
 Download:
Download:




-
Introduction: Rabies is an animal-borne infectious disease caused by the rabies virus, with a case fatality rate of nearly 100%. This study aimed to evaluate the safety and efficacy of an anti-rabies virus monoclonal antibody ormutivimab in patients aged <18 years with category III rabies exposure.
Methods: This randomized, double-blind, non-inferiority clinical trial was conducted in individuals aged <18 years with category III rabies exposure. Participants were randomized in a 1∶1 ratio to the omertivir monoclonal antibody or human rabies immunoglobulin (HRIG) group. On the day of enrollment (day 0), after thorough wound cleaning, participants received either the monoclonal antibody or HRIG, along with human rabies vaccine co-administration. Follow-up was conducted for 1 year after completion of the full vaccination regimen. Venous blood samples were collected on days 0, 3, 7, 14, and 42 to compare seroconversion rates and rabies virus-neutralizing antibody activity between the two groups. Survival status within 1 year after completion of vaccination and the incidence of adverse events within 30 days were also assessed.
Results: A total of 240 participants were enrolled. The safety results showed that the incidences of adverse events in the ormutivimab and HRIG groups were 53.78% and 59.17%, respectively, with related adverse event rates of 40.34% and 48.33%, respectively. The efficacy results demonstrated the following: 1) For individuals with serum rabies virus neutralizing antibody activity <0.5 IU/mL prior to drug administration (mFAS1), on day 3 post-administration, the antibody seroconversion rate in the omeltivir group was similar to that in the HRIG group. By day 7, the omeltivir group showed significantly higher antibody seroconversion rates than the HRIG group (P=0.0312). By days 14 and 42 post-administration, both groups achieved 100% seroconversion rates. Additionally, on day 3 post-administration, the geometric mean concentrations (GMC) levels in the omeltivir group were significantly lower than those in the HRIG group (P=0.0087). By day 7, GMC levels in both groups were comparable with no significant difference (P=0.2540). By days 14 and 42, omeltivir group antibody GMC levels were significantly higher than those in the HRIG group (P<0.0001). 2) Survival rates remained 100% up to 1 year in both groups after completing the full vaccination regimen.
Conclusions: The combination of ormutivimab and the human rabies vaccine achieved an efficacy endpoint for post-exposure prophylaxis in individuals <18 years of age with category III rabies exposure and demonstrated a favorable safety profile.
-
Rabies is a severe zoonotic infectious disease that remains almost uniformly fatal once clinical symptoms onset (1). Despite the availability of effective post-exposure prophylaxis (PEP), rabies continues to pose a substantial public health burden, particularly in low- and middle-income settings (2). Children and adolescents are at high risk for rabies exposure and have a high incidence of the disease. According to the World Health Organization (WHO) statistics, individuals aged <15 years account for 40% of rabies cases (3). Furthermore, children are more likely than adults to suffer severe injuries from rabies exposure, particularly those affecting the head, face, neck, and perineal regions. These areas are more vulnerable than other areas to viral invasion due to their proximity to the brain and high neural innervation. The WHO recommends that exposure in these areas be classified as category III exposure (4), requiring comprehensive PEP.
Category III rabies exposure in this clinical trial was defined as single or multiple penetrating skin bites or scratches, licking of broken skin, contamination of mucous membranes by animal saliva, or exposure to bats on the head, face, neck, hands, and external genitalia; this aligns with the national technical guidelines (5), and requires a combination of immediate wound management, passive immunization, and active vaccination.
Passive immunization plays a critical role during the early post-exposure period by providing neutralizing antibodies immediately before vaccine-induced immunity is established. Traditionally, passive immunization relies on human or equine rabies immunoglobulins. However, the availability, cost, and batch-to-batch variability of immunoglobulin products limit their widespread use. Since 2018, the WHO has recommended the use of monoclonal antibodies as an alternative to immunoglobulins for PEP (1). Recombinant monoclonal antibodies offer several potential advantages, including standardized manufacturing, consistent potency, and improved supply security.
Currently, clinical evidence for anti-rabies monoclonal antibodies (mAbs) is largely limited to adults. In China, only two types of rabies mAbs are available for individuals aged ≥18 years with category III exposure, leaving an important evidence gap in children and adolescents. To address this gap, we conducted a randomized, double-blind, active-controlled phase III clinical trial to evaluate the immunogenicity and safety of ormutivimab, a recombinant human anti-rabies monoclonal antibody, compared with human rabies immunoglobulin (HRIG) when administered in combination with standard rabies vaccination in individuals aged <18 years with category III rabies exposure.
This study was approved by the Vaccine Clinical Trial Ethics Committee of the Yunnan Provincial Centre for Disease Control and Prevention. The trial was registered in the Drug Clinical Trial Registration and Information Disclosure Platform (CTR20201247).
This randomized, double-blind, active-controlled phase III clinical trial was conducted at four centers for disease control and prevention in Yunnan Province, China, between August 2021 and June 2023. Eligible participants were individuals aged <18 years with category III rabies exposure who had not previously received a rabies vaccination. The inclusion and exclusion criteria are listed in
Supplementary Table S1 .Participants were randomized in a 1∶1 ratio to receive either ormutivimab (treatment group) or HRIG (control group). Randomization was stratified by study site.
On day 0, participants received either ormutivimab or HRIG as passive immunization. Both groups received the same batch of a commercially available human rabies vaccine administered intramuscularly on days 0, 3, 7, 14, and 28 in accordance with the national guidelines. Participants were followed up for 1 year after completion of the full vaccination regimen.
Ormutivimab and HRIG were administered via wound infiltration injection at a dose of 20 IU/kg. If residual volume remained after infiltration injection of all wounds, it was injected into muscle away from the vaccination site (recommended injection sites: for wounds above the waist, into the ipsilateral back muscle group; for wounds below the waist, into the ipsilateral middle lateral thigh muscle group).
In accordance with the requirements of the Center for Drug Evaluation of the National Medical Products Administration and the results of previous studies, the sample size was determined based on safety considerations. Enrolling 100 participants in the experimental group yielded an 80% likelihood of detecting at least one adverse event, with an incidence rate of 1.6%. Accounting for a 20% dropout rate, the trial and control groups planned to enroll 120 participants each, totaling 240 participants.
All adverse events occurring within 30 days of completion of the full immunization regimen were recorded. Adverse events were graded according to the adverse event grading guidelines issued by the National Medical Products Administration (6) and coded using the Medical Dictionary for Regulatory Activities (version 25.0, ICH, Herndon, USA).
Safety analyses included all participants who received at least one dose of the study drug.
Venous blood samples were collected from all the participants on days 0, 3, 7, 14, and 42. Blood samples were collected on day 0 before the trial drug and vaccine administration, and on days 3, 7, and 14 before vaccine administration. The Rapid Fluorescent Foci Inhibition Test, recommended by the WHO, was then performed to determine rabies virus neutralizing antibody (RVNA) activity (1). RVNA was measured by JOINN Laboratories Co. Ltd. (China).
Seroconversion rates and corresponding 95% confidence intervals were calculated for each group on days 3, 7, 14, and 42 post-administration. The geometric mean concentrations (GMCs) of RVNA were calculated after logarithmic transformation of the antibody titers.
Seroconversion rates between the groups were compared using the chi-square test or Fisher’s exact test, as appropriate. All statistical analyses were performed using SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA). Statistical significance was assessed using two-sided tests, with a significance level of 0.05.
A total of 240 participants were randomized between August 2021 and June 2023, as shown in Figure 1. One participant in the treatment group who had received outpatient immunoglobulin was excluded, resulting in 239 participants.
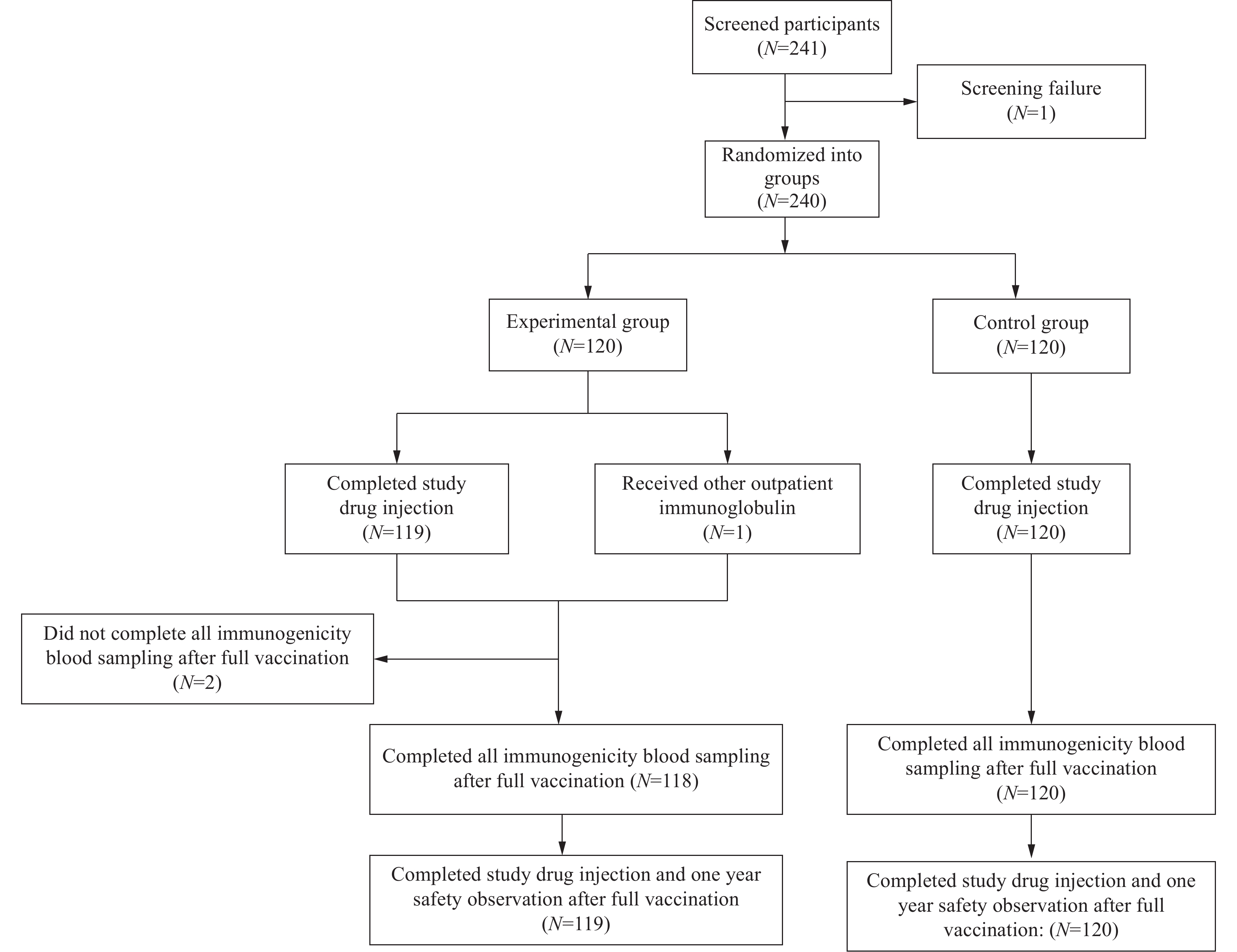 Figure 1.
Figure 1.Distribution diagram of participants.
No significant differences were noted in sex, body mass index, type of biting animal, wound location, and exposure duration between the two groups (P>0.05), indicating a balanced distribution. The primary animal species involved in exposure was dogs (73.95% and 73.33%, respectively), with the most common exposure sites being the limbs, particularly the right upper limb (36.97%). The detailed statistical results are presented in Table 1.
Variables Ormutivimab (N=119) HRIG (N=120) P Sex, n (%) 0.4784 Male 64 (53.78) 70 (58.33) Female 55 (46.22) 50 (41.67) Age Mean (SD) 7.23 (3.46) 8.58 (3.98) 0.0057 Median 6.75 8.44 BMI (kg/m2) 0.3496 Mean (SD) 16.62 (2.57) 16.95 (2.96) Median 15.94 16.01 Biting animals 0.9139 Dog 88 (73.95) 88 (73.33) Cat 31 (26.05) 32 (26.67) Duration between exposure and informed consent (h) 0.5659 Mean (SD) 13.32 (6.79) 12.81 (7.02) Median 15.40 15.29 Wound site, n (%) Head 0 (0.00) 0 (0.00) 1.0000 Face 3 (2.52) 9 (7.50) 0.0780 Neck 0 (0.00) 0 (0.00) 1.0000 Truncus 7 (5.88) 4 (3.33) 0.3471 Left upper limb 36 (30.25) 35 (29.17) 0.8543 Right upper extremity 44 (36.97) 36 (30.00) 0.2533 Left lower extremity 10 (8.40) 22 (18.33) 0.0242 Right lower limb 19 (15.97) 19 (15.83) 0.9776 Others 2 (1.68) 1 (0.83) 0.6218 Note: FAS1 means the full analytical set for neutralizing antibody activity consisted of 239 participants, including 119 in the ormutivimab group and 120 in the HRIG group.
Abbreviation: HRIG=human rabies immunoglobulin.Table 1. Baseline characteristics of all enrolled participants (FAS1, N=239).
The mean ages of the participants in the ormutivimab and HRIG groups were 7 and 8 years, respectively, with a significant age difference between the two groups (P<0.05). In the following analysis, the participants were divided into three subgroups: 1–5, 6–11, and 12–17 years. No significant difference was noted in positivity rates among age groups at 3 days post-administration; however, at 7 days post-administration, the positivity rate in the 12–17 age group was significantly lower than that in the 1–5 and 6–11 age groups. At 14 and 42 days post-administration, the antibody positivity rate was 100.00% in both the experimental and control groups across all age groups (
Supplementary Table S2 ). On days 3 and 7 post-administration, no significant difference in antibody GMC was observed between the two groups across different age groups, with similar trends. On days 14 and 42 post-administration, the antibody GMC in the 1–5 age group of the experimental group showed a difference of more than 18 IU/mL compared with the 6–11 and 12–17 age groups. No significant differences were observed between age groups in the control group (Supplementary Table S3 ).Within 30 days of treatment, the overall incidence of adverse events, treatment-related adverse events, and the distribution of adverse event severity were similar between the groups, with lower rates observed in the ormutivimab group (Table 2). Most adverse events were mild or moderate (grade 1 or 2). No grade 4 or 5 adverse events were reported in either group. The most frequently reported adverse reactions (incidence ≥10%) in both groups were injection-site swelling and pyrexia.
Adverse events Ormutivimab (N=119) HRIG (N=120) Number Incidence rate (%) Number Incidence rate (%) Adverse events, overall 64 53.78 71 59.17 Severity of adverse events Adverse events of category I severity 24 20.17 27 22.50 Adverse events of category II severity 36 30.25 40 33.33 Adverse events of category III severity 4 3.36 4 3.33 Adverse events of category IV severity 0 0.00 0 0.00 Adverse events of category V severity 0 0.00 0 0.00 Adverse reactions with an incidence rate of ≥10% Injection-site swelling 28 23.53 31 25.83 Pyrexia 18 15.13 16 13.33 Injection site pain 11 9.24 14 11.67 Injection site erythema 6 5.04 12 10.00 Note: FAS1 means the full analytical set for neutralizing antibody activity consisted of 239 participants, including 119 in the ormutivimab group and 120 in the HRIG group.
Abbreviation: HRIG=human rabies immunoglobulin.Table 2. Summary of adverse events (FAS1, N=239).
Among participants with baseline RVNA levels <0.5 IU/mL (mFAS1 population), the seroconversion rates increased over time in both groups following administration of passive immunization and rabies vaccination (Table 3). On day 3 after administration, seroconversion rates were comparable between the ormutivimab and HRIG groups; however, the rate on day 7 was significantly higher in the ormutivimab than in the HRIG group (69.8% vs. 55.6%, P=0.0312). Both groups reached 100% seroconversion rates by days 14 and 42, respectively.
Time Ormutivimab (N=106) HRIG (N=108) P Seroconversion rates* Control for GMC Seroconversion rates* Control for GMC N (%) 95% CI GMC 95% CI N (%) 95% CI GMC 95% CI Positive† GMC Day 3 12 (11.32) 5.99, 18.94 0.29 0.27, 0.31 14 (12.96) 7.27, 20.79 0.32 0.30, 0.34 0.7131 0.0087 Day 7 74 (69.81) 60.13, 78.35 0.75 0.64, 0.88 60 (55.56) 45.68, 65.12 0.67 0.57, 0.78 0.0312 0.2540 Day 14 106 (100.00) 96.58, 100.00 61.05 50.36, 74.00 108 (100.00) 96.64, 100.00 24.07 19.92, 29.08 1.0000 <0.0001 Day 42 106 (100.00) 96.58, 100.00 42.62 36.22, 50.16 108 (100.00) 96.64, 100.00 21.70 18.49, 25.46 1.0000 <0.0001 Note: mFAS1 means a subset of FAS1, excluding subjects with pre-treatment neutralizing antibody levels ≥0.5 IU/mL.
Abbreviation: HRIG=human rabies immunoglobulin; GMC=geometric mean concentration; CI=confidence interval.
* represents the proportion of individuals with post-treatment RVNA levels ≥0.5 IU/mL among those with pre-treatment levels <0.5 IU/mL.
† represents the percentage of participants with RVNA levels ≥0.5 IU/mL.Table 3. Antibody seroconversion rates and GMC of rabies virus neutralizing antibody at each testing time point (mFAS1).
Among participants with baseline RVNA levels <0.5 IU/mL (mFAS1 population), the GMC of RVNA increased substantially over time in both treatment groups (Table 3, Figure 2). At day 3 post-administration, the GMCs in the ormutivimab group were significantly lower than those in the HRIG group (P=0.0087). At day 7, the GMC levels in both groups were not significantly different (P=0.2540). However, on days 14 and 42 post-administration, the GMC in the ormutivimab group was significantly higher than that in the HRIG group (P<0.0001).
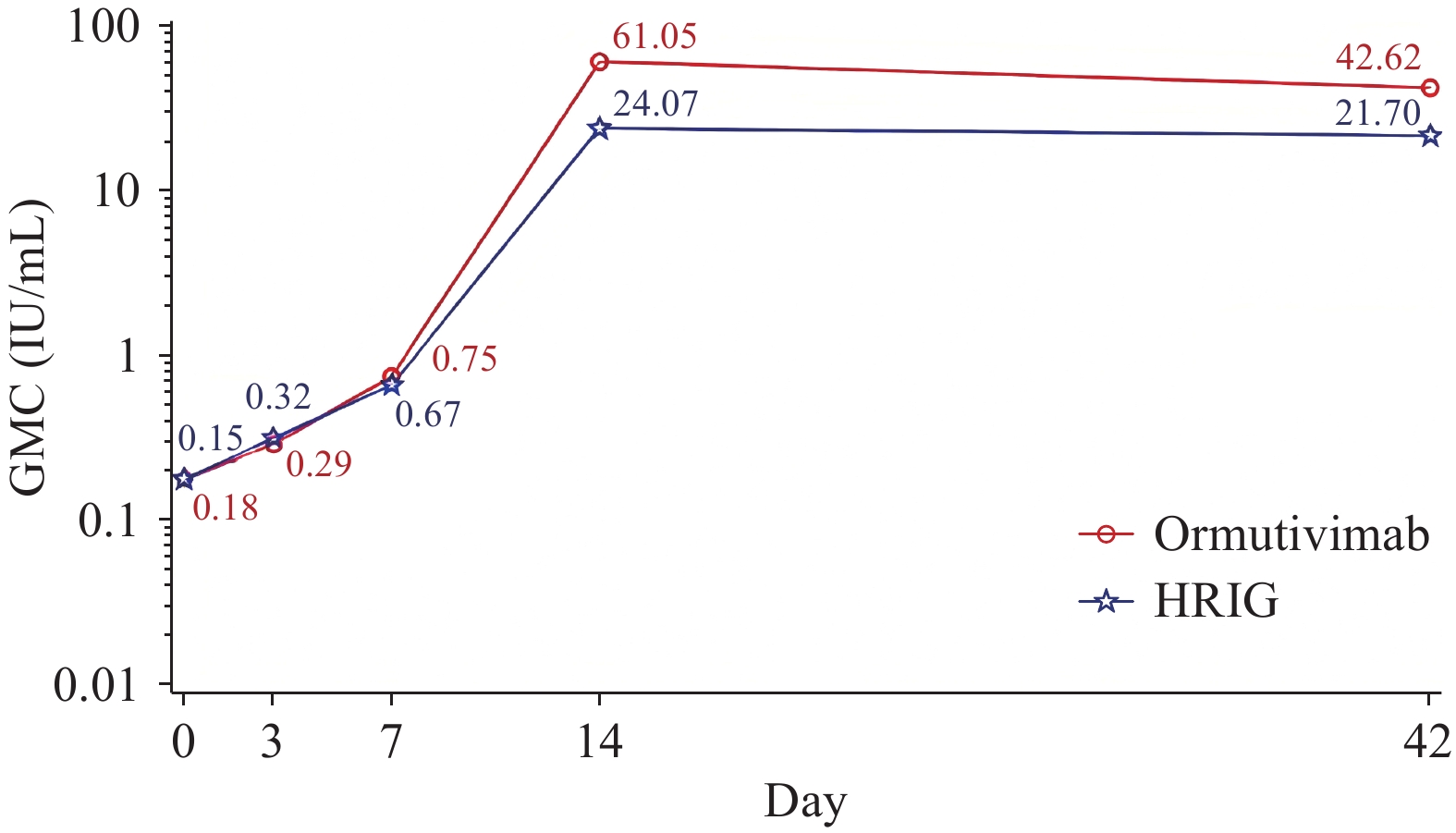 Figure 2.
Figure 2.Semi-logarithmic plot of rabies virus neutralizing antibody levels over time before and after immunization for each group (mFAS1).
Note: mFAS1 means a subset of the full dataset for antibody level analysis, excluding subjects with pre-treatment neutralizing antibody levels ≥0.5 IU/mL.
Abbreviation: HRIG=human rabies immunoglobulin; GMC=geometric mean concentrations.
All participants who completed the follow-up were alive 1 year after completion of the full rabies vaccination course.
In this randomized, double-blind, active-control phase III trial involving individuals aged <18 years with category III rabies exposure, ormutivimab demonstrated a favorable safety profile and immunogenicity comparable to that of HRIG when administered in combination with standard rabies vaccination. The incidence and severity of adverse events were comparable between groups, with most events being mild or moderate.
-
The positivity rate in the 12–17 years age group was lower than that in the 1–5 years and 6–11 years age groups at 7 days post-administration, suggesting slower initiation of active immunity in the 12–17 years age group, which could not promptly compensate for the decline in passive antibodies. Ormutivimab is metabolized through neonatal Fc Receptor (FcRn)-mediated circulation, and the FcRn expression in adolescents (12–17 years) is similar to that in adults (7–8). Although the initiation of active immunity in the 12–17 years age group was delayed compared with the 1–5 and 6–11 years age groups, it caught up by day 14, achieving a 100% positivity rate. On days 3 and 7 post-administration, no significant difference in antibody GMCs was observed between the ormutivimab and HRIG groups across different age groups. On days 14 and 42 post-administration, the GMC in the 1–5 years age group of the ormutivimab group showed a difference of more than 18 IU/mL compared with the 6–11 and 12–17 years age groups. This may be due to the younger age and lower body weight of the participants in the 1–5 years age group, which could amplify differences in the inhibitory effects of ormutivimab and HRIG on the vaccine, resulting in less inhibition with the trial drug. Additionally, the homogeneous Fc segment of anti-rabies monoclonal antibodies (human IgG1 subtype) can enhance active immunity through multiple mechanisms (9), and this enhancing effect is more pronounced in immunologically immature and highly plastic 1–5 year old children. No significant differences were observed between the control groups across different age groups, likely because HRIG provides only passive neutralizing antibodies and lacks immunomodulatory effects.
Here, participants receiving ormutivimab achieved higher seroconversion rates on day 7 than those receiving HRIG, and all participants in both groups reached seroprotective RVNA levels by day 14. Compared with the results of a phase III clinical trial of ormutivimab in individuals aged ≥18 years, a higher seroconversion rate was achieved in the sub-18 population within 7 days (10). Our findings suggest that ormutivimab provides timely passive immune support during the early post-exposure period when vaccine-induced immunity has not yet fully developed.
This study has several limitations. First, the rabies infection status of the biting animals could not be confirmed due to the logistical and safety challenges of capture and virological testing, preventing a direct assessment of protection against confirmed exposure. Second, only two participants aged <2 years were enrolled, limiting conclusions in very young children; therefore, ormutivimab is not recommended for children aged <2 years. Third, because no universally accepted method exists for detecting the local neutralization effect at the wound site, only RVNA levels were used as an indirect pharmacodynamic indicator. Finally, the RVNA titers were measured only up to day 42, preventing evaluation of immune persistence and limiting guidance on immunization strategies for re-exposure.
In conclusion, this phase III trial provides evidence supporting the immunogenicity and safety of ormutivimab as an alternative to HRIG for category III post-exposure prophylaxis in individuals aged <18 years. Anti-rabies mAbs are not restricted by raw material sources and can be produced stably, at scale, and sustainably, providing reliable passive immunization support in rabies-endemic regions. The development of anti-rabies mAbs enhances the standardization and coverage of PEP, facilitates the implementation of regional rabies elimination programs, contributes to the comprehensive and efficient operation of the national rabies prevention and control network, strengthens the emergency response and long-term prevention capabilities of the public health system, and supports the Global Strategic Plan to End Human Deaths from Dog-mediated Rabies by 2030 (Zero by 30).
HTML
| Citation: |

|