
 Download:
Download:




-
Introduction: In China, the total time from laboratory confirmation of human immunodeficiency virus (HIV) infection at the Center for Disease Control and Prevention to antiretroviral therapy (ART) initiation (T_total) comprises two intervals: the time from confirmed HIV diagnosis to the first hospital visit (T_PreHOS) and the time from the first hospital visit to ART initiation (T_PostHOS). However, the relative contributions of these intervals and their changes in the integrase strand transfer inhibitors (INSTI) era remain unclear.
Methods: This retrospective cohort study included adults with newly diagnosed HIV infection in Nanjing, China (2021–2024). Temporal trends in T_total, T_PreHOS, and T_PostHOS were assessed across calendar years. Factors associated with delays were examined using Cox proportional hazards model.
Results: Among the 1,456 patients analyzed, all three intervals showed substantial year-to-year reductions. The median T_total decreased from 20 to 9 days, driven by reductions in T_PreHOS (12 to 7 days) and T_PostHOS (7 to 0 days). In 2024, 37% initiated ART within 7 days of diagnosis, 49.8% attended the hospital within 7 days of HIV confirmation, and 87.9% initiated ART within 7 days of their first hospital visit. Notably, 56.3% started ART at their initial visit. Younger age was associated with delayed hospital attendance. INSTI-based regimens were independently associated with faster ART initiation.
Conclusion: Hospital-level delays have been largely eliminated in the INSTI era, making same-day ART initiation increasingly achievable. Further reductions in delay mandates targeted efforts to shorten T_PreHOS.
-
Rapid or same-day antiretroviral therapy (ART) initiation reduces viremia duration, disease progression, mortality, and human immunodeficiency virus (HIV) transmission (1). In China, patients are typically diagnosed at the Center for Disease Control and Prevention (CDC) and then referred to designated hospitals for ART; this diagnosis–referral–first-visit pathway may prolong time to ART initiation (2). New-generation integrase strand transfer inhibitors (INSTIs), with high resistance barriers and reduced reliance on baseline laboratory results, facilitate rapid ART after hospital presentation (3); however, real-world evidence on how the diagnosis-to-treatment interval (T_total) has changed in the INSTI era is limited. The relative contributions of the pre-hospital interval (from diagnosis to the first hospital visit; T_PreHOS) and post-hospital interval (from the first hospital visit to ART initiation; T_PostHOS) remain unclear. Although INSTIs were recommended by WHO in 2015 and China’s national guidelines in 2018 (4–5), uptake was constrained by cost until price reductions and reimbursement expansion in 2020 (6). We therefore define 2021–2024 as the “integrase strand transfer inhibitor (INSTI) era.”
To address this gap, we conducted a retrospective cohort study of adults (≥18 years) with HIV infection diagnosed between 2021 and 2024 and managed at the Second Hospital of Nanjing, which provides care for approximately 90% of persons with HIV in Nanjing (local CDC data), excluding those with severe AIDS-defining illnesses before ART initiation. In routine outpatient care, the only prerequisite for ART initiation was the absence of major abnormalities in routine blood tests and basic chemistry results, indicating intolerance to potential drug-related adverse events; and no regimen-specific or protocolized rapid-ART pathway was implemented. Temporal trends in T_total, T_PreHOS, and T_PostHOS were analyzed and their relative contributions to the overall delay were assessed. Group differences were compared using the Wilcoxon rank-sum test or the Chi-square test, as appropriate. Temporal trends were assessed using the Jonckheere–Terpstra trend test.
To identify factors associated with longer or shorter intervals, time-to-event analyses were conducted with T_PreHOS and T_PostHOS, treated as continuous outcomes without pre-specified delay thresholds. Kaplan–Meier methods and Cox proportional hazards models were used to evaluate the time to first hospital visit and time to ART initiation. For T_PreHOS, time zero was the date of laboratory-confirmed HIV diagnosis, and the event was the first hospital visit; for T_PostHOS, time zero was the first hospital visit, and the event was ART initiation. Participants were followed up until event occurrence or administratively censored at 30 days (T_PreHOS) or 14 days (T_PostHOS), whichever occurred first. All analyses were conducted using the R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria).
During 2021–2024, 1,818 adults newly initiated ART; after excluding 362, 1,456 were included, of whom 1,369 (94.0%) were male, with a median age of 30 years [interquartile range (IQR): 24.7–40.4]. Most infections occurred via homosexual transmission (1,056, 72.5%). At baseline, the median plasma HIV RNA level was 30,050 copies/mL (IQR: 6,500–83,800), and the median CD4 count was 351 cells/μL (IQR: 232–475). T_total had a median duration of 15 days (IQR: 9–27). In total, 230 patients (15.8%) initiated ART within 7 days after HIV confirmation and 1,120 (76.9%) started treatment within 30 days. The median T_PreHOS was 10 days (IQR: 5–19); 516 (35.4%) and 1,224 (84.1%) visited a designated hospital within 7 days and 30 days after HIV confirmation, respectively. T_PostHOS was shorter, with a median of 5 days (IQR: 0–7); 402 patients (27.6%) initiated ART on the same day as their first hospital visit, 937 (64.4%) within 7 days, and 1,402 (96.3%) within 30 days (Table 1).
Characteristics Total (N=1,456), n (%) Age, years 30 (24.7–40.4)* <30 730 (50.1) 30–44 446 (30.6) 45–59 174 (12.0) ≥60 106 (7.3) Men 1,369 (94.0) Marital status Unmarried 986 (67.7) Married or living with a partner 364 (25.0) Widowed, divorced, or unknown 106 (7.3) Routes of HIV transmission HET 386 (26.5) MSM 1,056 (72.5) IDU or unknown 14 (1.0) BMI, kg/m2 22.4 (20.3–24.5)* Occupation Employee outside the public-sector system 646 (44.4) Informal or flexible employment 434 (29.8) Public sector employee 197 (13.5) Student 179 (12.3) Educational attainment Junior college and above 946 (65.0) High school and secondary vocational school 201 (13.8) Junior high school and below 251 (17.2) Unknown 58 (4.0) VL, copies/mL 30,050
(6,500–83,800)*<10,000 434 (29.8) 10,000–50,000 494 (33.9) >50,000 528 (36.3) CD4, cells/μL 351 (232–475)* <350 721 (49.5) ≥350 735 (50.5) T_PreHOS, days 10 (5.0–19.0)* ≤7 516 (35.4) ≤30 1,224 (84.1) T_PostHOS, days 5 (0.0–7.0)* same-day 402 (27.6) ≤7 937 (64.4) ≤30 1,402 (96.3) T_total, days 15 (9.0–27.0)* ≤7 230 (15.8) ≤30 1,120 (76.9) Initial ART regimen NNRTI based 472 (32.4) INSTI-2DR 419 (28.8) INSTI-3DR 557 (38.3) Other 8 (0.5) Note: * Data are presented as median (interquartile range).
Abbreviation: ART=antiretroviral therapy; HET=heterosexual contact; MSM=men who have sex with men; IDU=intravenous drug use; BMI=body mass index; VL=viral load; CD4=CD4 count; NNRTI=non-nucleoside reverse transcriptase inhibitor; INSTI-2DR=integrase strand transfer inhibitor–based two-drug regimen; INSTI-3DR=integrase strand transfer inhibitor–based three-drug regimen; T_PreHOS=time from confirmed HIV diagnosis to the first hospital visit; T_PostHOS=time from the first hospital visit to ART initiation; T_total=time from confirmed HIV diagnosis to ART initiation (T_total=T_PreHOS+T_PostHOS).Table 1. Characteristics of the participants.
We then examined the temporal changes in these intervals across calendar years. Median T_total declined steadily from 20 days (IQR: 13–34) in 2021 to 18 (12–32) in 2022, 14 (7–26) in 2023, and 9 (5–18) in 2024. Median T_PreHOS is 12 days (IQR: 6–25) in 2021 and remain 12 (6–20) in 2022, followed by a decrease to 10 (5–19) in 2023 and 7 (4–13) in 2024. Median T_PostHOS decreased from 7 days (IQR: 4–8) in 2021 and 6 (3–8) in 2022 to 2 (0–6) in 2023 and 0 (0–3) in 2024 (Figure 1A–C).
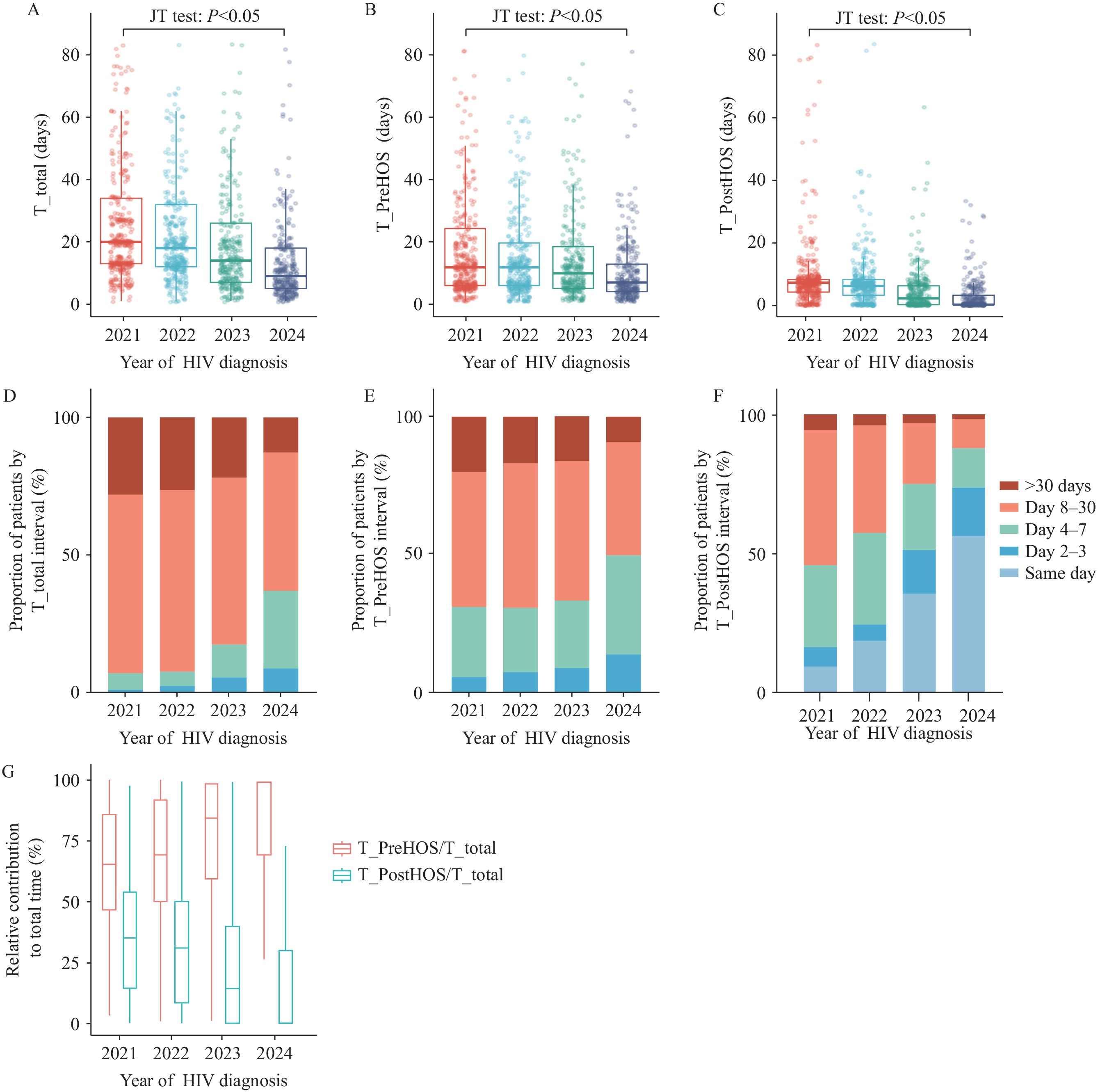 Figure 1.
Figure 1.Time intervals from HIV diagnosis to ART initiation: annual trends and distributions among adults in nanjing, 2021–2024. (A–C) Boxplots of T_total, T_PreHOS, and T_PostHOS by diagnosis year. (D–F) Proportions of patients in each interval category for T_total, T_PreHOS, and T_PostHOS. (G) Relative contributions of T_PreHOS and T_PostHOS to T_total.
Note: T_total = T_PreHOS+T_PostHOS.
Abbreviation: ART=antiretroviral therapy; T_PreHOS=time from confirmed HIV diagnosis to the first hospital visit; T_PostHOS=time from the first hospital visit to ART initiation; T_total=time from confirmed HIV diagnosis to ART initiation; JT=Jonckheere-Terpstra.
Correspondingly, ART initiation within 7 days of diagnosis increased from approximately 7.0% in 2021 to 37.0% in 2024, whereas initiation within 30 days increased from 71.9% to 87.1% (Figure 1D). For T_PreHOS, the proportion of patients attending a designated hospital within 7 days increased from 30.9% to 49.8% and within 30 days from 80.0% to 91.0% (Figure 1E). For T_PostHOS, same-day initiation increased from 9.3% to 56.3%, and initiation within 7 days of the first visit increased from 45.8% to 87.9% (Figure 1F).
To assess stage contributions, we compared absolute durations and proportional contributions (T_PreHOS/T_total and T_PostHOS/T_total). Across all years, median T_PreHOS consistently exceeded T_PostHOS (all P<0.05). Accordingly, median T_PreHOS/T_total ratio increased from 0.65 (IQR: 0.46–0.86) in 2021 and 0.69 (0.50–0.92) in 2022 to 0.86 (0.60–1.00) in 2023 and 1.00 (0.70–1.00) in 2024, consistently exceeding the corresponding T_PostHOS/T_total ratios of 0.35 (IQR: 0.14–0.54), 0.31 (IQR: 0.08–0.50), 0.14 (IQR: 0–0.40), and 0 (IQR: 0–0.30), respectively (all P<0.05; Figure 1G). These findings indicate that pre-hospital delays accounted for most of the diagnosis-to-treatment interval.
For T_PreHOS, Kaplan–Meier curves showed significant variations in hospital attendance within 30 days of diagnosis according to age and marital status (all P<0.05;
Supplementary Figure S1A–C ). In the multivariable Cox regression analysis, younger age (<30 years) was independently associated with a lower risk of hospital attendance (Supplementary Table S1 ).INSTI-based regimens were predominant (67.0%), followed by non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimens (32.4%). The proportion of patients receiving INSTI-based regimens increased from 52.6% in 2021 to approximately 73% in 2022 and remained stable thereafter, at approximately 75% at first hospital visit (Figure 2). For T_PostHOS, Kaplan–Meier analyses demonstrated differences in ART initiation speed across baseline CD4 strata and initial regimen types (all P<0.05;
Supplementary Figure S1D–I ). In the multivariable Cox model, baseline CD4 count and regimen remained significant: patients with CD4 ≥350 cells/μL had a lower hazard of ART initiation, whereas those receiving INSTI-based regimens had a higher hazard of ART initiation (Supplementary Table S2 ).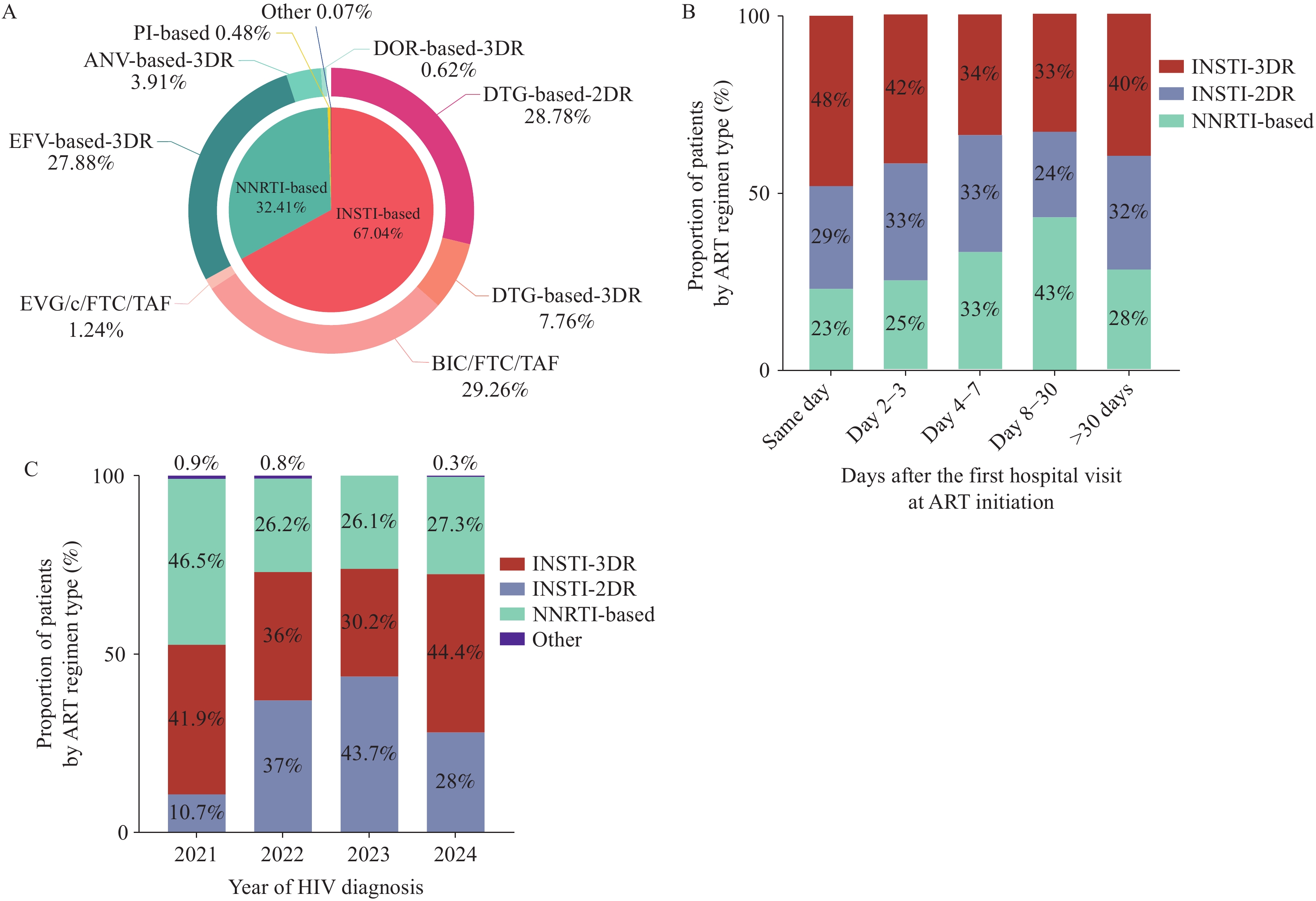 Figure 2.
Figure 2.Distribution and temporal patterns of initial ART regimens. (A) Overall distribution of initial ART regimens. (B) Distribution of initial ART regimens by time from first hospital visit to ART initiation. (C) Distribution of initial ART regimens by year of HIV diagnosis.
Abbreviation: ART=antiretroviral therapy; BIC=bictegravir; DOR=doravirine; DTG=dolutegravir; EFV=efavirenz; EVG/c=elvitegravir/cobicistat; FTC=emtricitabine; TAF=tenofovir alafenamide; 3TC=lamivudine; ANV=ainuovirine; INSTI=integrase strand transfer inhibitor; INSTI-2DR=INSTI-based two-drug regimen; INSTI-3DR=INSTI-based three-drug regimen; NNRTI=non-nucleoside reverse transcriptase inhibitor; PI=protease inhibitor. -
From 2021 to 2024, both T_PreHOS and T_PostHOS declined substantially, paralleling rapid ART implementation and expanded access to INSTI-based regimens after the 2021 insurance negotiations (6). Median T_PostHOS decreased from 7 days to 0 days, with over half of the patients initiating ART on the day of their first visit since 2022, indicating that it was no longer a major barrier. In contrast, despite improvement, T_PreHOS remained prolonged, with more than half of the patients in 2024 not accessing care within 7 days of diagnosis, making it the main limiting factor for further reductions in T_total.
T_PreHOS reflected a predominantly patient-dependent process. In multivariable analysis, younger age (<30 years) was independently associated with a longer T_PreHOS. Delayed hospital presentation among younger patients may reflect lower perceived urgency, fewer symptoms, and psychological factors, such as denial or stigma. Targeted post-diagnosis counseling, youth-focused education, and streamlined referral navigation may help reduce pre-hospital delays.
In contrast, T_PostHOS decreased substantially over time and contributed minimally to T_total. After adjustment, the INSTI-based regimens were the main regimen-level factors associated with faster ART initiation. Rather than reflecting a predefined rapid ART program, this association likely reflects evolving physician-driven practice patterns in a resource-rich setting, where early initiation is increasingly favored after safety assessment. INSTI-based regimens are therefore more frequently selected for earlier initiation because of perceived safety and flexibility, without implying a mandatory or exclusive role in accelerating treatment.
For patients in whom INSTI-based regimens were not selected, regardless of patient preference or other practical considerations, ART initiation was not subject to mandatory delays or required laboratory results. However, both clinicians and patients may have opted for a less urgent initiation timeline, allowing additional clinical information to guide treatment decisions. Additionally, patients with higher baseline CD4 counts experienced modest delays in ART initiation, possibly reflecting a lower perceived urgency for immediate treatment after clinical assessment. Importantly, this study does not assess rapid ART intervention, but describes organically accelerated ART initiation under preserved clinical discretion in a resource-rich environment.
This observed delay refines prior findings across different settings. National surveillance data from China show substantial reductions in the overall diagnosis-to-treatment interval, but aggregate pre- and post-hospital phases, obscuring phase-specific determinants (7). Building on the Guangxi “simplified test and treat” intervention, which identified service fragmentation as a key driver of delay and mortality, our analysis indicates that administrative separation between CDC confirmation and hospital-based treatment remains the principal contemporary bottleneck (8). Similar structural barriers have been reported in other systems, although with distinct system architectures; streamlined pathways in Hong Kong SAR, and rapid-entry programs in the United States have shortened diagnosis-to-ART intervals by reducing administrative complexity (9–10). Within China’s referral framework, integrated public health–clinical models could further shorten T_PreHOS including on-site joint CDC–hospital services enabling confirmatory testing, referral, and ART assessment within a single clinical unit, as well as electronic referral and shared data platforms allowing real-time appointment scheduling at diagnosis (8).
The findings in this report are subject to at least three limitations. First, this was a single-center study that primarily included clinically stable, outpatient adults initiating ART; therefore, the findings may not be generalizable to individuals with advanced disease or inpatient care pathways. Second, several unmeasured patient-level and system-related determinants could not be explicitly modeled, impeding quantification of their effects on T_PreHOS. Finally, the favorable local infrastructure may further limit direct generalizability to resource-limited settings, although, expanding access to generic INSTI-based regimens, may enable similar trends elsewhere.
In summary, in the INSTI era, China’s ART strategy has progressed, but T_PreHOS remains limiting; achieving same-day or 7-day ART initiation requires integrated public health and clinical services, institutions and patient engagement to reach national 95–95–95 targets.
-
Approved by the Ethics Committee of the Second Hospital of Nanjing (2024-LS-ky076). All the participants provided written informed consent.
HTML
| Citation: |

|