
 Download:
Download:




-
Introduction: Tuberculosis preventive treatment (TPT) is pivotal in preventing the progression of latent tuberculosis infection (LTBI) to active tuberculosis (ATB). However, systematic, national data on TPT implementation in China are scarce. We characterized the scale-up of the TPT between 2022 and 2025, and identified the factors associated with its acceptance and completion.
Methods: This preplanned cross-sectional study utilized two levels of national TPT surveillance [31 provincial-level administrative divisions (PLADs), 2022–2025] and 2,676 individuals with LTBI (five PLADs, 2023–2024). The analyses included descriptive statistics and Firth-penalized logistic regression (R 4.3.1).
Results: The number of TPT recipients increased 2.5-fold (37,514–92,331) with approximately 79% short-course regimen use. The acceptance and completion rates were 45.14% and 85.18%, respectively. Higher acceptance was observed in individuals aged 15–44 years [odds ratio (OR)=0.648, 95% confidence interval (CI): 0.469, 0.896], ethnic minorities (OR=5.045, 95% CI: 1.910, 16.914), healthcare workers (OR=82.029, 95% CI: 16.422, 822.390), and designated hospitals (OR=3.620, 95% CI: 2.507, 5.281). It was lower in immunocompromised individuals (OR=0.409, 95% CI: 0.219, 0.749) and those with moderate PPD positivity (OR=0.384, 95% CI: 0.275, 0.533).
Conclusions: China has progressed in scaling up the TPT; however, low acceptance and subgroup disparities persist. Integrating TPT into routine clinical practice, prioritizing short-course regimens, and targeting high-risk groups are critical for TB elimination.
-
Tuberculosis (TB) remains a major global public health challenge, with 10.7 million new cases reported worldwide in 2024. China accounts for 6.5% of global cases (ranking fourth globally) (1), bearing a substantial TB burden. Latent tuberculosis infection (LTBI) refers to a persistent immune response to Mycobacterium tuberculosis antigens without clinical, bacteriological, or radiological evidence of active TB. As a vast reservoir for future TB cases, 5%–10% of individuals with LTBI develop active TB during their lifetime, severely hindering the global aim of ending the TB epidemic (2). The LTBI rates in China are 18.1% in individuals aged ≥5 years and 20.3% in those aged ≥15 years, indicating a considerable potential risk of active TB transmission. In the absence of an effective adult TB vaccine, tuberculosis preventive treatment (TPT) has emerged as a cornerstone intervention to block the progression of LTBI to active disease, making it indispensable for reducing TB incidence and advancing the elimination of the TB epidemic (3). Recognizing its critical significance, China has integrated TPT into its national TB control strategies and has successively issued key policies, including the TB Prevention and Control Management Guidelines (4) and the National TB Prevention and Control Plan (2024–2030) (5), which explicitly designate TPT as a core indicator of TB prevention efforts. However, despite these clear policy commitments, there remains a critical gap in national-level systematic data on TPT implementation, including coverage, adherence, and factors influencing its effectiveness. Moreover, both global and national TPT implementations face major challenges, such as low acceptance and completion rates, further limiting their effectiveness in TB control. This knowledge deficit not only restricts the ability to assess whether the TPT is meeting its intended public health goals but also hinders the optimization of strategies to achieve a broader impact. To address this gap, we analyzed the national TPT data from 2022 to 2025 to characterize the current implementation status, identify barriers in the care cascade, and explore the key influencing factors. The findings of this study provide evidence-based insights to refine China’s TPT policies and accelerate progress toward ending the TB epidemic.
This preplanned cross-sectional study used two-level data. Nationally, the TPT progress was analyzed using the 2022–2025 data for 31 provincial-level administrative divisions (PLADs) obtained from the Chinese Disease Control and Prevention Information System. Provincially, to identify factors influencing TPT acceptance, the Centers for Disease Control and Prevention (CDC) designated hospitals and health centers in five PLADs (Jiangsu, Henan, Shaanxi, Yunnan, and Xinjiang Uygur Autonomous Region) were selected via convenience sampling based on the implementation feasibility. Anonymized data were extracted using structured forms from routinely registered individuals with LTBI documented between 2023 and 2024. All eligible individuals recorded during the study period were included. The investigators were trained by public health staff from the participating institutions to ensure standardized procedures and consistent variable definitions. Quality control measures included supervisory reviews and data verification to ensure completeness and logical consistency across PLADs. Statistical analyses were performed using R (Version 4.4.3, Vienna, Austria, https://www.r-project.org/). Descriptive statistics summarized the national TPT progress. Associations with TPT acceptance were evaluated using univariate and multivariate Firth-penalized logistic regressions. Bidirectional stepwise selection (α=0.05 for entry and removal) was used to determine the final model. As a sensitivity analysis, multilevel logistic regression, with PLAD specified as a random intercept, was conducted to account for potential regional clustering.
The number of national TPT recipients increased steadily from 37,514 in 2022 to 92,331 in 2025, with students who have been in close contact with TB patients being the largest group across all years (21,654 in 2022 to 34,616 in 2025). In addition, close contacts with patients having bacteriologically positive TB also reported a sharp increase (7,683 in 2022 to 28,854 in 2025). Short-course regimens were the main TPT strategies, with utilization rates of 79.2% (29,725/37,514) in 2022, 78.8% (41,639/52,836) in 2023, 76.5% (66,555/87,034) in 2024, and 79.6% (73,517/92,331) in 2025, which remained consistently high throughout the study period (Figure 1).
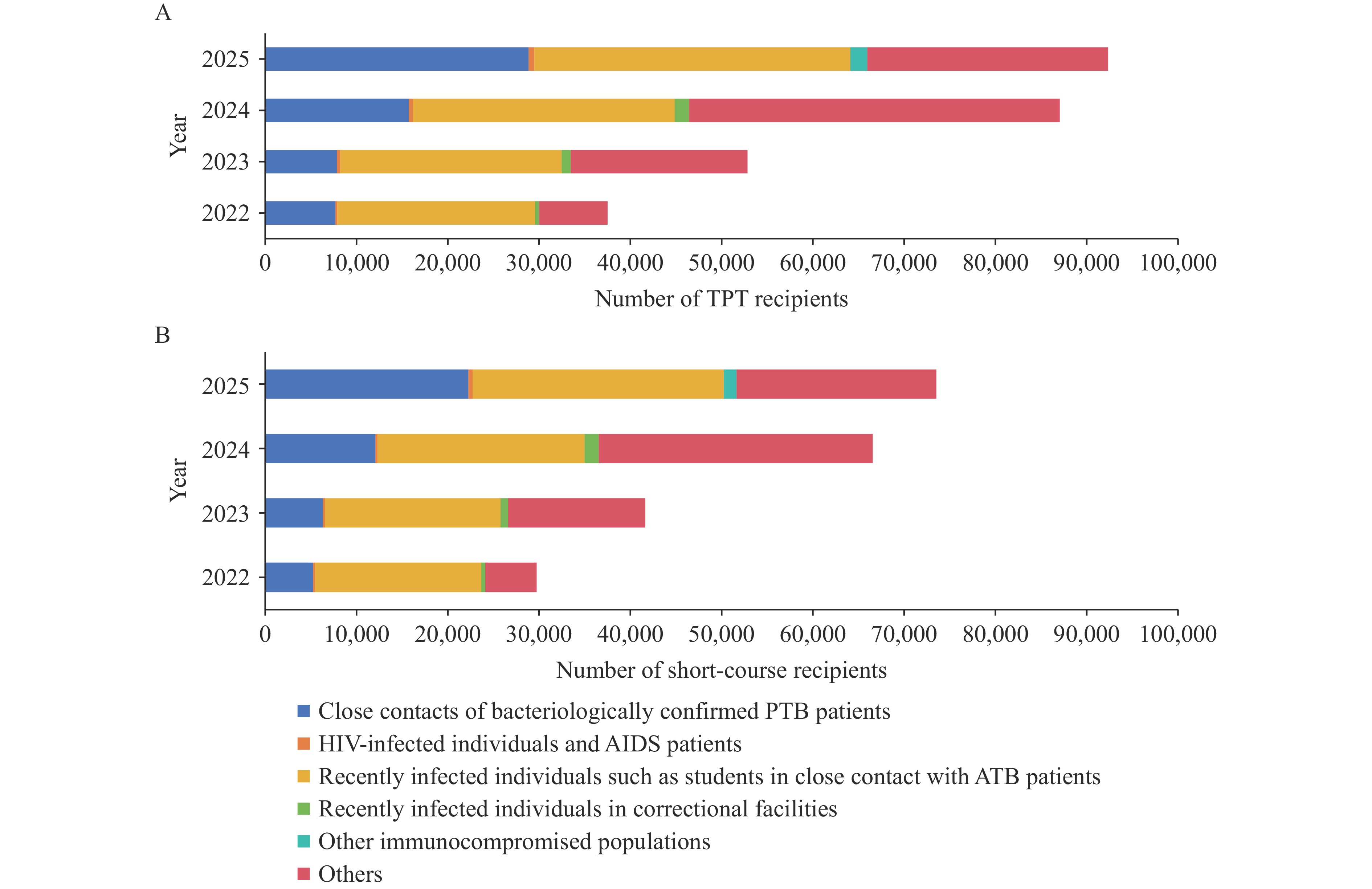 Figure 1.
Figure 1.TPT implementation and scale-up in China from 2022 to 2025. (A) Individuals on TPT; (B) Individuals on shorter regimens.
Abbreviation: PTB=pulmonary tuberculosis; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome; ATB=active tuberculosis; TPT=tuberculosis preventive treatment.In total, 2,676 individuals with LTBI were included in the survey. The overall acceptance rate of the TPT was 45.14% (1,208/2,676). Among those who initiated TPT, 85.18% (1,029/1,208) completed the full course (Table 1).
Variable Total (n) TPT acceptance [n/(%)] TPT completion [n/(%)] Total 2,676 1,208 45.14 1,029 85.18 Age (years) 0–14 453 215 47.46 193 89.77 15–44 1,416 599 42.30 491 81.97 45–59 273 191 69.96 161 84.29 ≥60 534 203 38.01 184 90.64 Gender Male 1,343 587 43.71 512 87.22 Female 1,333 621 46.59 517 83.25 Ethnicity Han 2,179 784 35.98 641 81.76 Other ethnic groups 497 424 85.31 388 91.51 PLAD Henan 1,038 143 13.78 105 73.43 Jiangsu 387 304 78.55 253 83.22 Shanxi 207 14 6.76 2 14.29 Xinjiang Uygur Autonomous Region 460 387 84.13 354 91.47 Yunnan 584 360 61.64 315 87.50 Education level Junior school and below 1,292 692 53.56 617 89.16 Senior high school 1,066 294 27.58 247 84.01 College and above 318 222 69.81 165 74.32 Population classification HIV/AIDS and other immunocompromised 402 76 18.91 66 86.84 Household close contacts of TB patients 568 448 78.87 385 85.94 Densely populated place population 1,646 635 38.58 545 85.83 Healthcare workers 25 24 96.00 10 41.67 Other 35 25 71.43 23 92.00 TPT-providing institution CDC 297 63 21.21 41 65.08 Designated hospital 1,948 962 49.38 837 87.01 Health center 431 183 42.46 151 82.51 Infection test result PPD strong positive 1,479 811 54.83 713 87.92 PPD moderate positive 675 96 14.22 85 88.54 TBST positive 438 229 52.28 177 77.29 IGRA positive 84 72 85.71 54 75.00 TPT regimen 6-9H – 46 – 39 84.78 3H2P2 – 474 – 431 90.93 3HR – 529 – 453 85.63 Immunotherapy – 207 – 106 51.21 Note: “–” means data not available.
Abbreviation: TPT=tuberculosis preventive treatment; LTBI=latent tuberculosis infection; PLAD=provincial-level administrative division; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome; TB=tuberculosis; CDC=Centers for Disease Control and Prevention; PPD=purified protein derivative; TBST=tuberculosis skin test; IGRA=interferon-gamma release assay; H=isoniazid; P=rifapentine; R=rifampicin; Ref.=reference group; 6-9H=a 6-month or 9-month regimen of daily isoniazid monotherapy, H 5 mg/kg (max 300 mg) daily; 3H2P2=a 3-month regimen of twice-weekly isoniazid plus rifapentine, ≥50 kg: H 600 mg and P 600 mg twice weekly, <50 kg: H 500 mg and P 450 mg twice weekly; 3HR=a 3-month regimen of weekly isoniazid plus rifampicin, ≥50 kg: H 300 mg and P 600 mg twice weekly, <50 kg: H 300 mg and P 450 mg daily; Immunotherapy=a 3-month immunotherapy regimen consisting of Mycobacterium bovis vaccine administered once every 2 weeks.Table 1. TPT acceptance and completion rates among individuals with LTBI by demographic and clinical characteristics, China, 2023–2024.
Multivariate logistic regression analysis identified several factors that were significantly associated with TPT acceptance. Key factors included age [15–44 vs. 0–14: odds ratio (OR)=0.648, 95% confidence interval (CI): 0.469, 0.896, P=0.009]; ethnicity (other ethnic groups vs. Han: OR=5.045, 95% CI: 1.910, 16.914, P<0.001); PLAD (e.g., Jiangsu vs. Henan: OR=31.499, 95% CI: 15.320, 68.720, P<0.001; Xinjiang vs. Henan: OR=8.610, 95% CI: 2.353, 26.462, P=0.002); education level (senior high school vs. junior school and below: OR=0.721, 95% CI: 0.527, 0.986, P=0.041); population classification (HIV/AIDS/immunocompromised vs. densely populated place population: OR=0.409, 95% CI: 0.219, 0.749, P=0.004; healthcare workers vs. densely populated place population: OR=82.029, 95% CI: 16.422, 822.390, P<0.001); TPT-providing institution (designated hospital vs. CDC: OR=3.620, 95% CI: 2.507, 5.281, P<0.001); and infection test result (PPD moderate positive vs. PPD strong positive: OR=0.384, 95% CI: 0.275, 0.533, P<0.001) (Table 2). Completion rates varied considerably across subgroups, being notably low for healthcare workers (41.67%) and those on immunotherapy regimens (51.21%) but high for ethnic minorities (91.51%) and the elderly (90.64%). The random-intercept variance for the PLADs was 1.93, suggesting moderate between-provincial heterogeneity. However, the fixed-effect estimates were not materially altered (
Supplementary Table S1 ).Variable Univariate analysis Multivariate analysis P OR (95% CI) P OR (95% CI) Age (years) 0–14 Ref. Ref. 15–44 0.054 0.812 (0.656, 1.004) 0.009 0.648 (0.469, 0.896) 45–59 <0.001 2.569 (1.876, 3.539) 0.136 0.695 (0.432, 1.122) ≥60 0.003 0.679 (0.527, 0.875) 0.254 0.735 (0.435, 1.250) Gender Male Ref. Ref. Female 0.135 1.123 (0.965, 1.308) 0.388 1.096 (0.890, 1.350) Ethnicity Han Ref. Ref. Other ethnic groups <0.001 10.274 (7.949, 13.450) <0.001 5.045 (1.910, 16.914) PLAD Henan Ref. Ref. Jiangsu <0.001 22.757 (16.948, 30.861) <0.001 31.499 (15.320, 68.720) Shaanxi 0.004 0.468 (0.256, 0.794) 0.470 0.726 (0.301, 1.723) Xinjiang Uygur Autonomous Region <0.001 32.900 (24.382, 44.927) 0.002 8.610 (2.353, 26.462) Yunnan <0.001 10.021 (7.881, 12.804) <0.001 6.198 (4.363, 8.869) Education level Junior school and below Ref. Ref. Senior high school <0.001 0.331 (0.278, 0.393) 0.041 0.721 (0.527, 0.986) College and above <0.001 1.999 (1.542, 2.609) 0.208 0.787 (0.542, 1.142) Population classification HIV/AIDS and other immunocompromised <0.001 0.373 (0.284, 0.485) 0.004 0.409 (0.219, 0.749) Household close contacts of TB patients <0.001 5.924 (4.749,7.438) 0.002 0.454 (0.275, 0.744) Densely populated place population Ref. Ref. Healthcare workers <0.001 25.997 (6.752, 233.246) <0.001 82.029 (16.422, 822.390) Other <0.001 3.865 (1.924, 8.342) 0.014 0.260 (0.097, 0.752) TPT-providing institution CDC Ref. Ref. Designated hospital <0.001 3.603 (2.710, 4.855) <0.001 3.620 (2.507, 5.281) Health center <0.001 2.727 (1.956, 3.838) 0.064 1.892 (0.963, 3.664) Infection test result PPD strong positive Ref. Ref. PPD moderate positive <0.001 0.137 (0.108, 0.173) <0.001 0.384 (0.275, 0.533) TBST positive 0.347 0.902 (0.729, 1.117) 0.734 0.901 (0.485, 1.626) IGRA positive <0.001 4.778 (2.695, 9.205) 0.514 1.363 (0.539, 3.506) Abbreviation: TPT=tuberculosis preventive treatment; LTBI=latent tuberculosis infection; PLAD=provincial-level administrative division; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome; TB=tuberculosis; PPD=purified protein derivative; TBST=tuberculosis skin test; IGRA=interferon-gamma release assay; OR=odds ratio; CI=confidence interval; Ref.=reference group. Table 2. Univariate and multivariable logistic regression analyses of factors associated with TPT acceptance among individuals with LTBI, China, 2023–2024.
-
LTBI affects nearly one-quarter of the global population, forming the largest reservoir of ATB and hindering its global elimination (6). TPT effectively halts LTBI progression to ATB (7); however, its global implementation is compromised by low acceptance and completion rates (8). We addressed the evidence gap by investigating TPT uptake, completion, and associated factors among individuals with LTBI in China to identify optimized national prevention strategies.
We demonstrated that China’s TPT scale-up achieved remarkable progress during 2022–2025, with a 2.5-fold increase in recipients and consistently high utilization (around 79%) of WHO-recommended short-course regimens, validating the effectiveness of national TB control policies. Although the post-acceptance completion rate (85.18%) indicated good adherence, the overall acceptance rate (45.14%) was a critical bottleneck, with stark disparities across subgroups: acceptance was extremely low in adults ≥60 years, individuals living with HIV/AIDS (PLHIV), immunocompromised individuals and Shaanxi residents, but high in healthcare workers, ethnic minorities, and Jiangsu/Xinjiang residents. Grassroots institutions (designated TB hospitals and community health centers) outperformed CDCs in TPT delivery, underscoring the value of routine clinical settings for preventive care. Therefore, policies must shift the focus from merely promoting completion to actively facilitating acceptance. Our data strongly advocate for the integration of TPT services into designated hospitals and health centers, which are associated with four-fold and two-fold higher odds of acceptance, respectively, compared to CDC facilities. This suggests a policy shift toward not “mainstreaming” TPT into routine clinical care settings where patients already seek services, potentially improving the accessibility and perceived legitimacy of treatment (9). Secondly, the superior completion rate of the 3H2P2 regimen (90.93%) supports the urgent need for national programs to prioritize the procurement and rollout of shorter, patient-friendly regimens to improve overall program effectiveness (10). Third, identified risk groups, such as immunocompromised individuals and residents of low-performing PLADs, require tailored proactive outreach strategies. For example, seamlessly integrating TPT acceptance into HIV care clinics and implementing performance-based financing for TPT in lagging regions could be effective measures derived from our evidence.
The findings in this report are subject to at least two limitations. First, the survey on TPT influencing factors used convenience sampling, selecting PLADs/counties with active screening and complete data, which may have led to selection bias and limited the generalizability of the results to the whole country. Second, the surveillance data did not include detailed information on TPT follow-up and adverse reactions, which may be crucial factors influencing TPT completion, and were not analyzed in this study.
To optimize China’s TPT strategy and effectiveness, targeted recommendations based on study findings include prioritizing TPT for high-risk groups, such as student close contacts and bacteriologically positive TB patient contacts. In addition, personalized measures (simplified screening, free drugs, and regular follow-ups) should be used for the elderly (≥60 years), HIV-infected, and immunocompromised individuals to improve acceptance. Optimizing grassroots services involves shifting TPT from CDCs to designated hospitals and community/township health centers; training grassroots staff on TPT screening, regimen selection, and adverse reactions; and establishing standardized processes to improve accessibility and quality. Standardizing short-course regimens and expanding coverage require maintaining high utilization of 3HR/3H2P2 through regular safety and effectiveness evaluations, resuming standardized TPT for detainees, and expanding coverage for immunocompromised groups via standardized protocols. Establishing a comprehensive TPT cascade system involves integrating LTBI screening, TPT acceptance, adherence, and follow-up into the national TB surveillance to track cascade losses and promptly address implementation barriers. Finally, promoting regional balance includes increasing financial and technical support for low-acceptance central/western regions (e.g., Shaanxi), establishing cross-regional platforms for experience sharing, and narrowing implementation disparities.
-
The Centers for Disease Control and Prevention (Health Supervision Institutions), designated hospitals, and health centers in Jiangsu, Henan, Shanxi, Shaanxi, Yunnan, and Xinjiang Uygur Autonomous Regions. We also thank all the staff involved in data collection and data entry for their invaluable contributions and technical support.
HTML
| Citation: |

|