
 Download:
Download:




-
Introduction: Unintentional injuries are a leading cause of morbidity and mortality in young children. However, recent population-based epidemiological data on Chinese children are limited.
Methods: Data were obtained from a baseline survey of an ongoing cluster-randomized controlled trial completed between August 2024 and February 2025. Injury was defined as an event requiring medical care, first aid by a nonmedical responder, or more than half a day of school absence. Adjusted odds ratios quantified these associations.
Results: Among 7,087 children, 646 injuries occurred in the prior year, yielding an incidence of 9.12% [95% confidence interval (CI): 8.47, 9.81]. Compared with infants <1 year, children aged 1–2 and 3–5 years were at greater risk of injury. Boys and urban children had higher injury incidence rates than girls and rural children, and falls accounted for 69.2% of all cases. The injury events mainly occurred at home (57.9%) and during play (78.5%), resulting in emergency department or outpatient visits (40.1%) or self-care (54.6%). Commonly injured body parts included the head or neck (42.9%) and lower limbs (16.6%), with abrasions and open wounds being the most frequent outcomes.
Conclusion: Nonfatal injuries among young children remain a challenge in Changsha and require policy intention.
-
Unintentional injuries are the leading cause of death and disability in children worldwide. According to the Global Burden of Disease (GBD) 2023 estimates, they caused over 168,000 deaths and 15.9 million disability-adjusted life-years (DALYs) among children <5 years worldwide (1). In China, unintentional injuries accounted for 23% of all under-5 deaths in 2022 (2). Reliable, timely, and locally valid injury burden estimates are essential for targeting preventive strategies and allocating health resources. Currently, injury estimates in China rely largely on GBD studies or the hospital-based National Injury Surveillance System (NISS) (1-2). However, the GBD provides limited subnational details for local estimations. Meanwhile, the NISS, based on medically attended injuries from 310 hospitals across 109 counties or districts, merely provides injury case counts without population denominators. Furthermore, it does not capture injuries not treated in hospitals, missing about 40% of cases and underestimating the nonfatal injury burden (3). Population-based estimates with large samples of children <5 years are scarce in China. To our knowledge, the most recent study with a large sample estimating nonfatal injury morbidity was conducted in 2017 (4).
This study analyzed baseline data from an ongoing, cluster-randomized controlled trial evaluating a mobile health intervention to reduce unintentional injuries among children aged 0–5 years. The study design and sampling procedures are detailed in a previously published protocol (5). Briefly, a structured WeChat-based questionnaire was administered in Changsha, Hunan Province, China, from August 2024 to February 2025. Using urban–rural stratified sampling, eight urban streets and four rural towns were selected based on prespecified eligibility. Primary caregivers of children aged ≤5 years were recruited from these 12 clusters with the assistance of local healthcare institutions and kindergartens. Data were collected from the youngest child in each household if the family had two or more eligible children. A total of 7,097 caregivers submitted the questionnaire. After excluding 10 duplicate and incomplete records, 7,087 participants remained. This sample provided sufficient precision for estimating population-level injury incidence, with the anticipated 95% confidence interval half-width constrained to approximately ±1.0 percentage points based on prior evidence (6).
The structured questionnaire gathered data on 1) caregiver and child sociodemographic characteristics and 2) the child’s unintentional injury history in the past 12 months, including injury type, location, activity at the time of injury, post-injury care, injured body region, and nature of the injury. An injury event was defined (7) as any event meeting the following: 1) diagnosis and treatment at a healthcare facility; 2) first aid provided by a nonmedical responder; or 3) absence from school for more than half a day due to injury.
The primary outcome was the 12-month injury incidence rate, defined as the number of injury events in the past 12 months divided by the total number of children. Descriptive statistics and bar charts were used to summarize participant characteristics and subgroup patterns. The 95% confidence intervals (CI) were calculated using the Wilson score method. Statistical significance was assessed using the Pearson chi-square test for categorical comparisons. The adjusted odds ratios (aORs) were estimated using a multilevel mixed-effects logistic regression with a random intercept for the study site to account for clustering. Covariates were selected based on a literature review. All tests were two-sided (α=0.05). Subgroup analyses were conducted based on age and sex. All analyses were performed using SAS (version 9.4, SAS Institute, Cary, NC, USA).
Of the 7,087 children, 64.0% were aged 3–5 years, 53.2% were boys, and 59.2% resided in urban areas (Table 1). A total of 646 unintentional injuries were reported within the past 12 months, corresponding to an incidence rate of 9.12% (95% CI: 8.47, 9.81). The crude injury incidence was higher in urban areas (9.99%; 95% CI: 9.11, 10.93) than in rural areas (7.85%; 95% CI: 6.93, 8.89). After using the combined study population as the standard, the age-standardized incidence was 9.94% in urban areas and 8.45% in rural areas. After controlling for covariates, boys, children living in urban areas, and older children (1–2 years and 3–5 years) had higher incidence rates than girls (aOR=1.67; 95% CI: 1.41, 1.98), those residing in rural areas (aOR=1.24; 95% CI: 1.01, 1.52), and those <1 year (aOR=2.15; 95% CI: 1.54, 2.99 and aOR=2.13; 95% CI: 1.58, 2.89) (Table 1). Subgroup analyses stratified by age and sex yielded results consistent with those of the main analysis (
Supplementary Tables S1 and S2 ).Variable Number (%) Incidence (%) (95% CI) Adjusted OR (95% CI) Total 7,087 (100.0) 9.12 (8.47, 9.81) Place Rural 2,891 (40.8) 7.85 (6.93, 8.89) Ref Urban 4,196 (59.2) 9.99 (9.11, 10.93) 1.24 (1.01, 1.52)* Child age (years) <1 1,113 (15.7) 4.76 (3.66, 6.18) Ref 1–2 1,440 (20.3) 9.58 (8.17, 11.21) 2.15 (1.54, 2.99)* 3–5 4,534 (64.0) 10.04 (9.19, 10.94) 2.13 (1.58, 2.89)* Child sex Female 3,317 (46.8) 6.96 (6.15, 7.88) Ref Male 3,770 (53.2) 11.01 (10.05, 12.05) 1.67 (1.41, 1.98)* Caregivers’ characteristics Age group (years) <30 1,555 (21.9) 8.68 (7.38, 10.18) Ref 30–39 4,571 (64.5) 9.34 (8.53, 10.22) 0.95 (0.77, 1.17) ≥40 961 (13.6) 8.74 (7.12, 10.69) 0.89 (0.66, 1.20) Sex Female 5,695 (80.4) 9.11 (8.39, 9.89) Ref Male 1,392 (19.6) 9.12 (7.72, 10.75) 0.97 (0.78, 1.19) Level of education Middle school or lower 1,243 (17.5) 8.85 (7.39, 10.56) Ref High school or equivalent 1,603 (22.6) 8.05 (6.81, 9.48) 0.83 (0.62, 1.09) College or higher 4,241 (59.8) 9.60 (8.75, 10.52) 0.94 (0.73, 1.22) Annual household income (CNY) <20,000 1,187 (16.7) 8.76 (7.28, 10.51) Ref 20,000–49,999 1,463 (20.6) 8.13 (6.84, 9.65) 0.89 (0.67, 1.18) 50,000–99,999 2,134 (30.1) 9.56 (8.38, 10.88) 1.01 (0.78, 1.31) ≥100,000 2,303 (32.5) 9.51 (8.38, 10.78) 0.95 (0.72, 1.23) Note: Multilevel logistic regression included the following covariates: location (urban or rural), child age, child sex, caregivers’ characteristics (including age group, sex, level of education, and annual household income), and study sites (streets or towns) as a random intercept to control for clustering effects.
Abbreviation: OR=odds ratio; CI=confidence interval; CNY=Chinese Yuan.
* P<0.05.Table 1. Unintentional injury incidence among children aged 0–5 years — Changsha City, Hunan Province, China, 2024–2025.
As shown in Figure 1A, falls were the most common cause of injury (69.2%), particularly among infants <1 year (75.5%) and children 1–2 years (76.1%). Children’s homes were the primary injury settings (57.9%), especially for children aged 1–2 years (70.3%) and in rural areas (71.8%) (Figure 1B). Most injuries took place during play (78.5%) (Figure 1C). Post-injury care was commonly self-care or first aid (54.6%), followed by care in emergency departments or outpatient clinics (40.1%) (Figure 1D).
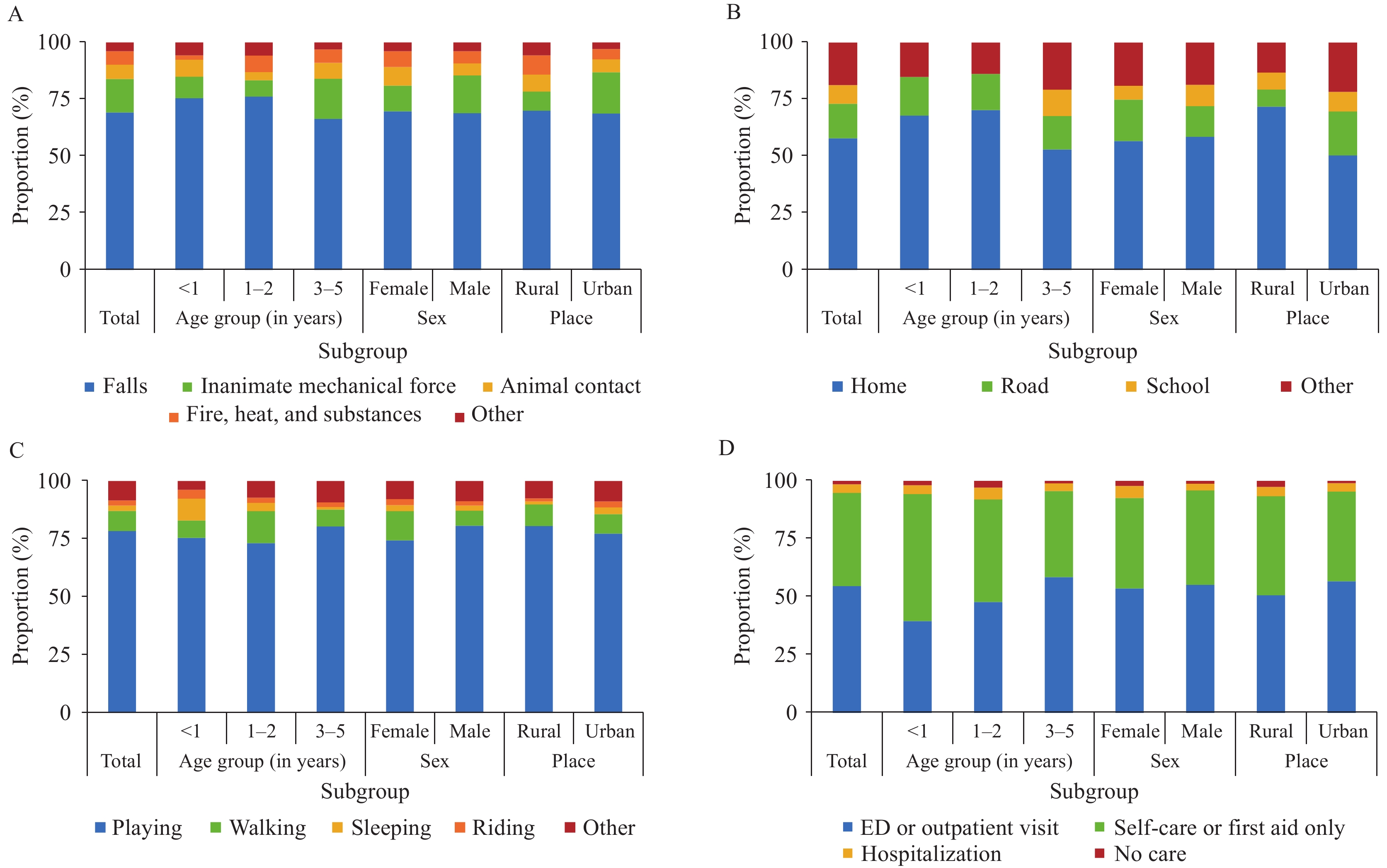 Figure 1.
Figure 1.Distribution of external cause, location, activity, and treatment of unintentional injuries in children aged 0–5 years in Changsha City, Hunan Province, China, 2024–2025. (A) Injury type; (B) Injury location; (C) Activity at injury; (D) Post-injury care.
Note: In Figure 1A, total traffic-related injuries accounted for only 1.5% of events and were merged into the “Other” category. Abbreviation: ED=emergency department.Head or neck, lower limbs, and hands or feet were the most frequently injured body regions, at 42.9%, 16.6%, and 14.4%, respectively. By nature, abrasions (42.4%) and open wounds (25.7%) were the most common outcomes of injuries (Figure 2).
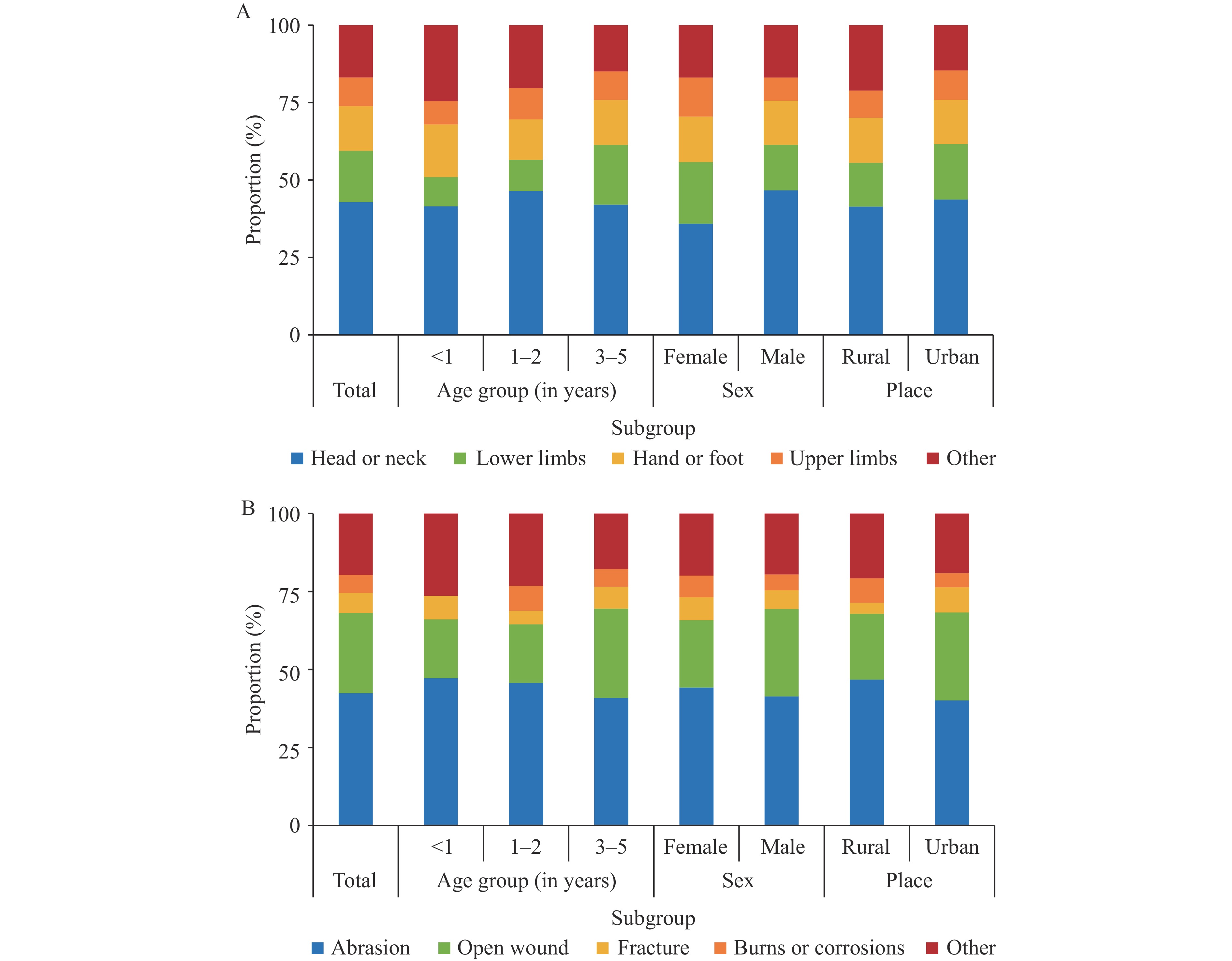 Figure 2.
Figure 2.Distribution of body part and nature of unintentional injuries in children aged 0–5 years in Changsha City, Hunan Province, China, 2024–2025. (A) Injured body region; (B) Nature of injury.
-
The incidence of unintentional injury in early childhood varies according to sex, age group, and urban–rural residence. Falls were the predominant injury type, with most injuries occurring at home during play and typically managed with self-care or first aid.
Although this survey estimate of injury incidence (9.12%) was numerically lower than the GBD 2023 national estimate for Chinese children <5 years (11.7%), these data are not directly comparable. The GBD provides a nationally aggregated, model-based estimate derived from multiple data sources (mortality, inpatient, and outpatient data) and may reflect a different case mix and severity spectrum compared to this community survey in Changsha. The survey estimate was also lower than the 34% reported in the 2017 Changsha study, which used a similar injury definition but sampled only urban areas and included children aged 0–6 years (8). Recent improvements in child injury prevention over the past several years may have contributed to this decline. By contrast, the survey estimate exceeded that of the 2017 multi-province survey (3.0% for non-school-aged children and 5.0% for preschool children), although both studies relied mainly on caregiver reports and the multi-province survey additionally incorporated kindergarten teacher reports (4). These differences are likely driven by variations in the sampling frames, case definitions, and estimation methods. Overall, our findings provide an up-to-date, locally generated estimate for Changsha and highlight the need to standardize community-based injury measurements in China.
Age- and sex-specific patterns were consistent with those reported in previous studies (9–10). However, the observed urban-rural difference — a higher incidence in urban areas than in rural areas — contrasts with earlier findings that typically reported a heavier burden in rural settings (2–3,10). Four factors may help explain this observation. First, urban families often rely on grandparents or other informal childcare facilities, which may be associated with a higher risk of injury. Second, urban caregivers may have greater access to health information and injury-related knowledge, which may increase their injury recognition and reporting. Conversely, grandparents living in rural areas may have underreported minor events. Therefore, the observed urban–rural differences may partly reflect differential ascertainment and differences in injury event reporting. Third, rapid urbanization in Changsha’s high-rise housing, more indoor play in confined spaces, and increasing private vehicle ownership may have shifted children’s exposure profiles toward urban, home, and traffic-related risks. Fourth, differences in the types (or spectra) of injuries contribute to the disparity in the incidence of urban–rural injuries.
Falls were the predominant injury mechanism (69.2%), which differs from that reported by the 2018 NISS for both urban and rural children (55.3% and 60.2%, respectively) (9). This is consistent with earlier community-based studies in Hunan and multi-province surveys, which found that household interviews captured many mild, nonmedically attended fall events that were missed during hospital surveillance (3–4). As shown in this study, more than half of injury events were managed at home. Separately, the national mortality surveillance reports a different leading cause profile for fatal injuries (e.g., suffocation, drowning, and road traffic injuries) (10). Given the fundamental differences in outcome severity, these findings should not be directly compared; rather, they suggest that prevention priorities may differ between fatal and nonfatal injuries. These findings highlight falls in and around the home as a priority target for caregiver education, safe home modifications, and the integration of injury prevention content into routine child health services. Consistent with the Child Fall Intervention Technical Guidelines published by the Chinese Center for Disease Control and Prevention in 2011, relevant local authorities could consider providing home safety devices (e.g., window restrictors, anti-slip mats, and corner guards) to families with children aged 0–2 years, distributed through routine community immunization visits at one, six, and 18 months.
This study has several limitations. First, injury information was collected from caregivers using a 12-month recall window; minor, quickly resolved, or non-care-seeking injuries were likely to be forgotten. Second, this survey did not cover additional behavioral or environmental factors, nor did it include conditions such as attention-deficit/hyperactivity disorder (ADHD) that may increase the risk of injury. Third, the data were collected from Changsha using a WeChat-based questionnaire, which may limit generalizability to other regions or households with limited digital access. Additionally, the WeChat recruitment process via mobile phones may overrepresent younger parents and exclude older caregivers (e.g., grandparents), introducing a potential sample selection bias. As the data were collected via caregiver self-reports, recall bias may have existed. Because this study did not analyze fatal injury data, the results may differ from child unintentional injury mortality data.
This large community-based baseline survey provides updated, locally relevant estimates of nonfatal unintentional injuries among children <5 years of age in Changsha. Unintentional injuries remain common, with falls being the leading cause. Unlike earlier studies showing a higher burden in rural areas, this survey reported a higher incidence in urban settings, suggesting changing exposure patterns and the influence of caregiver arrangements. These findings demonstrate the importance of community-based reporting in capturing injuries that were not captured during hospital surveillance. Prevention efforts should focus on falls, home and play safety, and reducing urban-specific risks.
-
All participating primary healthcare institutions and kindergartens, as well as local government officials, for their support in facilitating this project.
-
Approved by the Ethics Committee of the Xiangya School of Public Health, Central South University (XYGW-2024-71).
HTML
| Citation: |

|