
 Download:
Download:




-
Since the 2022 mpox outbreak in non-endemic countries, mpox has become a major global public health threat, prompting WHO to declare it a “Public Health Emergency of International Concern” twice (1-2). From 2 June 2023 to 30 June 2025, China reported 2,769 confirmed cases, 99% of which were attributed to MPXV clade Ⅱb, with 20 imported cases involving clades Ia and Ib (3-4). The persistent risk of clade I importation and complex MPXV mutation patterns poses sustained challenges for effective control.
Policy analysis identifies priorities and gaps in disease control. Policy tools bridge policy objectives and outcomes (5). A three-dimensional framework was developed to comprehensively analyze China’s national mpox policies, considering the policy evolution stages and policy content. A comparative analysis was conducted between these policies and the WHO’s five interdependent core components (5Cs) for the prevention and control of mpox. This analysis elucidates the characteristics of China’s mpox control policies, informing and guiding future improvements in policies addressing mpox and other emerging infectious diseases.
-
Mpox-related policies were retrieved from official websites of the National Health Commission (NHC) and National Disease Control and Prevention Administration (NDCPA), and the Peking University Law Database. The publication date range was set from 1 January 1950 to 1 July 2025. The search strategy utilized the terms: FT=(“猴痘” OR “猴痘病毒” OR “Mpox” OR “MPXV” OR “猴痘疫情” OR “monkeypox”). Overall, 175 relevant policies were initially identified. Currently effective policies excluded 3 invalid documents (replaced by updated versions were selected, with only the latest version retained for each policy type), 4 with low policy authority (e.g., draft for public comment), 31 unrelated to mpox control, and 117 not issued at the national-level. Ultimately, 20 policies were included for analysis.
Prior to conducting the three-dimensional analysis across policy instruments (X), policy objects (Y), and policy measures (Z), content analysis was performed. NVivo 15 (Lumivero, Denver, Colorado, US, version 15.0.0, August 2024) was used to code prevention and control measures. Two researchers independently coded each sentence in the policies based on semantic meaning, following the principle of non-divisibility. When discrepancies occurred between the two coders, they were resolved through expert adjudication. This process yielded 811 policy items.
-
China’s infectious disease prevention and control operates under government leadership. Based on government intervention levels, Howlett and Ramesh’s classification (6) and infectious disease-specific subdivisions (7) were adapted to define mandatory, mixed, and voluntary tools (
Supplementary Table S1 ). -
Policy objects represent implementation subjects of policy measures. The Y dimension was categorized into territorial governments, departments, institutions, and individuals, subdivided into 19 types based on responsibilities (Figure 1).
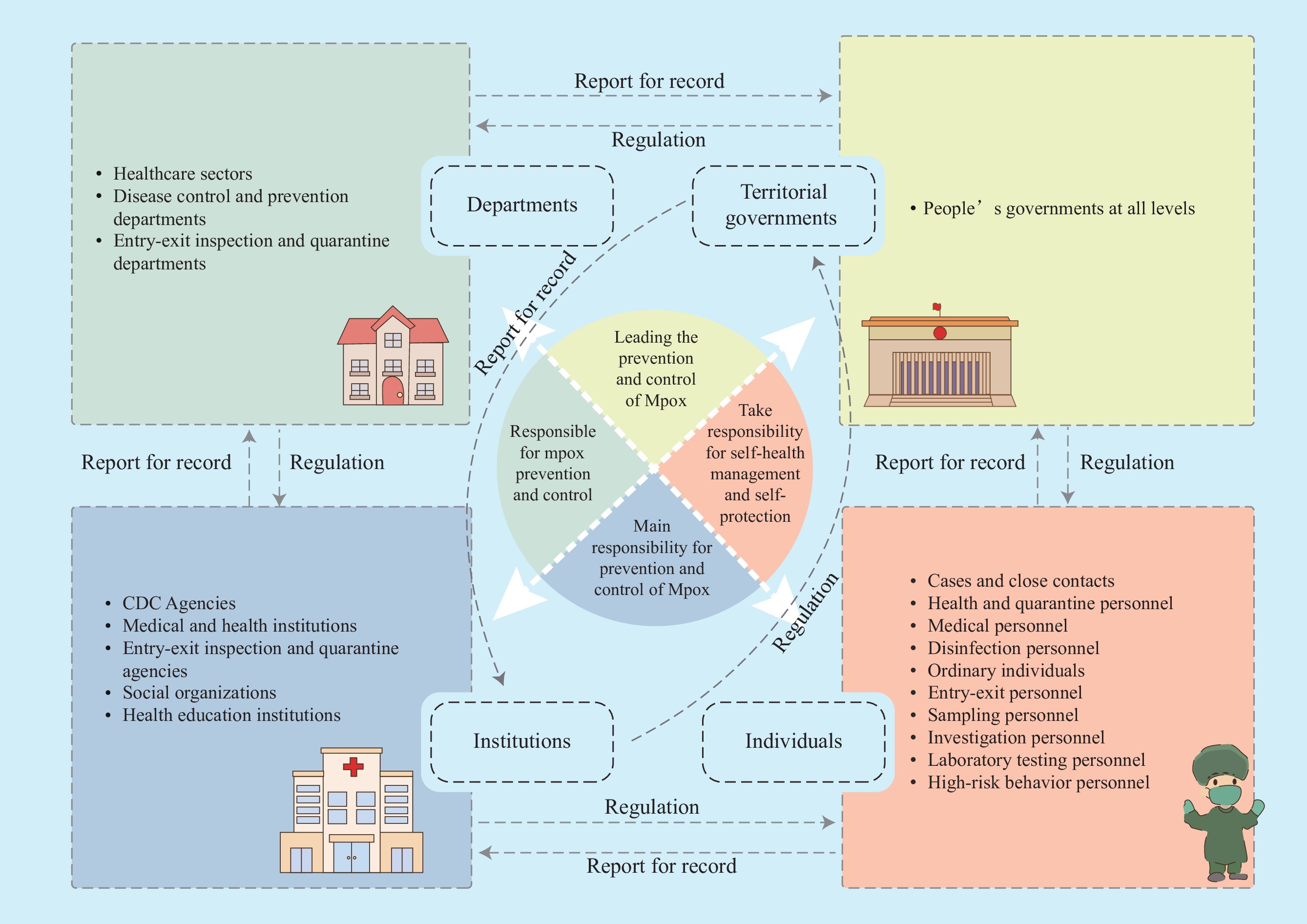 Figure 1.
Figure 1.Relationship diagram of policy objects in China’s mpox control.
Note: This figure illustrates how territorial governments, departments, institutions, and individuals constitute the four-party responsibility framework stipulated in China’s Law of the People’s Republic of China on the Prevention and Control of Infectious Diseases. These four categories correspond to the implementation subjects for mpox prevention and control measures, establishing clear divisions of labor and well-defined responsibilities. -
The infectious disease prevention and control framework, established under the Law of the People’s Republic of China on the Prevention and Control of Infectious Diseases defines primary measures encompassing disease prevention, epidemic response, medical treatment, and support measures, which are further subdivided into 19 secondary measures.
-
Four policy phases were identified: International Surveillance and Domestic Preparedness, First Imported Clade IIb Case to Local Transmission, Shift to Category B Management to the First Imported Clade Ib Case, and Preparedness for Clade Ib Outbreak, with policies released and global mpox reported cases for each phase (Figure 2).
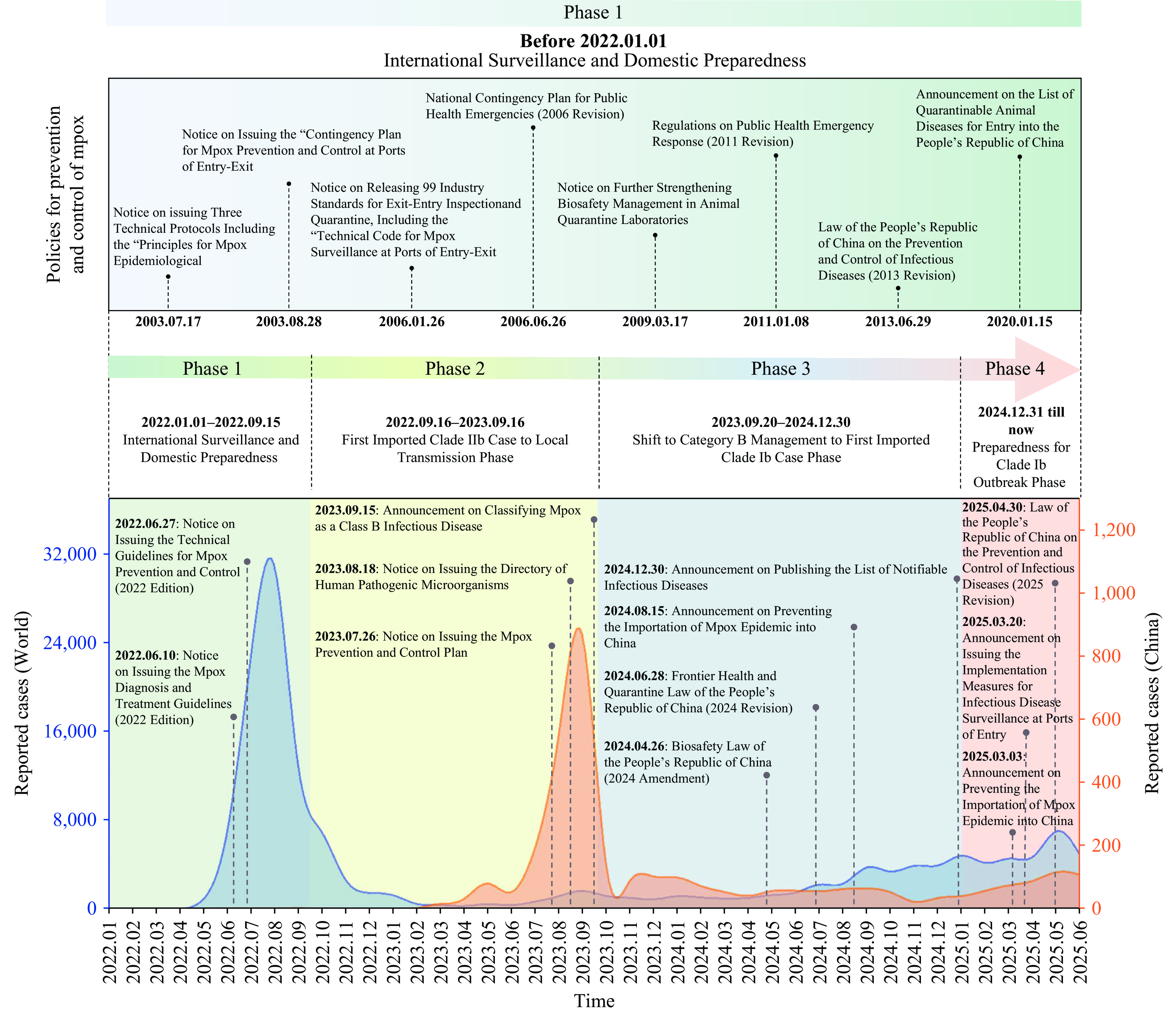 Figure 2.
Figure 2.Phased analysis of China’s mpox prevention and control policies and domestic and international reported mpox cases.
Note: Domestic and international mpox case data are sourced from the WHO website. Since WHO has not published global mpox case surveillance data prior to 1 January 2022, this figure only displays the available case trend information.
This figure presents the timeline of China’s mpox prevention and control policies alongside domestic and international reported mpox cases. The upper section displays the policy dimension, showing the evolution of China’s mpox prevention and control policies by phase.
By May 2022, nearly 12 non-endemic countries outside Africa had reported multiple MPXV infections (8). During this initial phase, China reported no cases and implemented an “external prevention of importation” strategy. China closely monitored the international epidemic while strengthening surveillance capacity, issuing 10 policies. Technical guidelines, including the “Notice on Issuing the Technical Guidelines for Mpox Prevention and Control (2022 Edition)” were developed. Entry quarantine was strengthened through the “Contingency Plan for Mpox Prevention and Control at Ports of Entry-Exit” and the “Announcement on the List of Quarantinable Animal Diseases for Entry into the People’s Republic of China.” The General Administration of Customs of China requested incoming personnel to conduct health declarations and undergo quarantine screening.
In 2022, Chongqing Municipality identified China’s first imported clade IIb mpox case (9) . Following the first domestic infection in 2023, cases were documented across 28 provinces (autonomous regions and municipalities) nationwide, primarily among men who have sex with men (MSM) (4). China adjusted its strategy to “precision prevention and control + rapid response,” improving the technical support system and issuing two policies. First, mpox was included in the “directory of human pathogenic microorganisms causing human infections” (10) . Second, medical institutions screened patients in key departments such as dermatology; disease control institutions conducted wastewater surveillance and implemented peer education; customs authorities conducted health quarantine on individuals with mpox-like symptoms. The “medical institutions — disease control institutions — customs” joint mechanism effectively controlled the epidemic spread.
China classified mpox as a legally Class B disease in September 2023. The reported cases declined thereafter, averaging 55 cases per week and decreasing to 13 cases per week in 2024. While most global outbreaks were attributed to clade IIb, clade Ib presented new challenges. Evidence indicates that clade Ib demonstrates higher fatality rates compared to clade IIb, and its genetic diversity is also 54% higher than that of clade I (11). China faces both significant importation risks and domestic transmission control pressure. Four policies were issued requiring enhanced mpox prevention and control activities, including surveillance, early warning systems, and outbreak response protocols. The revised 2024 Biosecurity Law and Frontier Health and Quarantine Law provide a legal framework for mpox prevention and control.
To address emerging and common infectious diseases, including mpox, China strengthened its infectious disease prevention infrastructure, issuing four policies. In 2025, China revised the Law of the People’s Republic of China on the Prevention and Control of Infectious Diseases, providing enhanced legal foundations for mpox prevention and control. Through accumulated expertise in surveillance, laboratory testing, and intervention measures developed across previous phases, China established robust rapid response capabilities for infectious disease outbreak management, effectively containing potential domestic epidemic transmission.
-
In policy instruments, mandatory instruments served as the primary tools. Command and authority tools predominated (41.14%, n=230). Among mixed tools, capacity-building tools were primary (46.57%, n=95), with information and persuasion tools secondary (32.35%, n=66). Voluntary tools consisted primarily of family and individual instruments (93.75%, n=45), while social organization tools were rarely employed (6.25%, n=3) (Table 1).
Dimension Disease prevention Epidemic response Medical treatment Support measures Total Mandatory 95 (17.28) 298 (53.26) 31 (5.47) 135 (23.99) 559 (68.93) Command and authority 58 (25.22) 147 (63.91) 1 (0.43) 24 (10.43) 230 (41.14) Institutions and regulations 32 (18.29) 47 (26.86) 1 (0.57) 95 (54.29) 175 (31.31) Direct provision 5 (3.57) 104 (74.82) 29 (20.86) 1 (0.72) 139 (24.87) Supervision and punishment − − − 15 (100.00) 15 (2.68) Mixed 42 (20.67) 43 (21.63) 3 (1.44) 116 (56.25) 204 (25.15) Capacity building 5 (5.26) 7 (7.37) 1 (1.05) 82 (86.32) 95 (46.57) Information and persuasion 37 (56.06) 25 (37.88) 2 (3.03) 2 (3.03) 66 (32.35) Support and subsidies − 11 (25.58) − 32 (74.42) 43 (21.08) Voluntary 18 (37.50) 30 (62.50) − − 48 (5.92) Families and individuals 15 (33.33) 30 (66.67) − − 45 (93.75) Social organizations 3 (100.00) − − − 3 (6.25) Total 155 (19.11) 371 (45.75) 34 (4.19) 251 (30.95) 811 (100.00) Note: Data in the table represent the number of codes (percentage).
“−” indicates a percentage of 0.00% (code count of 0).Table 1. Distribution of policy measures across different policy regulatory powers.
Among the four policy objects, institutions comprised the largest proportion (46.73%, n=379), followed by individuals (21.82%, n=177), departments (21.21%, n=172), and territorial governments (10.23%, n=83). At the institutional level, the disease control institutions represented the highest proportion (42.48%, n=161), while social organizations accounted for an extremely low proportion (0.79%, n=3). At the departmental level, health departments (50.58%, n=87) and disease control departments (25.00%, n=43) predominated. At the territorial level, people’s governments at all levels served as the main implementation objects. At the individual level, cases and close contacts accounted for a relatively high proportion (16.95%, n=30) (
Supplementary Table S2 ).Within policy measures, epidemic response dominated (45.75%, n=371), followed by support measures (30.95%, n=251), disease prevention (19.11%, n=155), and medical treatment (4.19%, n=34). Case detection and reporting were the primary focus of epidemic response measures (33.42%, n=124). Resource reserves and laboratory management received limited attention in support measures, each accounting for approximately 10.00%. Vaccination represented the smallest component within disease prevention (9.68%, n=15). Case transfers showed the lowest proportion among medical treatment measures (17.65%, n=6) (
Supplementary Table S3 ).Cross-dimensional analysis of X and Z revealed mandatory tools were predominantly employed in epidemic response (53.31%, n=298) and support measures (24.15%, n=135). Mixed tools comprised the largest proportion in support measures (56.86%, n=116). Voluntary tools had limited application, used exclusively for disease prevention (37.50%, n=18) and epidemic response (62.50%, n=30) (
Supplementary Table S3 ).Cross-analysis of dimensions X and Y revealed that mandatory instruments were most frequently applied to institutions (52.24%, n=292) and departments (22.00%, n=123). Mixed instruments were used across institutions, departments, individuals, and territorial governments. Voluntary instruments were predominantly directed at individuals (89.58%, n=43) (
Supplementary Table S4 ).Cross-analysis of dimensions Y and Z showed that the number of coded items at the institution level significantly exceeded those for other objects across all policy measures. Territorial governments primarily undertook support measures (73.49%, n=61). Departments and institutions were mainly responsible for epidemic response and support measures, whereas individuals were primarily involved in epidemic response (68.36%, n=121) (
Supplementary Table S3 ).Three-dimensional cross-analysis of X, Y, and Z indicated that institutions and individuals were the most frequently targeted policy objects across different policy instruments and measures. Across all policy measure categories, mandatory instruments were used more frequently than mixed or voluntary instruments (
Supplementary Table S5 ).After constructing a two-dimensional analytical framework of Y versus X/Z, it was found that the results closely resembled those from the unidimensional analysis of Y. This pattern aligns with the clearly defined “four-party responsibility” framework in China’s mpox and infectious disease control system.
-
WHO’s 5Cs (12) provide a framework for adjusting and optimizing strategies worldwide. Comparative analysis reveals that China’s mpox prevention strategies demonstrate high consistency with WHO recommendations with minor variations. The primary difference is that antiviral drugs and vaccines for mpox have not been deployed nationwide (Table 2).
WHO 5Cs WHO recommendations China’s mpox prevention and control policies Connections and differences C1: Emergency coordination
Strengthen emergency operations and foster coordination between Member States and stakeholders for responsive public health and adaptive health servicesJoint Prevention and Control Mechanism Connections: WHO recommends establishing and maintaining multi-sectoral, multi-partner coordination mechanisms at global, regional, national, and subnational levels. China’s joint prevention and control mechanism represents a successful practice aligned with WHO recommendations and adapted to national conditions. Both approaches emphasize the critical importance of multi-sectoral collaboration.
Differences: WHO recommends establishing coordination mechanisms at global, national, and regional levels. China’s coordinated prevention efforts and information sharing involve multiple departments, including disease control centers, medical institutions, customs, public security, and industry and information technology agencies, which are designed to detect and respond to mpox outbreaks promptly and enhance rapid identification capabilities for the mpox virus.C2: Collaborative surveillance (a) Surveillance, epidemiological investigation, and contact tracing
(b) Laboratories and diagnostics(a) MSM population surveillance, symptom surveillance, wastewater surveillance, infectious disease network direct reporting system, risk assessment, epidemiological investigations, and close contact screening, etc.
(b) Mpox virus nucleic acid testing, gene sequencing, and related analyses.Connections: China’s surveillance system and epidemic response measures closely align with WHO recommendations. Both China and the WHO have established multidimensional surveillance networks and emphasize the critical importance of laboratory testing and virus typing in epidemic surveillance.
Differences: WHO recommends that countries and regions strengthen surveillance and reporting mechanisms while providing essential support to diagnostic laboratories with rapid, safe, and accurate testing capabilities. This approach enables early identification of mpox cases, provision of optimal clinical care, patient isolation, contact management, protection of high-risk populations, and implementation of effective control and prevention measures. It focuses on framework measures for capacity building in countries.
China’s prevention and control efforts have become increasingly proactive and standardized. It has implemented a comprehensive multi-channel surveillance strategy through disease control centers, customs authorities, and medical institutions. This includes enhanced port quarantine measures, active surveillance of MSM populations, symptom monitoring and sewage surveillance in medical facilities, and integration of mpox into the national infectious disease network direct reporting system. Simultaneously, epidemiological investigations and nucleic acid testing are conducted for mpox cases. Gene sequencing was performed when necessary, and close contacts were traced as thoroughly as possible.C3: Community protection (a) RCCE and infodemic management
(b) Points of entry, international travel and transport, mass gatherings, and population movements
(c) Vaccination(a) Collaborate with social organizations to conduct peer education, outreach services, testing and counseling services for individuals with mpox-like symptoms, and health education at MSM key venues and social media platforms. Timely disclosing the current status of the mpox epidemic and carry out risk communication while strictly protecting the personal information of cases.
(b) Port quarantine and the establishment of information sharing mechanisms among disease control centers, medical institutions, customs, and other relevant agencies.
(c) There is currently no commercially available vaccine for mpox.Connections: Both the WHO and China recognize the importance of community interventions and health education, particularly educational and behavioral interventions targeting high-risk populations. China’s community interventions—such as peer education, outreach services, port quarantine, and entry quarantine measures—align with WHO recommendations.
Differences : WHO recommends implementing health education through established community networks and providing targeted health education and risk information for high-risk population communities and those potentially exposed to infected animals to reduce viral transmission. It is also recommended that relevant national departments develop guidelines on border measures and international travel and establish a communication mechanism between ports and health authorities, which holds significant macro-level guiding value.
China places special emphasis on collaboration between disease control centers and social organizations, focusing on raising awareness among MSM populations through comprehensive online and offline training programs. A mature information sharing mechanism has been established among the CDC, customs authorities, and hospitals. Imported mpox patients can access medical care using a convenient hospital card, which better aligns with national conditions.
The most notable difference between China and WHO lies in their vaccination strategies. WHO recommends vaccinating high-risk groups during outbreaks. Currently, China’s mpox prevention and control strategy primarily relies on non-vaccine measures. However, a live attenuated mpox vaccine has been approved for clinical trials, and several genetically engineered vaccines are currently under development (13). As mpox vaccines progress in China, this difference is expected to diminish gradually.C4: Safe and scalable care
(a) Case management and clinical operations
(b) Infection prevention and control(a) For mpox cases and close contacts, hospitalization or home isolation is implemented. No marketed mpox antiviral therapeutic drugs are available, symptomatic supportive treatment and complication treatment.
(b) Establish hospital infection control systems, ensure personal protection for medical staff at risk of occupational exposure, provide training for medical personnel, conduct pre-examination and triage in hospitals, and perform environmental disinfection, among other measures.Connections: WHO recommends case screening and isolation based on local epidemiological circumstances. WHO recommends providing optimal supportive care for mpox patients while minimizing complications wherever possible. Regarding treatment protocols, WHO advocates for the use of approved antiviral medications while continuing relevant clinical studies to evaluate drug efficacy and safety in mpox treatment. Healthcare institutions should implement infection prevention and control measures. Regarding case management-including symptomatic support, complication management, and prevention and control of nosocomial infections, China aligns with WHO recommendations and is capable of enforcing standardized isolation protocols for confirmed cases.
Differences: China aligns with WHO recommendations concerning symptomatic support and complication management strategies. The primary difference lies in therapeutic drug availability, as WHO recommends utilizing approved antiviral agents. Although several drugs are progressing through research and development and clinical trial phases, China currently lacks specific mpox medications on the market. Simultaneously, China is exploring the integration of traditional Chinese medicine into mpox patient treatment protocols.C5: Countermeasures and research
Sharing information globallySharing mpox case information with WHO and timely sharing of research findings and practical experience Connections: Both WHO and China emphasize the timely sharing of case information.
Differences: WHO advocates for timely and transparent global information sharing, including epidemiological data, research findings, and best practices, to enable countries to rapidly adjust their response strategies and reduce disease transmission. It emphasizes voluntary and transparent information exchange.
China rigorously fulfills its International Health Regulations obligations regarding mpox outbreak information sharing in accordance with WHO requirements, while actively conducting mpox-related scientific research and establishing robust epidemic reporting mechanisms to ensure timely information reporting and sharing capabilities.Abbreviation: WHO=World Health Organization; RCCE=Risk Communication and Community Engagement; MSM=men who have sex with men. Table 2. Comparison of WHO core mpox recommendations with China’s mpox prevention and control policies.
-
Policies were efficiently deployed and adapted in response to the epidemic. China’s policies prioritize surveillance and early warning, providing a legal foundation for their implementation. The successful containment of the initial clade Ib outbreak in 2024 (3), suggests the effectiveness of China’s surveillance and response systems.
Policies were formulated rapidly using scientific evidence. Following the first domestic case, the NHC developed diagnostic and technical guidelines within 8 and 25 days, respectively. A national control plan was jointly issued within one month. Regarding case and close contact management, China’s patient management measures demonstrate both precision and humanitarian care in the prevention and control strategies. Suspected and confirmed cases require transfer to medical institutions and can only undergo home isolation treatment after lesion sites have crusted over. For confirmed cases with mild symptoms who meet home isolation treatment conditions, after joint assessment by medical institutions and disease control agencies, they may directly undergo home isolation treatment with follow-up by medical personnel.
-
China’s mpox prevention and control policies are formulated by the NHC and NDCPA, implemented by customs authorities at all levels, CDCs, and medical institutions, with social organizations participating in prevention and control efforts and the entry-exit inspection and quarantine departments involved in response activities. This represents a particularly prominent feature of China’s mpox prevention and control approach.
In China, the prevention and control programs of mpox are carried out at all levels of CDCs and medical institutions. The management system and organizational structure of the unit can ensure the timely implementation of the prevention and control requirements. Although territorial policy objects are limited, this does not indicate the absence of territorial function. Its role has been reflected through cross-departmental coordination and resource allocation. Based on the existing prevention and control system of mpox, multi-sectoral collaboration and information sharing can be promoted. Individual and family policy tools can be added to clarify the responsibilities and obligations of individuals and families in mpox prevention and control.
-
China’s prevention and control policies exhibit normative force. This framework ensures both the speed and quality of prevention and control implementation, which enabled an effective response to the mpox clade Ib outbreaks since 2023 (3–4,9). However, mpox control efforts should develop intervention models grounded in trust and voluntary participation. Incorporating a varied combination of voluntary policy tools can enhance the engagement of all stakeholders, while improving both the efficiency and effectiveness of policy implementation.
China’s mpox prevention and control measures focus predominantly on epidemic response, more attention and effort are needed for disease prevention. WHO recommends vaccination for high-risk groups, a strategy adopted in several African countries. China is currently advancing vaccine research and development initiatives. Moving forward, China should accelerate vaccine development or import a vaccine (14) to improve preparedness.
Non-endemic regions such as the Americas have experienced outbreaks closely associated with high-risk sexual behaviors, primarily transmitted through male-to-male contact among MSM populations. Targeted education and self-protection awareness for high-risk groups are essential. Social organizations play a crucial role in mpox prevention and control (14). These organizations can access MSM activity venues to promote testing initiatives and facilitate the detection of additional positive cases (15). Future strategies should incorporate voluntary policy tools to enhance social organization participation in mpox prevention and control (16). Future policy should integrate specific goals and scenarios for mpox prevention and control, clearly define the conditions under which mandatory measures are warranted, ensure the effective application of mandatory tools, and continue to enhance the use of mixed tools to improve the efficiency of mpox prevention and control.
China’s mpox policies align closely with epidemic trends, emphasize multi-sector coordination, including CDCs, medical institutions, and customs authorities, and are consistent with WHO recommendations, enabling early detection, reporting, isolation, and treatment. These policies exhibit robust normative force and prioritize comprehensive epidemic response capabilities. Future efforts should optimize vaccine strategies and social mobilization to enhance public health resilience.
-
All staff involved in policy coding and analytical functions for their contributions.
HTML
X: Policy Instruments
Y: Policy Objects
Z: Policy Measures
Overview of the Mpox Epidemic and Policy Evolution Phases
Analysis Results of Policies Content
Comparison of China’s Mpox Prevention and Control Policies with WHO Core Recommendations
Policy Deployment Demonstrates Efficiency and Epidemic-responsive Adaptation
Prevention and Control Policies Highlight Multi-departmental Coordination
The Policies Demonstrate Normative Force, Though Prevention and Control Measures Require Better Balance
| Citation: |

|