
 Download:
Download:




-
Introduction: Intraocular pressure (IOP) is essential for ocular homeostasis and pediatric glaucoma prevention. However, its developmental patterns and associations with refractive error remain unclear. This study examined grade- and sex-specific IOP variations and their relationship with ocular biometrics in a large pediatric cohort.
Methods: This nationwide cross-sectional study included 65,209 students (grades 0–12) from 10 provincial-level administrative divisions (PLADs) in China between 2020 and 2024. IOP was measured using non-contact tonometry. Cycloplegic refraction and ocular biometry — including axial length, corneal radius, and anterior chamber depth — were also assessed. Multivariable linear regression assessed associations between IOP and ocular parameters, adjusting for grade and sex.
Results: Mean IOP was 17.6±3.0 mmHg, showing a biphasic pattern, peaking at grade 6 (18.2±2.9 mmHg) and declining thereafter. Girls had significantly higher IOP prepuberty [peak difference at grade 5: 0.5 mmHg; 95% confidence interval (CI): 0.3, 0.7], whereas boys exhibited higher IOP post-puberty (grade 12: −0.5 mmHg; 95% CI: –0.9, –0.1). IOP was higher in children with myopia (P<0.01) and was significantly associated with spherical equivalent (β=−0.04, P=0.01), corneal radius (β=2.03, P=0.04), and anterior chamber depth (β=0.42, P<0.01).
Conclusion: This study identified distinct grade- and sex-specific IOP patterns among Chinese children, including a novel pubertal reversal in sexual dimorphism. The findings challenge a simple causal IOP−myopia relationship and warrant further investigation. These results support the need for tailored pediatric IOP monitoring strategies to improve glaucoma prevention, enhance myopia control, and promote overall ocular health.
-
Intraocular pressure (IOP), which is essential for ocular homeostasis, remains insufficiently studied in pediatric populations. IOP plays a pivotal role in the diagnosis and management of glaucoma, a leading cause of irreversible blindness worldwide, including among children (1). Early detection and screening are critical for preventing vision loss in pediatric glaucoma (1). Delayed diagnosis can impose substantial emotional and psychological burdens on both patients and their caregivers (1). Accurate assessment of IOP in children is therefore crucial for the timely detection of ocular hypertension and the prevention of childhood glaucoma, particularly given the absence of a universally accepted threshold for ocular hypertension in this age group (2).
Previous studies suggest that elevated IOP may induce scleral stress and creep, potentially contributing to axial elongation and myopia progression (3). However, current evidence regarding the association between IOP and myopia remains inconsistent (4–5). This inconsistency underscores the need for a more nuanced understanding of IOP’s role, which may vary according to refractive status and other ocular biometric parameters. Orthokeratology and low-concentration atropine eye drops — widely used strategies for myopia control — have been shown to modulate choroidal thickness and blood flow, suggesting a biomechanical pathway that may indirectly involve IOP (6).
Continuous IOP monitoring, alongside ocular biometric parameters such as axial length, may provide valuable insights for early detection and targeted interventions (7). However, most existing studies on IOP and ocular biometrics have focused on adults or relatively small, region-specific pediatric samples. To address this gap, the present study — conducted across 10 provincial-level administrative divisions (PLADs) in China — aimed to characterize grade- and sex-specific variations in IOP among school-aged children and to examine their associations with refractive error and ocular biometric parameters.
Between 2020 and 2024, the National Disease Control and Prevention Administration of China conducted a nationwide survey of hyperopia reserve across 10 PLADs: Beijing, Liaoning, Zhejiang, Shandong, and Guangdong (eastern China); Henan, Hunan, and Shanxi (central China); and Chongqing and Shaanxi (western China). The minimum sample size for each grade was estimated using the simple random sampling formula based on data from the 2020 national myopia survey. In most PLADs, two cities were selected according to economic development level (one more developed and one less developed). Within each PLAD, 15–20 kindergartens, 15–20 primary schools, 8–10 junior high schools, and 8–10 senior high schools were selected, maintaining a 1∶1 urban-to-rural ratio for each school type. Classes were then randomly selected within each school, and all students in the selected classes were invited to participate with informed consent. Using a multistage cluster sampling design, a total of 67,260 students from senior kindergartens (Grade 0) through third-year high school (Grade 12) were selected.
IOP was measured using a non-contact tonometer (Topcon CT-800A; Topcon Co., Tokyo, Japan). Cycloplegic refraction was performed following 0.5% tropicamide administration (four instillations at 5-minute intervals). Spherical equivalent (SE) was measured using an autorefractor (KR-800; Topcon Co., Tokyo, Japan). Cycloplegia and pupil dilation were assessed after an additional 30 minutes; full cycloplegia was defined as a pupil diameter ≥6 mm with the absence of the light reflex. Ocular biometric parameters, including axial length (AL), corneal radius (CR), and anterior chamber depth (ACD), were measured using the IOLMaster 500 (Carl Zeiss Meditec AG, Jena, Germany). Three consecutive measurements were obtained for each eye, and mean values were used for analysis.
All examinations were conducted by certified professionals to ensure measurement accuracy. Quality control included same-day random retesting of 5% of participants at each survey site. If the difference between repeated measurements was <5.0 mmHg for IOP, <0.50 diopters (D) for SE, <0.05 mm for AL, <0.50 D for CR, and <0.20 mm for ACD, the initial measurement was retained. If the difference exceeded these thresholds, corrective actions (e.g., optimizing the measurement environment or recalibrating instruments) were implemented, and measurements were repeated until criteria were met. If more than 5% of retested participants at a site exceeded these thresholds, all measurements from that day were considered invalid, and the survey was repeated. SE was calculated as spherical power plus half of the cylindrical power. Refractive status was classified as myopia (SE≤–0.50 D), emmetropia (–0.50 D<SE<+0.50 D), and hyperopia (SE≥+0.50 D). To ensure statistical independence, only right-eye measurements were included in the final analysis due to high interocular correlation.
Continuous variables are presented as means ± standard deviations (SDs), and categorical variables are presented as frequencies and percentages. Between-group comparisons were conducted using t-tests or one-way analysis of variance for continuous variables and chi-square tests for categorical variables, as appropriate. Univariable and multivariable linear regression analyses were performed to assess associations between IOP and ocular parameters. All tests were two-tailed, and P<0.05 was considered statistically significant. Analyses were conducted using R software (version 4.5.2; R Foundation for Statistical Computing, Vienna, Austria).
A total of 65,209 of 67,260 students (97.0%) were included in the analyses (
Supplementary Figure S1 ). Of these, 33,652 (51.6%) were boys. The sample comprised 15,071 (23.1%) senior kindergarten students, 42,871 (65.7%) elementary school students, 4,247 (6.5%) middle school students, and 3,020 (4.6%) high school students.IOP varied significantly across grade levels, with a mean±SD of 17.6±3.0 mmHg. From senior kindergarten (grade 0) through elementary school (grades 1–6), IOP increased progressively [17.0±2.9 mmHg in grade 0 vs. 18.2±2.9 mmHg in grade 6]. Thereafter, IOP declined gradually during secondary education (grades 7–12), reaching 17.3±3.0 mmHg in grade 12, with a slight rebound in grade 9. This biphasic pattern was observed in both sexes (Figure 1). Sex-specific differences in IOP were evident across developmental stages. Girls had significantly higher IOP than boys from grades 0–7, with the largest difference in grade 5 (mean difference, 0.5 mmHg; 95% CI: 0.3, 0.7). Although girls continued to exhibit slightly higher IOP in grades 8–9, these differences were not statistically significant. A reversal of the sex pattern occurred in later grades, with boys demonstrating higher IOP from grade 10 onward; this difference reached statistical significance in grade 12 (mean difference, −0.5 mmHg; 95% CI: −0.9, −0.1) (Table 1, Figure 2).
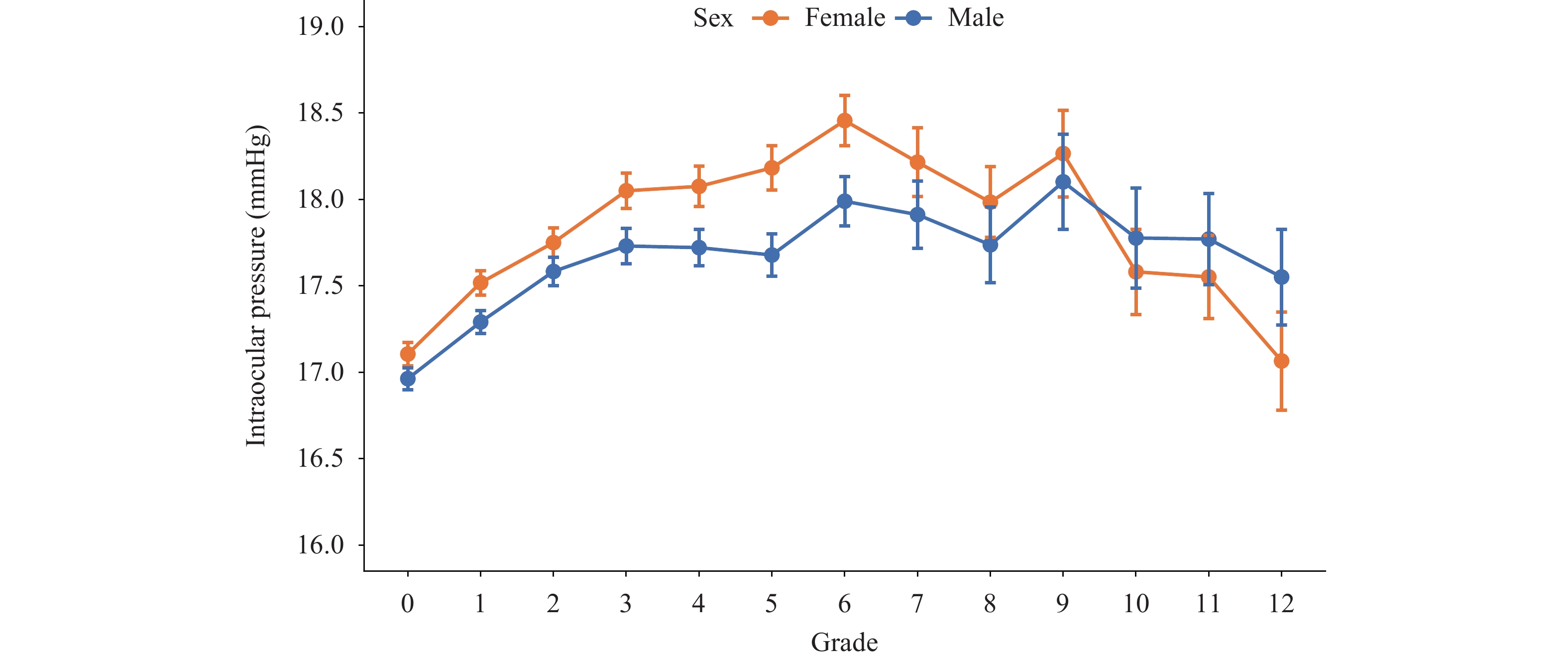 Figure 1.
Figure 1.Sex-stratified trends in mean intraocular pressure by grade level among children and adolescents across 10 provincial-level administrative divisions in China, 2020–2024.
Grade Intraocular pressure (Mean±SD) Mean difference (95% CI) P Female Male 0* 17.1±2.9 17.0±2.9 0.1 (0.0, 0.2) <0.01 1 17.5±3.0 17.3±2.9 0.2 (0.1, 0.3) <0.01 2 17.8±2.9 17.6±3.0 0.2 (0.0, 0.3) 0.01 3 18.1±3.1 17.7±3.1 0.3 (0.2, 0.5) <0.01 4 18.1±2.9 17.7±2.8 0.4 (0.2, 0.5) <0.01 5 18.2±3.0 17.7±3.0 0.5 (0.3, 0.7) <0.01 6 18.5±2.9 18.0±3.0 0.5 (0.3, 0.7) <0.01 7 18.2±3.0 17.9±3.0 0.3 (0.0, 0.6) 0.03 8 18.0±3.0 17.7±3.0 0.2 (–0.1, 0.5) 0.11 9 18.3±2.8 18.1±3.0 0.2 (–0.2, 0.5) 0.39 10 17.6±2.9 17.8±3.2 –0.2 (–0.6, 0.2) 0.31 11 17.6±2.9 17.8±3.1 –0.2 (–0.6, 0.1) 0.23 12 17.1±2.8 17.6±3.2 –0.5 (–0.9, –0.1) 0.02 Abbreviations: CI=confidence interval; SD=standard deviation.
* Grade 0 means senior kindergarten.Table 1. Sex differences in intraocular pressure across grade levels among children and adolescents across 10 provincial-level administrative divisions in China, 2020–2024.
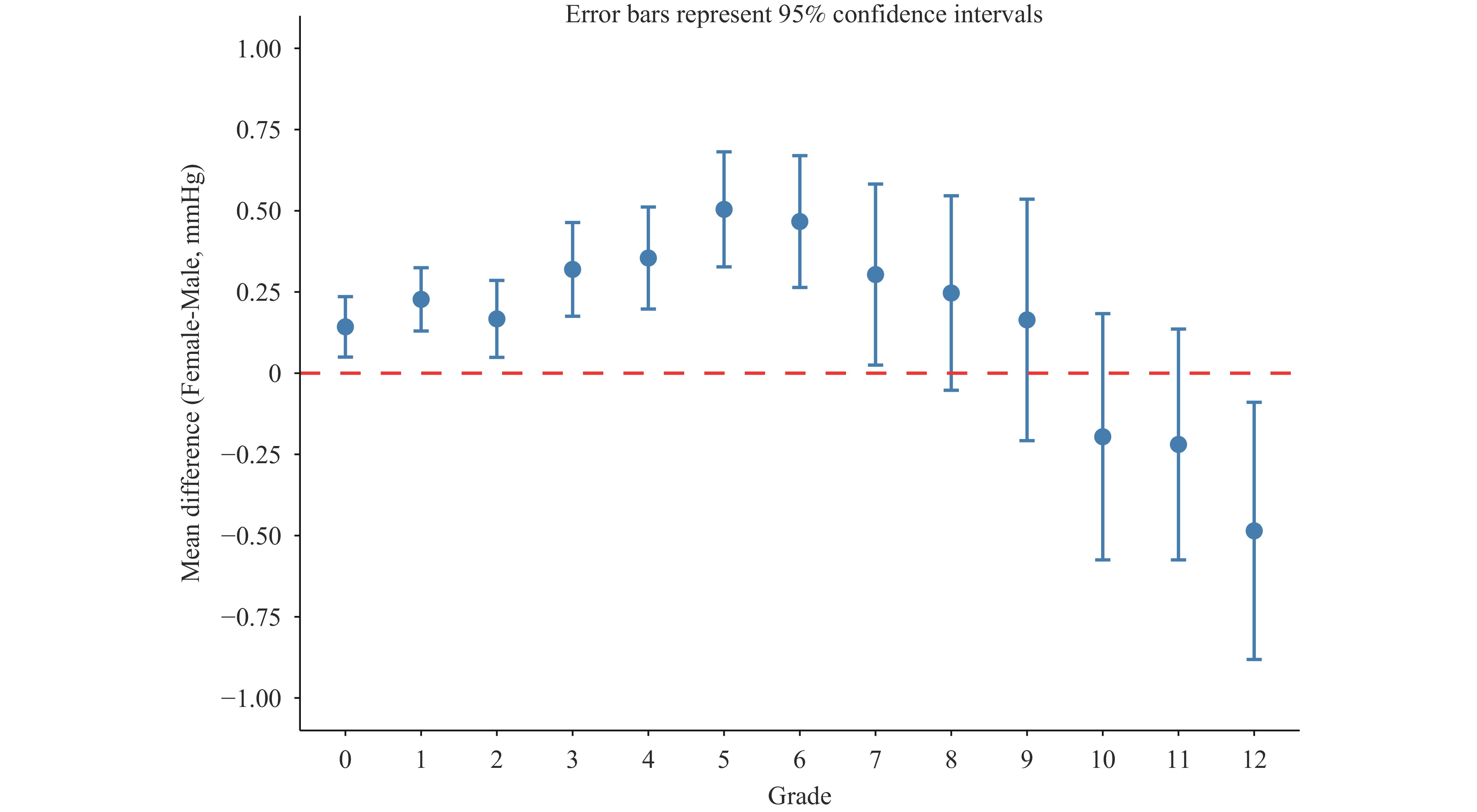 Figure 2.
Figure 2.Sex differences in intraocular pressure across grade levels among children and adolescents across 10 provincial-level administrative divisions in China, 2020–2024.
Overall, IOP differed significantly across refractive status groups (P<0.01). Myopic participants had the highest mean±SD IOP [17.9±2.9 mmHg], followed by emmetropic participants [17.7±2.9 mmHg] and hyperopic participants [17.4±3.0 mmHg]. Grade-stratified analyses revealed distinct developmental patterns (Table 2). In senior kindergarten (grade 0), emmetropic children had significantly higher IOP than hyperopic children (P=0.02). Among elementary school students (grades 1–6), a gradient was observed (myopia > emmetropia > hyperopia; all pairwise comparisons P<0.05). This association was not significant in lower secondary school (grades 7–9; all pairwise comparisons P>0.05) but reversed in upper secondary school (grades 10–12), where emmetropic students had significantly lower IOP than hyperopic students (P=0.02).
Educational Stages Refractive Status Mean difference (95% CI) P Kindergarten Emmetropia vs. Myopia 0 (–0.31, 0.30) 1.00 Kindergarten Hyperopia vs. Myopia –0.19 (–0.46, 0.08) 0.24 Kindergarten Hyperopia vs. Emmetropia –0.18 (–0.34, –0.03) 0.02* Elementary school Emmetropia vs. Myopia –0.10 (–0.20, –0.01) 0.03* Elementary school Hyperopia vs. Myopia –0.41 (–0.49, –0.33) <0.01* Elementary school Hyperopia vs. Emmetropia –0.30 (–0.39, –0.22) <0.01* Lower secondary school Emmetropia vs. Myopia –0.23 (–0.54, 0.09) 0.21 Lower secondary school Hyperopia vs. Myopia –0.14 (–0.53, 0.25) 0.68 Lower secondary school Hyperopia vs. Emmetropia 0.09 (–0.39, 0.56) 0.90 Higher secondary school Emmetropia vs. Myopia –0.27 (–0.69, 0.15) 0.30 Higher secondary school Hyperopia vs. Myopia 0.42 (–0.07, 0.90) 0.11 Higher secondary school Hyperopia vs. Emmetropia 0.68 (0.07, 1.29) 0.02* Abbreviation: CI=confidence interval.
Note: * P<0.05.Table 2. Differences in intraocular pressure across refractive status among children and adolescents across 10 provincial-level administrative divisions in China, 2020–2024, stratified by educational stage.
In univariable analyses, IOP was associated with several ocular biometric parameters, showing a negative correlation with SE and positive correlations with AL, CR, the AL/CR ratio, and ACD (all P<0.01). In multivariable models adjusted for grade, sex, and ocular parameters, IOP remained significantly associated with SE (β=−0.04; 95% CI: −0.06, −0.01; P=0.01), CR (β=2.03; 95% CI: 0.09, 3.96; P=0.04), and ACD (β=0.42; 95% CI: 0.34, 0.50; P<0.01). Associations with AL and the AL/CR ratio were not statistically significant (Table 3).
Variables Univariable analysis Multivariable analysis* β (95% CI) P β (95% CI) P SE –0.12 (–0.14, –0.11) <0.01 –0.04 (–0.06, –0.01) 0.01 AL 0.21 (0.19, 0.23) <0.01 –0.59 (–1.24, 0.06) 0.08 CR 0.18 (0.09, 0.27) <0.01 2.03 (0.09, 3.96) 0.04 AL/CR 1.63 (1.44, 1.81) <0.01 4.81 (–0.24, 9.86) 0.06 ACD 0.67 (0.60, 0.74) <0.01 0.42 (0.34, 0.50) <0.01 Note: β=regression coefficient reflecting the linear relationship between variables.
Abbreviation: SE=spherical equivalent; AL=axial length; CR=corneal radius; AL/CR=axial length to corneal radius ratio; ACD=anterior chamber depth; CI=confidence interval.
* The multivariable analysis was adjusted for ocular parameters (SE, AL, CR, AL/CR, and ACD), grade, and sex.Table 3. Associations between intraocular pressure (mmHg) and ocular parameters among children and adolescents across 10 provincial-level administrative divisions in China, 2020–2024.
-
This large-scale, population-based study provides comprehensive evidence of grade- and sex-related variations in IOP among Chinese school-aged children and adolescents and elucidates its complex associations with refractive status and ocular biometric parameters. These findings enhance understanding of IOP dynamics during ocular development in childhood.
IOP followed a biphasic developmental pattern: it increased to a peak in grade 6 (approximately 12 years of age), declined gradually through secondary education, and exhibited a transient elevation in grade 9 (approximately 15 years of age). This pattern partly aligns with previous studies in Chinese populations. The Shandong Study reported IOP peaks at ages 10 and 15 years (8), whereas the Mojiang Study identified peaks at ages 9 and 15 years (9). Notably, the present study’s IOP measurements aligned closely with those from the Shandong cohort but were consistently higher than those reported in the Mojiang Study across all age groups. These discrepancies may reflect differences in population characteristics (e.g., ethnic composition), geographic factors (particularly Mojiang’s high-altitude location), or measurement methodologies.
A novel finding is the grade-dependent reversal of the sex differences in IOP. Females exhibited higher IOP prepuberty (grades 0–7), whereas males showed higher IOP post-puberty. This transitional pattern has not been previously reported and contrasts with existing literature describing consistent sex-specific differences, with IOP persistently higher in either females (4,8–9) or males (10). This observed reversal may reflect hormonal influences on ocular hydrodynamics during development and warrants further investigation in prospective cohort studies.
The association between IOP and refractive status was complex and developmentally modulated. Although myopic participants had higher overall IOP, stratified analyses indicated that this relationship was not consistent across grade groups. The absence of a uniform gradient (myopia > emmetropia > hyperopia) suggests that the role of IOP in refractive development may be context-dependent, potentially mediated by other growth-related factors or restricted to specific developmental windows.
The findings in this report are subject to at least two limitations. First, its cross-sectional design precludes causal inferences. Second, although non-contact tonometry was used for its practicality in pediatric populations (e.g., efficiency and reduced infection risk), the absence of Goldmann applanation tonometry and central corneal thickness measurements may have introduced measurement bias (11).
This study also has notable strengths. Because it was conducted in schools on a grade-by-grade basis, age-stratified analysis were not performed. This approach is supported by evidence suggesting that grade level may have a stronger association with myopia than chronological age (12–13). A supplementary table reporting the mean age and SD for each grade is provided for reference (
Supplementary Table S1 ).This study underscores the public health importance of monitoring IOP as a potential target for myopia management in children and adolescents, expanding the focus beyond refractive correction to comprehensive ocular health, including the prevention of long-term complications (e.g., glaucoma). Finally, standardized protocols and nationwide sampling enhance the generalizability of the findings to similar populations.
In conclusion, using a large and representative sample, this study systematically characterizes the variation in IOP and its relationships with optometric parameters. The findings highlight the need for further research on IOP dynamics to inform myopia management strategies and support grade- and sex-specific IOP monitoring in pediatric populations to improve glaucoma prevention, myopia control, and overall ocular health.
-
All staff members who contributed to data collection and all students who participated in this study.
-
Approved by the Institutional Review Board of Beijing Center for Disease Prevention and Control (2022 No.24).
HTML
| Citation: |

|