
 Download:
Download:




-
Tuberculosis (TB) remains the leading cause of death due to infectious diseases worldwide. According to the Global Tuberculosis Report 2025 released by the World Health Organization (WHO), an estimated 10.7 million people developed TB and approximately 1.23 million died from the disease in 2024, underscoring the persistent gap between global targets and epidemiological reality (1). Although the WHO End TB Strategy defines a unified set of ambitious global targets to reduce incidence, mortality, and catastrophic expenditures by 2030 (2), progress has been uneven across regions and countries, reflecting differences in health system capacity, socioeconomic conditions, and epidemic trajectories. In some low- and intermediate-burden settings, progress that once appeared promising has slowed or even reversed. At the same time, concerns over reduced international donor funding threaten the sustainability of TB control gains in many countries (3-4). These trends underscore that achieving End TB targets will require not only effective technical interventions but also sustained financing, strong governance, and context-specific implementation strategies.
In stark contrast to the overall stagnation of global TB control efforts, China has achieved remarkable progress. According to the WHO Global Tuberculosis Report 2025, China is estimated to have reduced its TB incidence rate by approximately 20% from 65 per 100,000 people in 2015 to 49 per 100,000 people in 2024, suggesting a transition toward a lower incidence setting (1). Nevertheless, significant disparities persist across provincial-level administrative divisions (PLADs), largely driven by differences in economic development, health system capacity, population density, and internal migration patterns (5). Western and central PLADs generally exhibit a higher incidence and longer diagnostic delays, whereas the more economically developed eastern PLADs benefit from stronger surveillance and treatment infrastructure.
In response to the renewed global commitments emphasized in the 2023 United Nations High-Level Meeting Political Declaration on Ending TB, China has strengthened its comprehensive TB control strategy across a continuum of prevention, diagnosis, treatment, and care. National targets have been translated into specific provincial goals to support implementation and accountability, while innovative policy initiatives, particularly the nationwide expansion of zero-TB communities, demonstrate China’s efforts to operationalize broad strategic frameworks into locally adapted interventions. This multilayered, goal-oriented framework reflects a country’s efforts to harmonize national priorities with local realities, reduce inter-provincial disparities, and provide a directly replicable blueprint for low- and middle-income countries.
-
In 2024, national planning targets were established to reduce the incidence of TB to below 50 per 100,000 people by 2025 and to below 43 per 100,000 people by 2030 (6). To support the achievement of the 2030 goal, the 2025 TB incidence was estimated using notification data adjusted for underreporting and underdiagnosis, and provincial-specific incidence reduction targets were formulated (Figure 1). By 2025, the PLADs with relatively high TB burdens are expected to remain concentrated in western China, including Guizhou (87.2 per 100,000), Tibet (80.0 per 100,000), Qinghai (79.4 per 100,000), Xinjiang (65.0 per 100,000), and Hainan (60.0 per 100,000), all exceeding the national target threshold of 50 per 100,000.
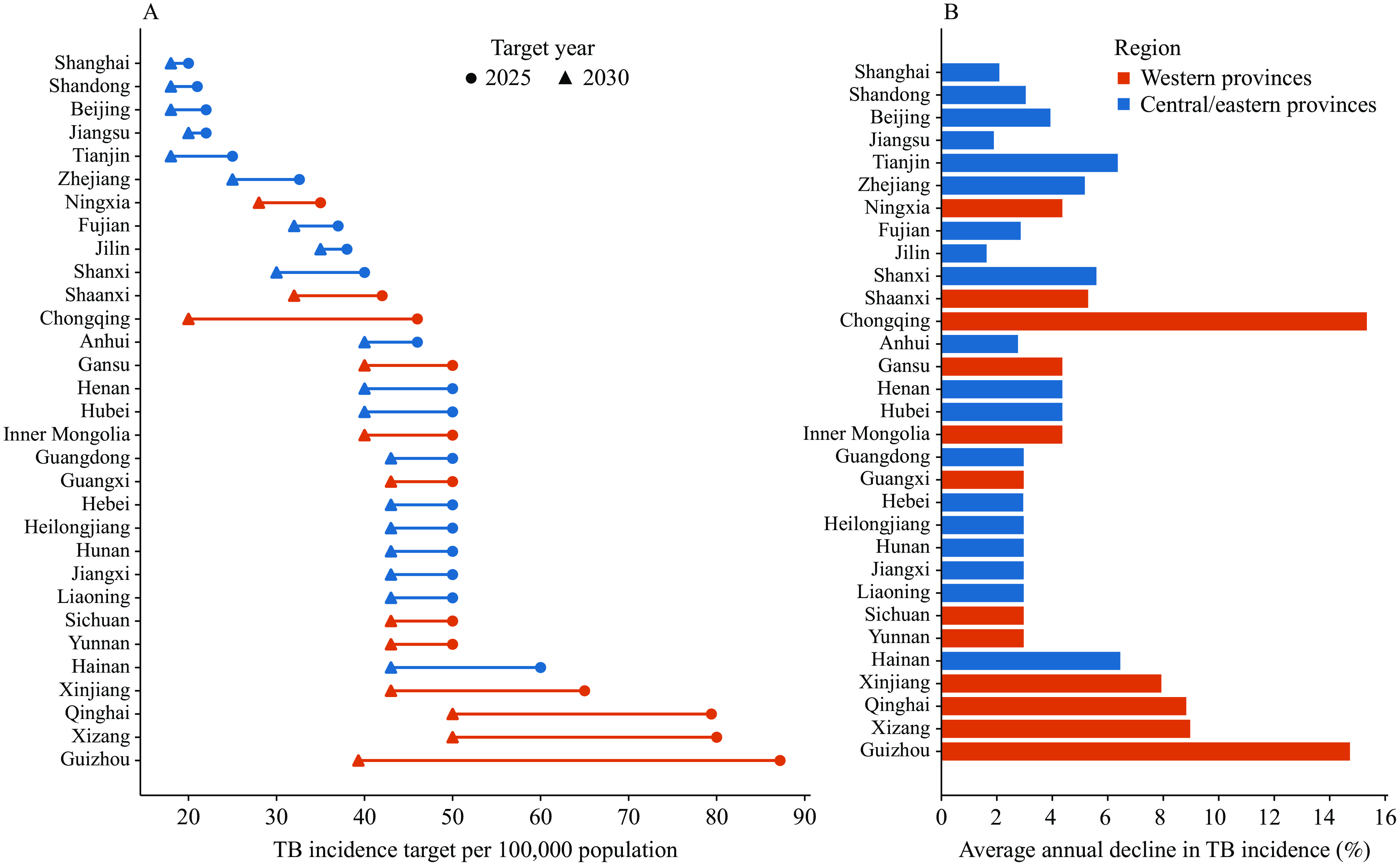 Figure 1.
Figure 1.Provincial TB incidence targets and projected annual declines across provinces in China. (A) Provincial TB incidence targets for 2025 to 2030. (B) Provincial average annual decline in TB incidence from 2025 to 2030 across provinces, shown using the same regional classification.
Note: In panel A, the circles denote the 2025 target and triangles denote the 2030 target, with lines linking the two targets within each province. Provinces are grouped by region as western provinces and central/eastern provinces.
Abbreviation: TB=tuberculosis.
Each PLAD subsequently establishes its own 2030 incidence-reduction target based on local epidemiological trends and programmatic capacity. Notably, Chongqing (15.34%), Guizhou (14.73%), Tibet (8.97%), Qinghai (8.83%), and Xinjiang (7.93%) had annual decline rates exceeding 7%. If all PLADs achieve their respective targets, the population-weighted national TB incidence will decline to 34.9 per 100,000 people by 2030, thereby meeting the national goal of remaining below 43 per 100,000.
-
China is implementing a comprehensive strategy that covers the entire process of TB prevention and control (Figure 2), ranging from reducing incidence through robust early detection and prevention using a community-based zero-TB approach, to ensuring timely treatment and comprehensive patient management through a multi-sectoral collaboration mechanism to implement the One Health policy. This strategy relies on a strong health system, sound financial support mechanisms, and extensive public awareness campaigns to ensure the achievement of the national TB control goals.
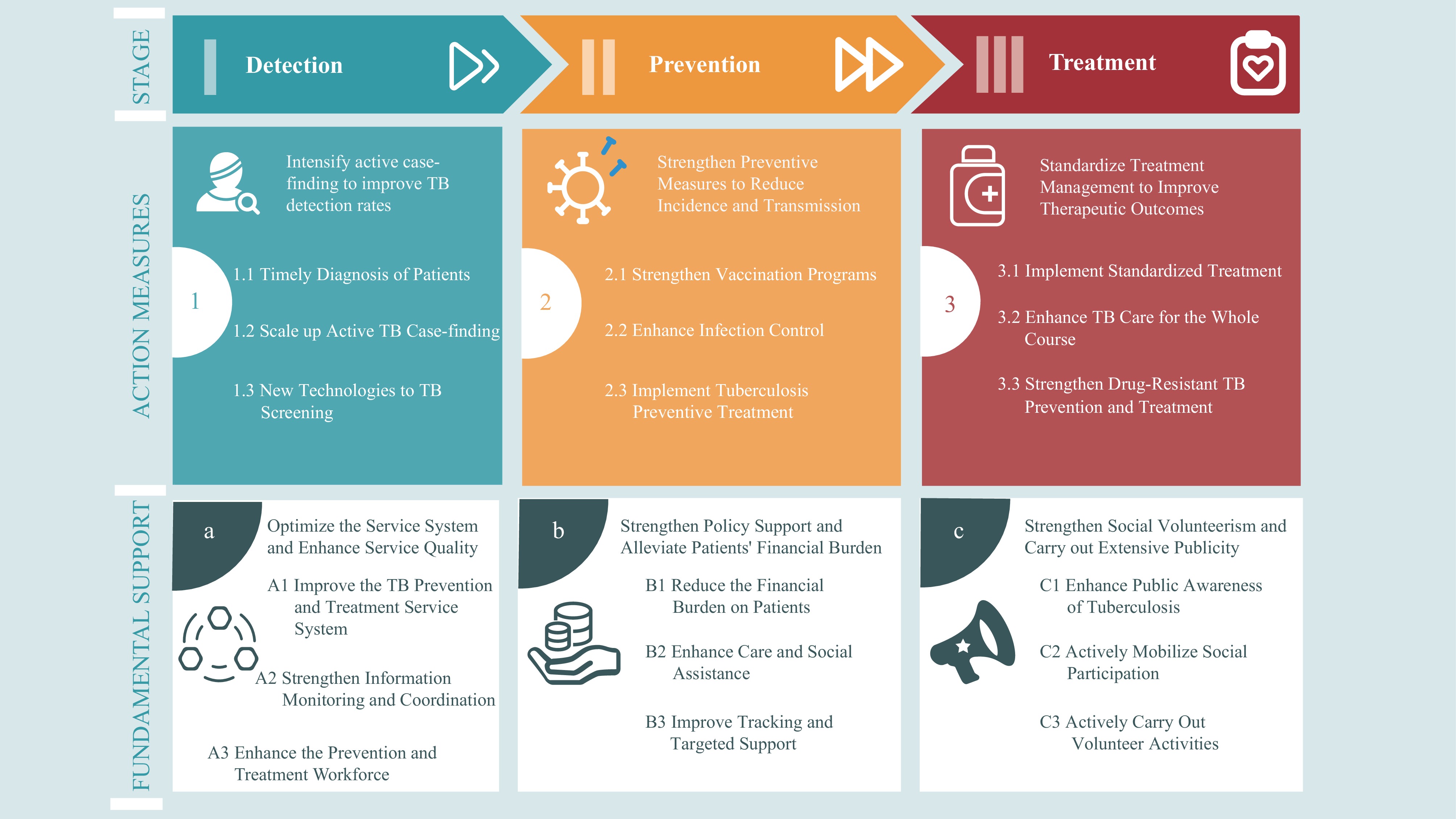 Figure 2.
Figure 2.The comprehensive TB control strategy in China.
Abbreviation: TB=tuberculosis. -
As the entry point of the full continuum of TB care, early and effective case detection is essential to reduce diagnostic delays, interrupt transmission, and enable timely treatment. From 2022 to 2024, China expanded its “Zero-TB Community initiative” pilot program from 36 to 790 sites, gradually establishing a community-based comprehensive intervention network centered on active screening and preventive treatment (7). Screening efforts prioritize key high-risk populations, such as close contacts of TB patients, HIV-infected individuals, patients with prior TB treatment, the elderly, and diabetic patients, with evidence demonstrating improved case detection in these groups. In settings with a high risk of transmission, such as schools and workplaces, mandatory screening during pre-enrollment medical examinations and annual routine checks further enhance early detection and outbreak prevention. To enhance the diagnostic capacity, designated healthcare facilities are equipped with the necessary equipment to perform molecular testing on suspected TB cases and molecular drug susceptibility testing to rapidly identify drug-resistant strains. Since 2010, the Chinese Center for Disease Control and Prevention has conducted annual evaluations of Mycobacterium tuberculosis drug-susceptibility testing capacity in laboratories of designated healthcare facilities nationwide. AI-assisted digital radiography and remote consultation systems are increasingly used in primary healthcare institutions to improve diagnostic accuracy and support healthcare providers in resource-limited areas (8). Additionally, some innovative screening modalities, such as mobile radiography vans, pooled sputum testing strategies, and emerging non-sputum molecular assays (e.g., tongue swab qPCR), are being assessed to expand the reach and efficiency of active case finding.
-
Building on enhanced case detection, China has implemented a multifaceted prevention framework to reduce TB transmission, prevent progression to active disease, and lower the overall incidence. These strategies include vaccination, infection control, preventive treatment, and zoonotic and anthroponotic TB control. Maintaining high coverage and rigorous quality control of the Bacillus Calmette–Guérin (BCG) vaccination remains fundamental. At the same time, ongoing clinical and translational research into novel vaccines, including subunit, inactivated mycobacterial, and RNA-based platforms, offers new opportunities for long-term TB prevention in China (9). Efforts are being strengthened through standardized isolation and leave policies for infected individuals, heightened awareness of personal protective measures, and targeted risk assessment and guidance at the household level, particularly among those in close contact with TB patients and among healthcare workers in high-exposure settings. Simultaneously, expanding the coverage of TB-preventive treatments (TPT) has become a key priority. This includes improving accessibility to preventive treatment clinics, optimizing screening to accurately identify eligible individuals, and enhancing diagnostic and therapeutic capacities to ensure timely initiation and adherence. Recent clinical and follow-up studies demonstrated that well-managed TPT significantly lowers the risk of progression to active disease in high-risk populations. However, barriers to acceptance and adherence remain. One study selected 10 counties/districts across five PLADs (Hebei, Henan, Hunan, Guangdong, and Chongqing) as survey sites and screened medical workers, students, teachers, and other occupational groups aged 15–65 years for LTBI between May and December 2023. The study found that the overall acceptance rate of TPT among individuals with LTBI was 17.0% (10). Therefore, China has begun to strengthen its preventive efforts through shorter rifamycin-based regimens (11), expanded policy support and financing mechanisms (12), and enhanced education and adherence support for target populations (13). In the field of prevention and control of zoonotic tuberculosis, China is strengthening source control at the national strategic level, requiring nationwide cross-departmental coordinated prevention and control efforts, and strengthening regional cooperation to achieve effective prevention and control. Together, these coordinated approaches aim to reduce infections, prevent disease progression, and block the spread of TB at the population level.
-
Standardized and patient-centered treatment management is a core priority in the TB care continuum to translate gains in detection and prevention into improved patient outcomes. This includes ensuring strict adherence to recommended regimens, implementing isolation measures for infected patients, and prioritizing fixed-dose combination therapies for drug-susceptible TB, with support from expert consultations and robust quality control systems. Comprehensive patient management should cover the entire treatment process, from screening and diagnosis to treatment and follow-up, to improve service coherence and consistency, especially in primary and rural healthcare institutions. The incorporation of digital health tools, such as electronic medication monitors and mobile health applications, has proven to significantly enhance treatment adherence and clinical outcomes, offering scalable solutions to support real-world patient management. Social support interventions, including psychological counseling and nutritional assistance, play a key role in eliminating non-medical barriers to treatment adherence and improving overall patient health. For drug-resistant TB, strengthening drug-resistance testing capacity and expanding coverage of shorter, all-oral regimens are key priorities, with emerging clinical evidence demonstrating improved patient tolerability and treatment success (14). In December 2024, the novel antituberculosis drug pretomanid was officially approved for marketing in China. This signifies the formal implementation of the WHO’s recommended 6-month all-oral short-term treatment regimen for drug-resistant TB (i.e., the BPaL/M regimen) in China. These strategies reflect a shift toward integrated patient-centered TB care aimed at achieving sustained treatment success and reducing disease transmission.
-
To sustain an effective delivery across the full continuum of care, China has focused on strengthening its underlying TB service system and improving service quality. The TB control service system is being progressively strengthened through clearer role divisions and improved coordination within an integrated healthcare network. Collaboration among the Chinese Centers for Disease Control, designated TB hospitals, and primary healthcare facilities has enhanced the effectiveness of tiered diagnosis and treatment, supporting more standardized and continuous patient management (15). Concurrently, the development and optimization of integrated information systems are improving the real-time data exchange between clinical and public health departments, enabling more efficient surveillance, earlier detection of outbreaks, and evidence-based policy adjustments. Measures to strengthen professional capacity have further solidified system performance, including high-level workforce training, structured competency development, and incentive mechanisms to improve staff motivation and retention (16). China has actively participated in the development of international technical standards and laboratory quality frameworks, thereby contributing to the advancement of global tuberculosis control practices. These measures will contribute to a more cohesive, responsive, and sustainable TB service system capable of supporting progress toward national TB goals.
-
Since economic hardship can undermine access to diagnosis, prevention, and treatment, financial protection is an indispensable component of a comprehensive TB care framework. Financial protection mechanisms for patients with TB in China are being strengthened through a multi-source financing framework that integrates infectious disease control funds, basic medical insurance schemes, local government subsidies, social assistance programs, and charitable donations (17). This diversified financing approach aims to reduce out-of-pocket expenditures and improve equitable access to healthcare services. The prices of anti-TB drugs are regulated through centralized procurement and negotiated pricing. The national essential medicine list and insurance reimbursement catalog are continuously updated to ensure the inclusion of cost-effective and clinically necessary TB drugs. To further reduce the risk of catastrophic healthcare expenditures, targeted monitoring systems are used to identify vulnerable patients, and tailored household-level support programs are implemented to prevent poverty induced by long-term treatment and loss of income. Evidence suggests that these integrated financial support strategies can effectively reduce both medical and non-medical economic burdens while improving treatment affordability and adherence among economically disadvantaged TB patients. These measures contribute to a more equitable and sustainable TB system.
-
Finally, effective implementation of the full continuum of TB care relies on strong public engagement, health communication, and broader social participation. Through multidimensional innovative health education strategies that combine traditional media and new digital communication platforms, public awareness and participation in tuberculosis prevention are constantly improving. These campaigns aim to improve TB-related health literacy among the general population, high-risk groups, and key institutions, thereby promoting timely care seeking and reducing delays in diagnosis and treatment. A nationwide cross-sectional study conducted across all PLADs during recent TB control initiatives showed gradual improvements in public knowledge, with an overall awareness rate of 82.51% for key TB information (18). However, substantial gaps remained among specific regions and population groups. Participants aged 60 and older, those with primary education or below, and students and individuals who had not received public TB education were less likely to be aware of all key TB information, underscoring the need for more targeted and practical communication strategies. Simultaneously, broad social participation is encouraged by expanding multi-sectoral collaboration and creating supportive community environments. Volunteer engagement and community health promotion activities should be encouraged to enhance individual health responsibilities, strengthen patient support networks, and maintain long-term behavioral changes. These initiatives collectively promote increased public awareness, reduce discrimination, and strengthen social participation in TB prevention and control.
-
China has made substantial progress in TB control over the past few decades through sustained political commitment, expansion of prevention and diagnostic coverage, strengthening treatment management, and continuous improvement in service delivery across the full continuum of care. These achievements demonstrate the value of combining national strategic direction with increasingly localized implementation and accountability. At the same time, the path toward ending TB in China remains challenging. Persistent disparities in surveillance, diagnostic capacity, and service quality across PLADs and between urban and rural areas have left some cases undetected or untreated, particularly among rural and remote populations (5). The expansion of TBT remains constrained by low acceptance, implementation gaps, and geographic variations, while financial protection is not uniform across all settings and population groups (10). A balanced assessment of these gaps is essential to understand both the strengths and limitations of China’s current TB control models.
To address these challenges, China has gradually developed a comprehensive TB control strategy that spans the full continuum of care, linking national strategic priorities to provincial accountability mechanisms, while continuously strengthening diagnostic and treatment capacities, improving financial protection for patients, and promoting broader public and community engagement (6). However, the effective implementation of this model depends largely on a strong governance capacity, a relatively well-developed public health network, a high degree of health system integration, and stable domestic public financing. These conditions may not be readily available in countries with fragmented healthcare systems or a long-term reliance on external aid. However, some interventions adopted in China may be more readily transferable because they are relatively low-cost and operationally feasible, including the use of AI-assisted chest radiography to support TB screening (19), scale-up of shorter all-oral regimens for drug-resistant TB (14), and the application of digital adherence support tools to improve treatment management and patient follow-up (20). These approaches are all broadly aligned with recent WHO policy updates and technical guidance and may help improve service efficiency and strengthen patient-centered care in resource-constrained settings. Overall, China’s experience should not be viewed as a one-size-fits-all solution that can be directly replicated; rather, it is better understood as a policy framework whose components can be selectively adapted according to local institutional conditions, service capacity, and fiscal space, thereby offering a practical and valuable reference for other countries seeking to strengthen TB control across the full continuum of care.
HTML
National and Provincial TB Incidence Targets in China
Comprehensive TB Control Strategy in China
Intensify Active Case-finding to Improve TB Detection Rates
Strengthen Preventive Measures to Reduce Incidence and Transmission
Standardize Treatment Management to Improve Therapeutic Outcomes
Optimize the Service System and Enhance Service Quality
Strengthen Policy Support and Alleviate Patients’ Financial Burden
Strengthen Social Volunteerism and Carry out Extensive Publicity
| Citation: |

|