 2-year cumulative incidence of 45.71%, which was concentrated in the early follow-up period. Seventy-five patients received Mycobacterium vaccae immunotherapy (intervention group), with a 2-year cumulative incidence rate of 10.67%. The intervention group had a lower risk in the early follow-up period; however, this risk increased significantly in the later period. log-Rank test results showed that the 2-year cumulative incidence in the intervention group was lower than that in the control group (χ2=23.27, P<0.01). The multivariable Cox proportional hazards regression model results, after adjusting for gender and age, showed that the hazard ratio (HR) in the intervention group was 0.10 [95% confidence interval (CI): 0.04, 0.25] compared with the control group, indicating that the 2-year cumulative incidence risk in the intervention group was 0.10 times or 90.04% reduced risk that of the control group (Figure 2).
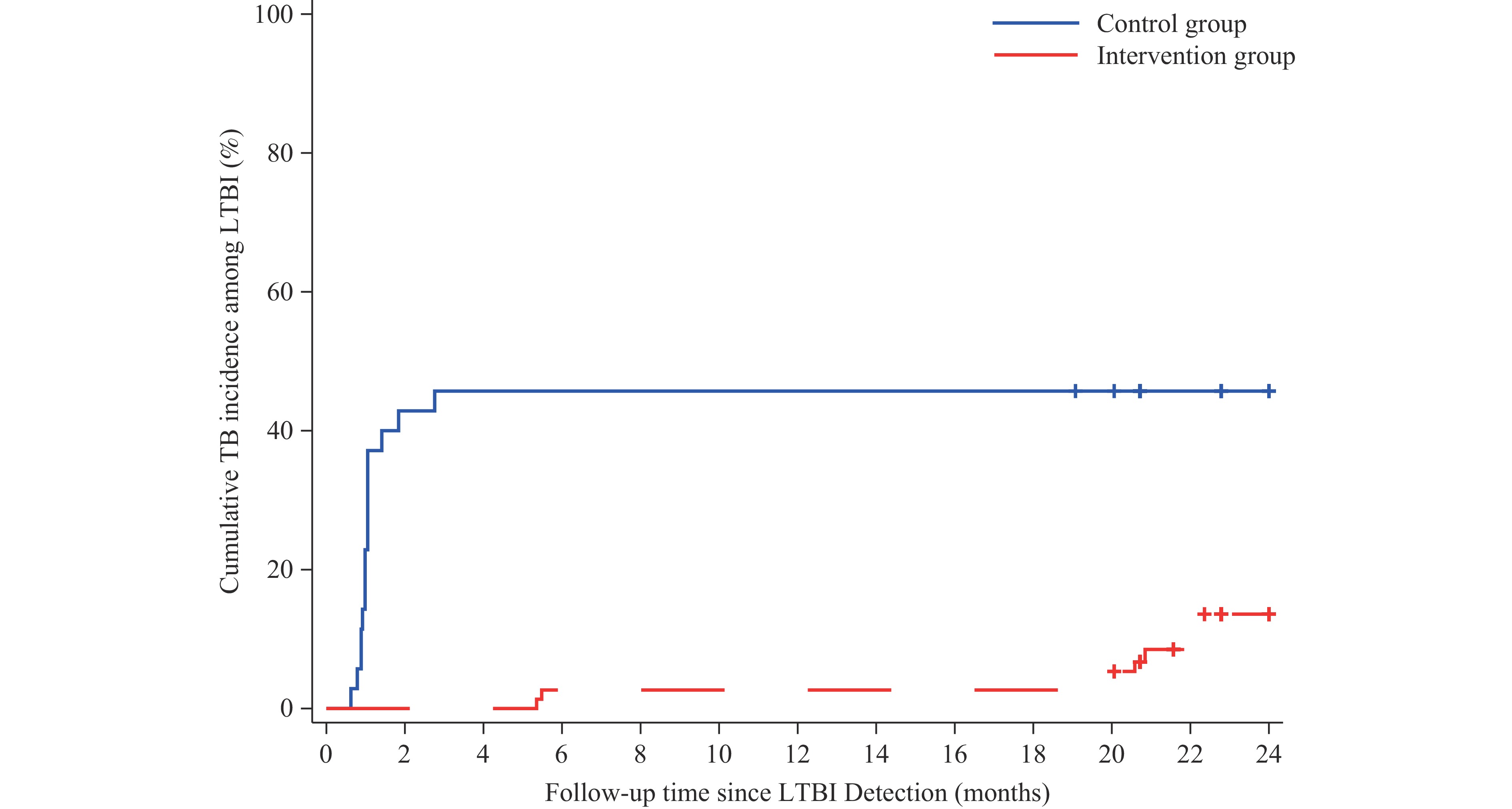 Figure 2.
Figure 2.Survival analysis of preventive treatment in individuals with LTBI.
Abbreviation: LTBI=latent tuberculosis infection; TB=tuberculosis. -
The ventilation conditions in the classrooms and dormitory where the cases occurred were poor, with no fans or air conditioners installed. In April 2024, the local CDC investigation found that the university had completed terminal disinfection of the epidemic sites but had missed air conditioner filters, suggesting that M. tuberculosis may persist in the environment. To test this hypothesis, laboratory staff collected environmental samples (air conditioner filters and air) from four of the nine classrooms and five of the 15 dormitory rooms involved in the outbreak. M. tuberculosis was detected in air conditioner filter samples from all 4 classrooms and 5 dormitory rooms, and in air samples from 2 dormitory rooms. Among the 25 secondary cases, all were contacts of the index case, sharing the same classroom, dormitory, or dormitory floor, or using the same classroom after the index case. Their environmental exposure settings were identical or similar to those of the index case; therefore, the environmental hygiene conditions were not described separately.
-
The ventilation conditions in the classrooms and dormitory where the cases occurred were poor, with no fans or air conditioners installed. In April 2024, the local CDC investigation found that the university had completed terminal disinfection of the epidemic sites but had missed the air conditioner filters, suggesting that M. tuberculosis may persist in the environment. To test this hypothesis, laboratory staff collected environmental samples (air conditioner filters and air) from four of the nine classrooms and five of the 15 dormitory rooms involved in the outbreak. M. tuberculosis was detected in air conditioner filter samples from all 4 classrooms and 5 dormitory rooms, and in air samples from 2 dormitory rooms. Among the 25 secondary cases, all were contacts of the index case, sharing the same classroom, dormitory, or dormitory floor, or using the same classroom after the index case. Their environmental exposure settings were identical or similar to those of the index case; therefore, the environmental hygiene conditions were not described separately.
-
The school TB outbreak involved 26 cases. After its occurrence, comprehensive prevention and control measures were implemented, resulting in no deaths or serious negative social impacts. According to the Chinese School Tuberculosis Prevention and Control Guidelines (2020 Edition) (Guidelines 2020) (3), this incident was determined to be a cluster outbreak of PTB in schools.
This outbreak reflects three urgent issues that need to be addressed:
First, the accreditation standards and quality evaluation mechanisms for institutions conducting TB screening during new student entrance health examinations are not yet robust (4). Since 2017, TB screening has been included as a mandatory component of entrance health examinations in China for new students, and routine health examinations for faculty and staff in all types of schools, effectively preventing patients with TB from transmitting the disease on campus (9). However, it is noteworthy that the current accreditation standards for entrance health examination institutions are low, leading to uneven quality. TB cluster outbreaks caused by lax screening at entrance examination institutions are common. The health examination institution involved in this outbreak did not participate in the quality control training organized by the local CDC. It conducted TB screening for approximately 9,000 new students at this university but reported no abnormalities. This institution’s failure to detect abnormalities in the index patient’s chest radiograph was a key reason for the development of this cluster outbreak. Therefore, it is necessary to issue national or local regulations to raise the accreditation threshold for health examination institutions, clarify their capacity limits, participate in mandatory local CDC training for TB screening institutions, and establish penalty standards for missed diagnoses.
Second, there are no requirements for evaluating the effectiveness of terminal disinfection at epidemic sites (5). M. tuberculosis is resistant to acid, alkali, natural environments, and drying and can survive in dried sputum for 6 to 8 months. Failure to disinfect air conditioner filters during terminal disinfection at schools was a significant factor in the prolonged outbreak. When teachers and students at the epidemic sites turned on air conditioners and closed windows and doors, classrooms and dormitory spaces became enclosed, creating favorable conditions for disease transmission. Environmental sample testing results showed that M. tuberculosis was detected in air conditioner filters and air from classrooms and dormitories where cases occurred (7), indicating that individuals at these sites faced a continued risk of infection. Currently, the Guidelines 2020 do not mention air conditioner filters in their list of disinfection targets and do not require an evaluation of terminal disinfection effectiveness (5).
Third, the follow-up monitoring requirements for individuals with LTBI who have completed preventive treatment require urgent revision. According to the Guidelines 2020, individuals with LTBI who refuse preventive treatment should undergo chest radiography examinations at 3, 6, and 12 months after screening. However, patients who complete preventive treatment are only required to undergo one chest radiography at the end of the treatment course (3). This outbreak investigation found that compared with the control group, the intervention group receiving preventive immunotherapy had a 90.04% reduced risk of developing active TB. However, the cumulative incidence within two years in the intervention group was still as high as 10.67%. The risk in the intervention group was low in the early intervention period, but rebounded significantly after one year. As an immunomodulator, the protective effect of Mycobacterium vaccae depends on the quantity and function of memory T cells in the body. In the absence of sustained stimulation by pathogens or antigens, memory T cells gradually undergo apoptosis (8). Therefore, it is necessary to increase the frequency of follow-up monitoring of individuals who have completed preventive immunotherapy to prevent renewed outbreaks due to delayed case detection.
Therefore, we propose: 1) Raise accreditation threshold for entrance screening institutions, enforce penalties for missed diagnoses, and strengthen quality control. 2) Require environmental sampling, including air conditioner filters, after terminal disinfection at outbreak sites to confirm M. tuberculosis elimination. 3) For LTBI individuals completing preventive immunotherapy, conduct chest imaging follow-ups (e.g., at 6, 12, and 24 months) to detect active TB cases that may arise due to waning immunity. 4) Tier contact management by exposure duration: longer exposure warrants more frequent screening and prioritization for preventive treatment, whereas shorter exposure allows a simplified protocol.
For details on Methods, Overview of the School, Spatial Distribution Description, Quantitative Analysis of Infection Risk and Disease Onset Risk, Laboratory Investigation, Supplementary Discussion, see the
supplementary materials . -
All field epidemiologists, laboratory personnel and imaging staff involved in the investigation and response to this outbreak.
HTML
Description of the Index Case
Distribution of Cases and LTBI
Evaluation of Preventive Treatment Effectiveness
Environmental Health Investigation
| Citation: |

|