
 Download:
Download:




-
Tuberculosis (TB), caused by Mycobacterium tuberculosis, remains one of the leading causes of death worldwide. According to the World Health Organization (WHO) Global TB Report, an estimated 10.7 million new TB cases occur annually, and approximately one-fourth of the global population is infected with M. tuberculosis (1). China reports approximately 696,000 new TB cases each year, ranking fourth among the 30 high-burden countries. Consequently, TB control remains a central priority under the “Healthy China 2030” strategy.
TB has a multi-stage natural history that includes latent infection, asymptomatic infection, and symptomatic active disease (2). Asymptomatic pulmonary tuberculosis (aPTB) is defined as "individuals without, unaware of, or not reporting symptoms during screening or history-taking, and without clinical signs indicative of TB" (3). National prevalence surveys indicate that 36%–80% of bacteriologically confirmed TB cases are asymptomatic (4). Although these individuals do not present with typical symptoms, such as persistent cough or fever, they may remain infectious and contribute to unrecognized community transmission (5). Preventing such transmission is essential to achieving the WHO End-TB strategy.
Traditional TB surveillance systems and burden estimates have focused primarily on symptomatic and active cases of TB, resulting in a limited understanding of the prevalence and burden of aPTB in China. To address this gap, a systematic analysis of the epidemiological characteristics and temporal trends of aPTB was performed across China. This study aimed to provide evidence to inform TB surveillance, prevention, and control policies, thereby addressing existing gaps, supporting national efforts to reduce TB incidence and advance progress toward the elimination of TB.
HTML
-
Data were obtained from the China Information System for Disease Control and Prevention, a mandatory nationwide surveillance platform operated by the China CDC. The eligibility criteria included TB cases reported between January 1, 2021, and December 31, 2024, with complete symptom records. During this study period, 2,210,063 TB cases were registered in the system. Of these, 1,228,398 cases were excluded due to incomplete symptom data, leaving 981,665 eligible cases for further analysis. Subsequently, 8,366 records were excluded because they were ineligible, including extrapulmonary TB, non-tuberculous mycobacterial (NTM) infection, duplicate entries, and logical inconsistencies. The final analytical sample comprised 973,299 PTB cases.
-
aPTB was defined as PTB cases without documentation of “cough” in the symptom field (6). Cough is the most common and characteristic symptom of PTB and is typically the primary reason individuals seek TB-related medical care. This operational definition is consistent with clinical practice.
-
Data were cleaned and organized using Microsoft Excel (version 2021, Microsoft, Redmond, USA, https://www.microsoft.com/) to remove duplicate records and resolve logical inconsistencies. Descriptive statistics were used to examine temporal (annual and monthly) and demographic (age, sex, and occupation) distributions. All statistical analyses were conducted using R software (version 4.3.0, Vienna, Austria, https://www.r-project.org/). Temporal trends were assessed using the Cochran-Armitage trend test.
Data Source
Case Definition
Statistical Analysis
-
A total of 973,299 PTB cases with complete symptom records from 2021 to 2024 were included in the analysis. Of these, 162,151 (16.66%) were asymptomatic and classified as aPTB. Bacteriological confirmation was obtained in 48.60% of aPTB cases and 68.45% of symptomatic PTB cases. Statistical analysis revealed significant annual differences in the proportion of aPTB cases (χ2=633.70, P<0.001), along with a significant downward temporal trend (Z=−9.35, P<0.001). The proportion of aPTB cases peaked in 2022 (18.07%; incidence: 3.69 per 100,000), followed by slight fluctuations in 2023 (16.04%; incidence: 3.82 per 100,000) and 2024 (16.31%; incidence: 3.30 per 100,000) (Table 1).
Year Asymptomatic PTB Symptomatic PTB Total Number Incidence (/100,000) Proportion
(%)Number Incidence (/100,000) Proportion
(%)2021 9,750 0.69 15.17 54,520 3.86 84.83 64,270 2022 52,050 3.69 18.07 236,031 16.72 81.93 288,081 2023 53,882 3.82 16.04 282,145 20.01 83.96 336,027 2024 46,469 3.30 16.31 238,452 16.93 83.69 284,921 Total 162,151 2.87 16.66 811,148 14.38 83.34 973,299 Abbreviation: PTB=pulmonary tuberculosis; aPTB=asymptomatic pulmonary tuberculosis. Table 1. Number and proportions of aPTB cases in China, 2021–2024.
-
The analysis examined the age, gender, and occupational distributions of nationally registered PTB cases from 2021 to 2024. Significant differences were observed between the aPTB and sPTB groups across all three characteristics (Figure 1; χ2=603.99 for sex, χ2=16,103.30 for age, and χ2=19,288.66 for occupation; all P<0.001). Regarding age distribution, the highest incidence of aPTB was observed among individuals aged ≥75 years (20.47 per 100,000), 65–74 years (20.37 per 100,000), and 55–64 years (15.93 per 100,000). Similarly, sPTB cases were most concentrated in the same age groups: ≥75 years (150.65 per 100,000), 65–74 years (141.34 per 100,000), and 55–64 years (94.94 per 100,000). With respect to sex distribution, the male-to-female ratio was 1.96∶1 in the aPTB group and 2.26∶1 in the sPTB group, indicating a consistent male predominance across most age groups in both cohorts. Among individuals aged ≥75 years, males accounted for 68.38% of aPTB cases. In terms of occupation, the three most common categories among aPTB were farmers and herders (50.87%), homemakers and unemployed (18.36%), and students (11.32%). Among sPTB cases, farmers and herders (65.47%), homemakers and unemployed (16.19%), and retirees (5.08%) were the predominant occupational groups (Figure 1).
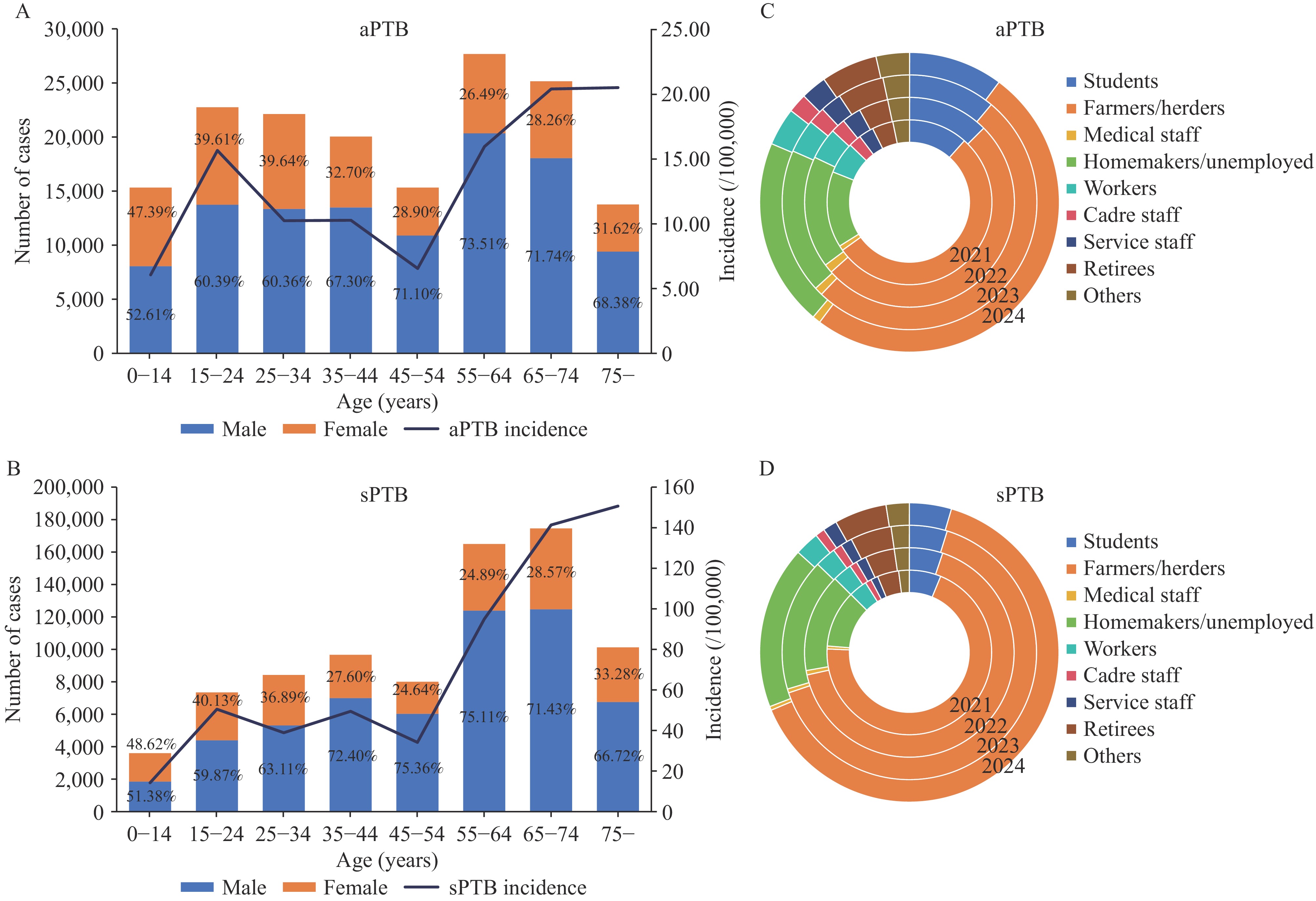 Figure 1.
Figure 1.Population distribution of aPTB and sPTB cases in China between 2021 and 2024. (A) Age distribution of aPTB cases; (B) Age distribution of sPTB cases; (C) Occupational distribution of aPTB cases; (D) Occupational distribution of sPTB cases .
Abbreviation: aPTB=asymptomatic pulmonary tuberculosis; sPTB=symptomatic pulmonary tuberculosis. -
Over the four-year study period, the annual number of aPTB cases remained relatively stable (9,750 in 2021, 53,882 in 2023 (peak), and 46,469 in 2024), whereas the number of sPTB cases fluctuated more substantially (54,520 in 2021, 282,145 in 2023 (peak), and 238,452 in 2024). Statistical analysis confirmed significant monthly variation in the proportion of aPTB cases (χ2=2,790.27, P<0.001). The number of aPTB cases increased from February (10,354 cases, accounting for 6.39% of the cumulative TB total) to a peak in August (15,722 cases, 9.70%), followed by a gradual decline through December (11,172 cases, 6.89%). For sPTB, the number of cases peaked in March (79,047 cases, 9.75% of the monthly TB total) and July (73,724 cases, 9.09%), with the lowest number of cases recorded in December (57,177 cases, 7.05%) (Figure 2).
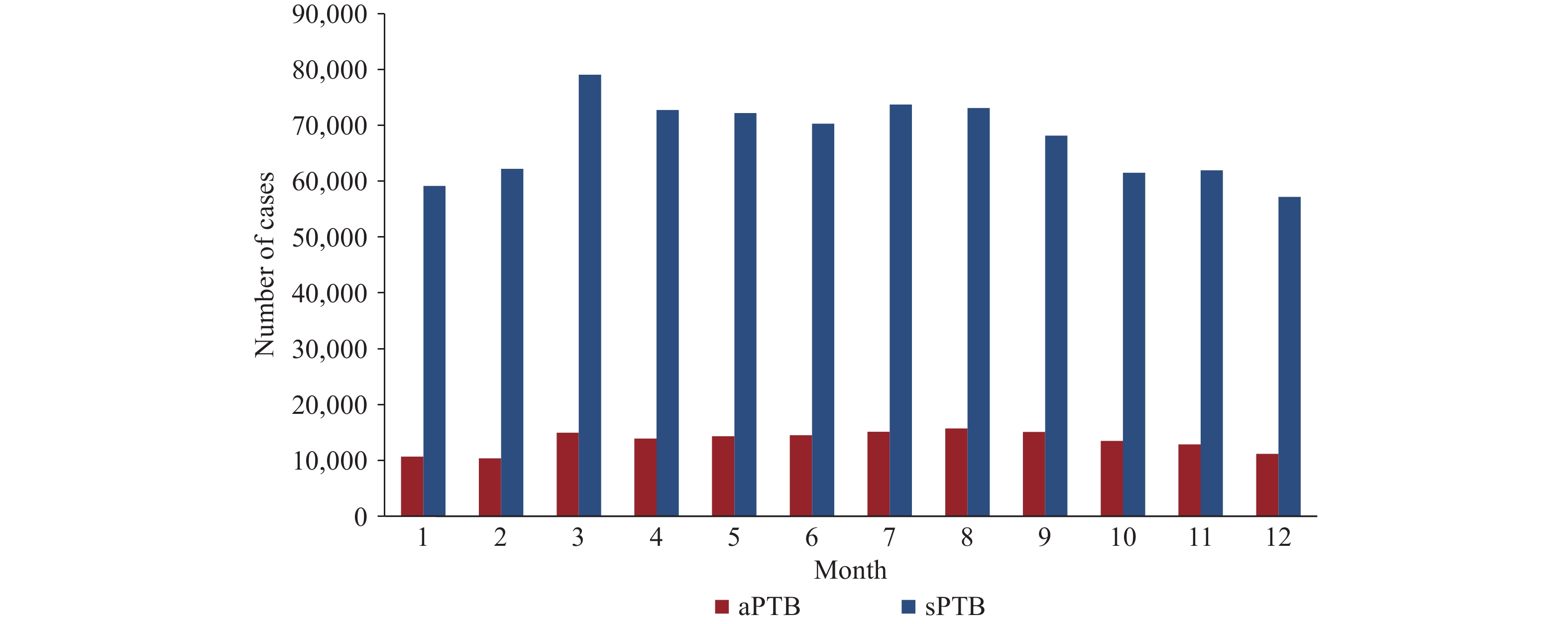 Figure 2.
Figure 2.Temporal distribution of aPTB and sPTB cases in China between 2021 and 2024.
Abbreviation: aPTB=asymptomatic pulmonary tuberculosis; sPTB= symptomatic pulmonary tuberculosis. -
From 2021 to 2024, the 5 provincial-level administrative divisions (PLADs) with the highest registration rates of aPTB were Xizang (9.50 per 100,000 population), Guizhou (7.56 per 100,000 population), Yunnan (5.30 per 100,000 population), Xinjiang (5.09 per 100,000 population), and Hubei (4.92 per 100,000 population). During the same period, the 5 PLADs with the highest registration rates of sPTB were Guizhou (42.12 per 100,000 population), Xizang (40.62 per 100,000 population), Xinjiang (35.19 per 100,000 population), Qinghai (34.39 per 100,000 population), and Guangxi (30.18 per 100,000 population) (Figure 3).
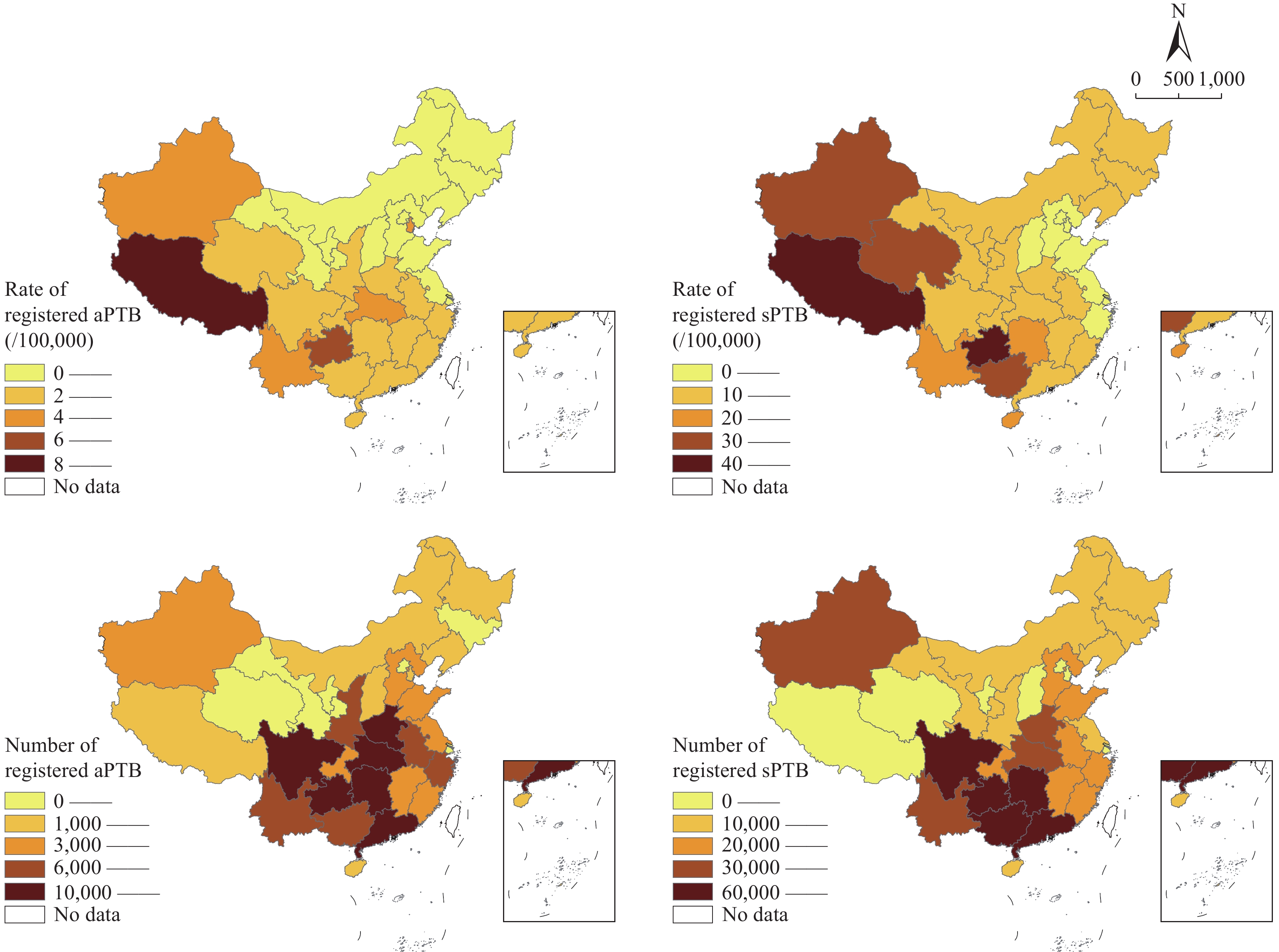 Figure 3.
Figure 3.Regional distribution of aPTB and sPTB cases in China, 2021–2024.
Abbreviation: aPTB= asymptomatic pulmonary tuberculosis; sPTB=symptomatic pulmonary tuberculosis.
Map approval number: GS京(2026) 0610号.
Overall Burden
Epidemiological Characteristics
Population distribution
Temporal distribution
Regional Distribution
-
This analysis describes the epidemiological characteristics of aPTB in China from 2021 to 2024 and provides insight into its burden and distribution. aPTB accounted for 16.66% of all TB cases with complete symptom records during the study period, indicating a substantial hidden burden. Although the proportion of aPTB declined over the four-year period, this trend may reflect changes in diagnostic sensitivity and healthcare-seeking behavior rather than a true reduction in asymptomatic disease. In terms of population distribution, aPTB was most common among individuals aged ≥75 years (corresponding to the highest aPTB incidence of 20.47 per 100,000) and 65–74 years (20.37 per 100,000). The male-to-female ratio for aPTB was lower than that for sPTB, although a male predominance persisted. Farmers and herders, homemakers and unemployed, and students represented the primary occupational groups. Spatially, high-incidence areas of aPTB were concentrated in western and southwestern China, partially overlapping with sPTB hotspots.
The 16.66% proportion of aPTB in this study falls within the 14.2%–43.1% range reported by the national epidemiological surveys conducted in 2000 and 2010 (7–8), but is lower than the 47.7% reported in a high-risk population study by Zhang et al. (9). This discrepancy likely reflects differences in study populations. Zhang et al. focused on high-risk groups such as older adults and patients with diabetes who may be more likely to have asymptomatic disease, whereas the present study included all registered TB cases with complete symptom records. Internationally, a multicountry study across 12 Asian and African countries reported a 39.8% proportion of aPTB (adjusted to 62.5%) using a “no cough” definition (6), exceeding the current estimate. Differences in epidemic disparities, screening strategies, and case definitions may explain this variation (10). The use of a “no cough” definition in this study may have modestly overestimated the proportion of aPTB compared with stricter definitions requiring the absence of all TB-related symptoms. Nevertheless, cough is the principal symptom prompting TB-related healthcare-seeking; therefore, this operational definition aligns with public health priorities. The lower bacteriological confirmation rate observed for aPTB compared with sPTB likely reflects earlier disease stage and lower mycobacterial load, which reduce microbiological detectability. Despite this limitation, bacteriologically positive aPTB cases warrant close attention, as they may contribute to silent transmission and sustain hidden transmission chains.
Several factors may explain the epidemiological patterns observed (11). The higher incidence of aPTB among older adults may be related to the age-associated immune decline, which increases susceptibility to Mycobacterium tuberculosis while producing atypical or mild clinical manifestations. This interpretation is consistent with findings from a study conducted in Zhejiang Province (8), where aPTB was more common among older individuals. In terms of occupational distribution, the high proportion of farmers and herders with aPTB likely reflects limited access to healthcare services, lower awareness of TB prevention and control, and fewer routine health examinations in rural and pastoral areas, resulting in the delayed detection of asymptomatic infections. Similar conclusions were reported by Gao et al. (12).
In terms of temporal distribution, the relative stability of aPTB and its mild seasonal variation may reflect the chronic nature of asymptomatic infection. Unlike symptomatic TB, which may be influenced by climatic conditions and population gathering activities, aPTB often progresses slowly and may be less sensitive to short-term seasonal changes.
The regional concentration of aPTB in high-incidence areas appears to be closely linked to geographical environment and socioeconomic factors (13). The western and southwestern regions of China have complex geographical environments, relatively low socioeconomic levels, poor living conditions, and insufficient medical resources, which may facilitate the spread of M. tuberculosis. Furthermore, high levels of internal migration may further increase the risk of undetected aPTB transmission. The regional distribution detected by the current analyses was also affected by regional epidemic levels and screening strategies.
Regions with high incidence of both sPTB and aPTB, including Tibet, Guizhou, and Xinjiang, are nationally recognized high-burden areas. Among non-overlapping high-incidence regions, areas with high sPTB incidences (e.g., Qinghai and Guangxi) are also high-TB-incidence regions nationally, whereas elevated aPTB detection in Yunnan, Hubei, and other regions may reflect proactive case-finding initiatives. Yunnan piloted an active pulmonary TB case-finding strategy in 2016 and promoted expanded active screening efforts in 2019 (14). These interventions likely enhanced aPTB detection, thus enabling the timely identification and reporting of more aPTB cases.
This study has several limitations. First, the analysis was restricted to registered TB cases with complete symptom records, which may have introduced selection bias. Unregistered aPTB cases, including individuals who were not screened or had incomplete records, were not captured. Therefore, the true burden of aPTB may be underestimated. Second, the analysis focused on epidemiological characteristics of aPTB from the perspectives of population, time, and region and did not examine biological factors (e.g., M. tuberculosis strain virulence) or individual behavioral factors (e.g., smoking, alcohol use, and living conditions) that may influence the occurrence of aPTB. The absence of these variables limits a more comprehensive understanding of the pathogenesis of aPTB.
These findings have important implications for optimizing TB prevention and control strategies in China and strengthening aPTB management. The relatively high proportion of aPTB cases indicates that reliance solely on symptom-based screening may be insufficient. Expanding imaging and etiological screening is crucial, particularly among high-risk populations. First, stratified active case finding (ACF) should be implemented for high-risk groups, including older adults, adolescents, farmers, and herders. Regular TB screening among elderly individuals and students, along with expanded outreach in rural and pastoral areas, could facilitate earlier detection and reduce the potential risk of transmission. Second, given the geographic concentration of high-incidence areas, increased investment in medical and healthcare resources in western and southwestern China is needed. Upgrade TB diagnosis and treatment capacity in these regions, and intensify health education initiatives to raise public awareness in the prevention and control of aPTB. Third, the substantial proportion of aPTB cases during the study period suggests that aPTB is an important component of the TB burden in China. It is necessary to incorporate aPTB prevention and control into the national TB prevention and control plan, formulate targeted prevention and control measures, and promote the early realization of the global goal of ending the TB epidemic. Finally, these analyses showed that aPTB has a mild seasonal pattern. This finding can provide a basis for the rational allocation of medical resources and the strengthening of screening, diagnosis, and treatment strategies in peak months (such as August) to improve the efficiency of case management.
| Citation: |

|