
 Download:
Download:




-
Introduction: Anemia represents a major health burden among women globally and poses a critical challenge to achieving international targets for reducing anemia prevalence in women of reproductive age and eliminating malnutrition by 2030. Despite its public health significance, temporal trends in anemia prevalence among Chinese women remain inadequately characterized.
Methods: This study analyzed health examination data from 231 prefecture-level cities across all 31 provincial-level administrative divisions in China, encompassing 16,700,713 women examined in 2019 (n=7,822,489) and 2024 (n=8,878,224). Standardized prevalence estimates with 95% confidence intervals (CIs) were calculated by adjusting for provincial population structures. Temporal changes were quantified using prevalence differences with corresponding 95% CIs. Multivariable logistic regression models incorporating time-by-covariate interaction terms were employed to identify factors associated with anemia and moderate-to-severe anemia and to assess time-varying associations.
Results: Between 2019 and 2024, the overall prevalence of anemia among urban women and women of reproductive age in China declined from 13.7% (95% CI: 13.0, 14.4) and 17.0% (95% CI: 16.3, 17.8) to 13.2% (95% CI: 12.7, 13.8) and 16.7% (95% CI: 16.1, 17.3), respectively, while moderate-to-severe anemia prevalence remained essentially unchanged. Among women aged 40–49 years, anemia prevalence increased modestly, with a statistically significant rise in moderate-to-severe anemia of 0.32 percentage points (95% CI: 0.06, 0.57). Substantial regional disparities persisted: anemia prevalence decreased in 18 provincial units but increased in the remaining 13 units. Among women of reproductive age, anemia prevalence rose in 14 provincial units, with three provinces reaching or exceeding the 20% threshold indicative of moderate public health burden.
Conclusion: Although China has achieved modest progress in reducing anemia among women, the overall disease burden remains substantial, with persistently elevated or increasing prevalence observed in specific subpopulations. These findings underscore the urgent need for targeted, risk-stratified public health interventions that prioritize women aged 40–49 years and provinces where anemia prevalence has increased or exceeds 20%.
-
Anemia poses a widespread threat to the health of women and their offspring while also diminishing productivity and imposing substantial economic and social burdens (1). Recognizing this critical public health challenge, the United Nations Sustainable Development Goals (SDGs) have prioritized the reduction of maternal anemia. China has actively embraced this initiative by incorporating maternal anemia prevention and control into its national strategic planning. Continuous monitoring of anemia prevalence and its associated risk factors is essential for policymakers to develop and refine targeted intervention strategies. However, existing studies have predominantly examined anemia prevalence among Chinese women or pregnant women within specific years or geographic regions, leaving significant gaps in our understanding of temporal trends across the broader female population (2–5). To address this knowledge gap, the present study compares anemia prevalence and associated factors among urban women in China between 2019 and 2024, thereby characterizing temporal patterns and informing evidence-based public health responses.
Data for this study were obtained from Meinian Healthcare Group, China's largest health examination chain, with service networks spanning 231 prefecture-level cities across all 31 provincial-level administrative divisions (PLADs) (6). We extracted records from non-pregnant women aged 18 years or older who underwent physical examinations during two distinct periods: January 1 to December 31, 2019, and January 1 to December 31, 2024. The final dataset comprised 16,700,713 participants, including 7,822,489 examined in 2019 and 8,878,224 in 2024. Study participants were predominantly urban residents, including employed individuals and other city dwellers.
Demographic information, physical measurements, and laboratory tests were collected using standardized protocols and calibrated instruments across all examination centers. Following World Health Organization (WHO) criteria, anemia was defined as hemoglobin concentration <120.0 g/L (7). Anemia severity was further categorized as mild (110.0–119.0 g/L), moderate (80.0–109.0 g/L), or severe (<80.0 g/L). Hemoglobin concentrations were measured using automated hematology analyzers, with altitude-adjusted thresholds applied to specific prefecture-level cities according to WHO recommendations. For analytical purposes, the study population was stratified into six geographic regions: North (Beijing, Tianjin, Hebei, Shanxi, Inner Mongolia), East (Anhui, Jiangxi, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong), Central (Henan, Hubei, Hunan, Guangxi, Guangdong, Hainan), Southwest (Chongqing, Sichuan, Guizhou, Yunnan, Tibet), Northwest (Shaanxi, Gansu, Qinghai, Ningxia, Xinjiang), and Northeast China (Liaoning, Jilin, Heilongjiang).
To account for demographic structure and enable valid temporal comparisons, prevalence estimates and 95% confidence intervals (CIs) were standardized to the population distribution reported in China's Seventh National Population Census (2020), which represents the most recent comprehensive demographic benchmark. Differences in categorical variables were assessed using the χ2 test with Rao-Scott correction for complex survey design. Temporal changes were quantified using prevalence differences with corresponding 95% CIs for both overall anemia and moderate-to-severe anemia. We employed multivariable logistic regression models to identify risk factors associated with anemia and moderate-to-severe anemia, adjusting for age, body mass index (BMI), history of cesarean delivery, geographic region, per capita gross domestic product (GDP), Engel coefficient, hypertension, total cholesterol, triglycerides, hyperuricemia, diabetes, and impaired kidney function. To address the hierarchical data structure, models incorporated random intercepts at the city-level to account for within-city correlation. Furthermore, we constructed pooled models combining data from both years and included “Year×Covariate” interaction terms to investigate temporal changes in risk factor associations. A statistically significant interaction (P for interaction < 0.05) indicated that the strength of association for a given risk factor differed between 2019 and 2024. All statistical analyses were performed using SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA), with a two-sided P<0.05 threshold for statistical significance.
Table 1 presents the prevalence of anemia and moderate-to-severe anemia among urban women in China during 2019–2024. Overall anemia prevalence among urban women declined from 13.7% in 2019 to 13.2% in 2024, while moderate-to-severe anemia decreased slightly from 5.1% to 5.0%. Among women of reproductive age, anemia prevalence fell from 17.0% to 16.7%. However, none of these reductions achieved statistical significance.
Variable 2019 2024 Prevalence difference for anemia
(%, 95% CI)Prevalence difference2
for moderate-severe anemia
(%, 95% CI)Number (%) Anemia
(%, 95% CI)Moderate-severe anemia
(%, 95% CI)Number (%) Anemia
(%, 95% CI)Moderate-severe anemia
(%, 95% CI)Overall 7,822,489
(100.0)13.7
(13.0, 14.4)5.1
(4.8, 5.4)8,878,224
(100.0)13.2
(12.7, 13.8)5.0
(4.8, 5.3)−0.49
(−1.03, 0.06)−0.06
(−0.23, 0.11)Age group (years) 18–29 1,577,832
(20.2)11.9
(11.1, 12.6)3.9
(3.6, 4.2)1,521,094
(17.1)11.8
(11.2, 12.4)4.1
(3.9, 4.3)−0.08
(−0.75, 0.60)0.18
(−0.02, 0.38)30–39 2,132,587
(27.3)16.8
(16.0, 17.6)6.6
(6.3, 7.0)2,634,552
(29.7)15.9
(15.3, 16.6)6.5
(6.2, 6.8)−0.84
(−1.47, −0.20)*−0.15
(−0.39, 0.08)40–49 1,732,054
(22.1)19.5
(18.7, 20.3)9.3
(8.9, 9.8)1,932,893
(21.8)19.6
(18.9, 20.4)9.7
(9.2, 10.1)0.15
(−0.41, 0.71)0.32
(0.06, 0.57)*50–59 1,497,049
(19.1)9.5
(8.9, 10.0)3.1
(2.9, 3.3)1,657,106
(18.7)8.9
(8.5, 9.4)2.8
(2.7, 3.0)−0.56
(−0.99, −0.14)*−0.25
(−0.36, −0.13)*60–69 677,413
(8.7)8.4
(7.7, 9.1)1.6
(1.4, 1.7)837,762
(9.4)7.6
(7.1, 8.2)1.4
(1.2, 1.6)−0.76
(−1.35, −0.17)*−0.17
(−0.32, −0.02)*70+ 205,554
(2.6)14.3
(13.3, 15.3)**3.8
(3.4, 4.2)**294,817
(3.3)13.4
(12.4, 14.4)**3.5
(3.0, 4.0)**−0.94
(−2.12, 0.25)−0.31
(−0.87, 0.25)Age group 2 (years) 18–49 5,442,473
(69.6)17.0
(16.3, 17.8)7.2
(6.9, 7.6)6,088,539
(68.6)16.7
(16.1, 17.3)7.3
(7.0, 7.7)−0.31
(−0.89, 0.26)0.09
(−0.12, 0.30)50+ 2,380,016
(30.4)10.0
(9.4, 10.7)**2.7
(2.5, 2.9)**2,789,685
(31.4)9.3
(8.8, 9.9)**2.5
(2.3, 2.7)**−0.70
(−1.29, −0.10)*−0.23
(−0.41, −0.05)*BMI Underweight 439,078
(5.6)16.6
(15.7, 17.5)5.5
(5.1, 5.8)433,134
(4.9)17.0
(16.2, 17.7)5.7
(5.5, 6.0)0.34
(−0.40, 1.09)0.27
(0.03, 0.52)*Normal 4,535,052
(58.0)15.5
(14.7, 16.3)5.7
(5.4, 6.0)4,970,298
(56.0)14.9
(14.3, 15.5)5.6
(5.3, 5.9)−0.60
(−1.20, 0.00)−0.11
(−0.30, 0.08)Overweight 2,168,776
(27.7)11.7
(11.1, 12.2)4.4
(4.2, 4.7)2,582,885
(29.1)11.3
(10.8, 11.8)4.4
(4.2, 4.6)−0.36
(−0.85, 0.12)−0.03
(−0.19, 0.13)Obesity 679,583
(8.7)9.6
(9.2, 10.1)**3.8
(3.6, 4.0)**891,907
(10.0)9.9
(9.5, 10.3)**4.1
(3.9, 4.3)**0.25
(−0.21, 0.70)0.27
(0.10, 0.44)*History of cesarean delivery Yes 321,881
(4.1)17.0
(15.8, 18.3)7.2
(6.6, 7.8)1,116,428
(12.6)16.3
(15.5, 17.0)7.3
(6.9, 7.7)−0.78
(−1.96, 0.41)0.11
(−0.40, 0.63)No 7,500,608
(95.9)13.6
(12.9, 14.2)**5.0
(4.8, 5.3)**7,761,796
(87.4)12.9
(12.3, 13.4)**4.8
(4.5, 5.0)**−0.73
(−1.25, −0.20)*−0.25
(−0.41, −0.09)*Per capita GDP Lowest 2,010,724
(25.7)14.0
(13.2, 14.9)5.3
(5.0, 5.6)2,021,530
(22.8)13.7
(12.9, 14.5)5.4
(5.0, 5.7)−0.32
(−1.16, 0.52)0.08
(−0.22, 0.38)Up to median 2,156,418
(27.6)13.0
(11.7, 14.2)4.9
(4.4, 5.4)2,025,231
(22.8)12.7
(11.7, 13.7)5.0
(4.5, 5.4)−0.30
(−1.19, 0.59)0.08
(−0.20, 0.36)Above median 1,805,148
(23.1)14.2
(12.6, 15.9)5.2
(4.5, 5.9)2,068,072
(23.3)12.7
(11.7, 13.8)4.8
(4.3, 5.3)−1.51
(−3.04, 0.02)−0.40
(−0.83, 0.02)Highest 1,850,199
(23.7)13.9
(12.5, 15.4)5.1
(4.5, 5.6)2,763,391
(31.1)13.9
(12.5, 15.3)5.0
(4.5, 5.5)−0.04
(−1.03, 0.94)−0.12
(−0.44, 0.20)Engel coefficient Highest 2,341,106
(29.9)13.8
(12.7, 14.9)4.9
(4.5, 5.3)2,504,518
(28.2)13.5
(12.4, 14.5)4.9
(4.5, 5.4)−0.35
(−1.24, 0.54)0.06
(−0.25, 0.36)Above median 1,608,892
(20.6)13.8
(12.0, 15.6)5.0
(4.2, 5.8)1,843,720
(20.8)13.2
(12.0, 14.3)4.9
(4.3, 5.4)−0.60
(−1.69, 0.49)−0.16
(−0.50, 0.18)Up to median 2,026,962
(25.9)13.9
(12.7, 15.2)5.3
(4.9, 5.7)2,292,146
(25.8)13.3
(12.4, 14.2)5.2
(4.8, 5.6)−0.65
(−1.62, 0.31)−0.08
(−0.36, 0.21)Lowest 1,845,529
(23.6)13.2
(12.1, 14.3)5.3
(4.9, 5.8)2,237,840
(25.2)12.8
(11.7, 13.9)5.3
(4.7, 5.8)−0.42
(−1.97, 1.12)−0.08
(−0.55, 0.39)Geographic region North 857,401
(11.0)11.9
(10.8, 13.0)5.1
(4.7, 5.5)1,474,737
(16.6)12.7
(11.4, 14.0)5.3
(4.7, 6.0)0.81
(−0.65, 2.28)0.26
(−0.26, 0.77)East 2,748,022
(35.1)13.7
(12.7, 14.7)5.1
(4.8, 5.5)3,133,161
(35.3)13.7
(13.0, 14.4)5.1
(4.8, 5.4)−0.02
(−0.86, 0.82)0.03
(−0.21, 0.26)Central 2,031,347
(26.0)16.1
(14.8, 17.4)5.8
(5.3, 6.3)2,254,437
(25.4)15.0
(14.1, 15.9)5.6
(5.2, 5.9)−1.11
(−2.39, 0.18)−0.23
(−0.65, 0.18)Southwest 1,001,486
(12.8)11.3
(10.1, 12.5)3.8
(3.4, 4.2)794,601
(9.0)10.6
(9.5, 11.6)3.7
(3.3, 4.0)−0.75
(−1.71, 0.20)−0.13
(−0.38, 0.12)Northwest 443,920
(5.7)14.1
(12.0, 16.2)6.0
(5.3, 6.6)448,662
(5.1)12.9
(11.7, 14.0)5.8
(5.4, 6.2)−1.23
(−3.01, 0.55)−0.16
(−0.77, 0.45)Northeast 740,313
(9.5)11.7
(11.0, 12.4)**4.1
(3.7, 4.4)**772,626
(8.7)10.4
(9.7, 11.2)**4.0
(3.8, 4.2)**−1.23
(−2.35, −0.12)*−0.07
(−0.54, 0.37)Note: The prevalence difference and P represent comparisons for the overall anemia rate.
Abbreviation: CI=confidence interval; GDP=gross domestic product; BMI=body mass index.
* P<0.05;
** P<0.01.Table 1. Prevalence of anemia by severity among urban women in China, 2019 versus 2024.
Age-stratified analysis revealed significant disparities in anemia prevalence and severity across age groups. Between 2019 and 2024, anemia prevalence decreased in all age groups except women aged 40–49 years, who experienced a slight increase. The reductions were particularly pronounced and statistically significant in the 30–39 and 50–69 age groups. For moderate-to-severe anemia, prevalence among women aged 40–49 years increased significantly over the five-year period [odds ratio (OR)=0.32, 95% CI: 0.06, 0.57], whereas prevalence among women aged 50–59 and 60–69 years decreased significantly (OR=−0.25, 95% CI: −0.36, −0.13; OR=−0.17, 95% CI: −0.32, −0.02).
Regional analysis revealed statistically significant differences in both overall anemia and moderate-to-severe anemia prevalence among Chinese urban women in both 2019 and 2024. Notably, only women in Northeast China demonstrated a significant decline in anemia prevalence during this period. Figure 1 provides detailed provincial-level data. Among all age groups, anemia prevalence decreased in 18 provincial-level administrative divisions (PLADs) while increasing in 13 PLADs, including Hebei, Guizhou, and Tibet. Among women of reproductive age specifically, 17 PLADs experienced declining prevalence whereas 14 PLADs showed increases, with Tibet, Shandong, and Hebei reaching the 20% threshold.
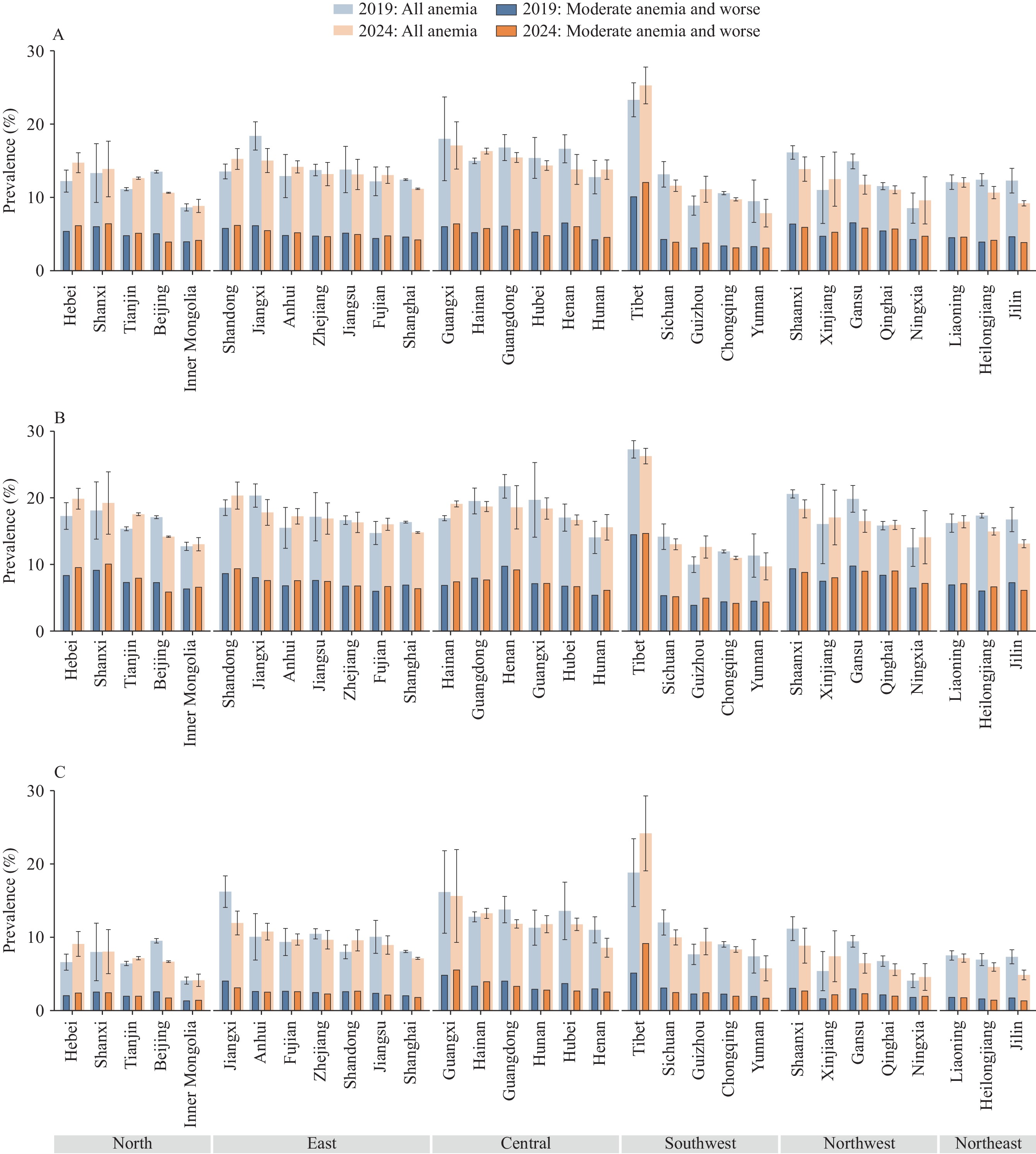 Figure 1.
Figure 1.Regional disparities in the prevalence of anemia among urban women in China, standardized by age, 2019 versus 2024. (A) Anemia among all urban women; (B) Anemia among urban women aged 18–49 years; (C) Anemia among urban women aged 50 years and over.
Multivariate analysis identified several factors significantly associated with anemia and moderate-to-severe anemia risk among Chinese urban women (Table 2). Relative to women aged 18–29 years, all other age groups except those aged 60–69 years demonstrated significantly elevated anemia risk. Age-year interaction analysis, however, revealed a significant temporal decline in anemia and moderate-to-severe anemia risk across all age groups except women aged 40–49 years (interaction OR=0.99, 95% CI: 0.99, 1.01). Underweight women exhibited significantly increased anemia risk that intensified over time, whereas obese women showed significantly reduced risk (OR=0.80, 95% CI: 0.78, 0.82), with this protective effect strengthening over time (OR=1.01, 95% CI: 1.00, 1.01). A history of cesarean section was associated with elevated anemia risk (OR=1.07, 95% CI: 1.04, 1.10), and this association with moderate-to-severe anemia strengthened over time (OR=1.02, 95% CI: 1.00, 1.03). Women residing in areas with the lowest per capita GDP demonstrated significantly higher anemia risk compared to those in the highest GDP areas (OR=1.15, 95% CI: 1.03, 1.28), though this association remained stable over time.
Variable Anemia Moderate-severe anemia Overall OR
(95% CI)Interaction OR
(95% CI)P for interaction Overall OR
(95% CI)Interaction OR
(95% CI)P for interaction Year 2019 Reference — — Reference — — 2024 0.98
(0.93, 1.02)— — 1.01
(0.97, 1.05)— — Age group (years) 18–29 Reference Reference — Reference Reference — 30–39 1.52
(1.48, 1.56)**0.987
(0.980, 0.995)<0.001 1.71
(1.66, 1.76)**0.984
(0.978, 0.991)<0.001 40–49 2.16
(2.11, 2.22)**0.999
(0.991, 1.008)0.908 2.88
(2.79, 2.97)**0.994
(0.987, 1.002)0.159 50–59 1.09
(1.04, 1.14)**0.982
(0.973, 0.990)<0.001 1.01
(0.97, 1.06)0.969
(0.961, 0.977)<0.001 60–69 1.01
(0.94, 1.09)0.923
(0.961, 0.985)<0.001 0.53
(0.47, 0.59)**0.961
(0.943, 0.980)<0.001 70+ 1.76
(1.64, 1.88)**0.979
(0.962, 0.995)0.013 1.15
(1.02, 1.30)*0.969
(0.940, 0.998)0.038 BMI Underweight 1.12
(1.10, 1.15)**1.015
(1.010, 1.020)<0.001 1.02
(0.99, 1.04)1.013
(1.006, 1.021)<0.001 Normal Reference Reference — Reference Reference — Overweight 0.86
(0.85, 0.87)**0.998
(0.995, 1.001)0.205 0.97
(0.96, 0.99)**0.998
(0.994, 1.001)0.156 Obesity 0.80
(0.78, 0.82)**1.009
(1.004, 1.014)<0.001 0.98
(0.96, 1.01)1.007
(1.002, 1.013)0.010 History of cesarean delivery Yes 1.07
(1.04, 1.10)**1.006
(0.993, 1.020)0.349 1.10
(1.07, 1.14)**1.015
(1.003, 1.027)0.015 No Reference Reference — Reference Reference — Per capita GDP Lowest 1.15
(1.03, 1.28)*0.998
(0.976, 1.020)0.856 1.20
(1.08, 1.34)**1.011
(0.991, 1.030)0.284 Up to median 1.05
(0.95, 1.17)0.995
(0.972, 1.018)0.680 1.10
(1.00, 1.22)*1.007
(0.988, 1.026)0.468 Above median 1.08
(0.95, 1.22)0.976
(0.947, 1.006)0.121 1.13
(1.00, 1.27)*0.987
(0.966, 1.009)0.258 Highest Reference Reference — Reference Reference — Engel coefficient Highest 1.08
(0.99, 1.17)1.005
(0.974, 1.037)0.755 0.97
(0.89, 1.06)1.011
(0.988, 1.035)0.350 Above median 1.05
(0.94, 1.17)0.999
(0.966, 1.033)0.968 0.95
(0.86, 1.05)0.999
(0.976, 1.024)0.958 Up to median 1.07
(0.97, 1.19)1.004
(0.972, 1.037)0.828 0.99
(0.90, 1.09)1.009
(0.987, 1.032)0.432 Lowest Reference Reference — Reference Reference — Geographic region North 1.13
(1.01, 1.27)*1.035
(0.999, 1.072)0.056 1.21
(1.09, 1.35)**1.007
(0.973, 1.042)0.696 East 1.25
(1.15, 1.35)**1.024
(0.998, 1.050)0.075 1.23
(1.15, 1.31)**1.001
(0.974, 1.029)0.934 Central 1.41
(1.29, 1.55)**1.005
(0.976, 1.036)0.728 1.35
(1.24, 1.46)**0.991
(0.960, 1.022)0.563 Southwest 0.90
(0.81, 1.01)1.007
(0.978, 1.036)0.654 0.83
(0.76, 0.91)**0.990
(0.961, 1.020)0.506 Northwest 1.10
(0.95, 1.28)0.998
(0.962, 1.035)0.914 1.26
(1.13, 1.40)**0.991
(0.958, 1.025)0.585 Northeast Reference Reference — Reference Reference — Note: “—” means not applicable.
Abbreviation: OR=odds ratio; CI=confidence interval; GDP=gross domestic product; BMI=body mass index.
* P<0.05;
** P<0.01.Table 2. Multilevel logistic regression analysis of factors associated with anemia among urban women in China: Overall effects and interactions with year (2019 versus 2024).
-
Although anemia among women remains a major public health concern, comprehensive data on the prevalence, severity, and temporal trends of anemia among Chinese women have been limited. To address this gap, the present study leveraged national-level health examination data to characterize recent changes in anemia prevalence and its associated risk factors. Our findings provide a detailed portrait of anemia burden among urban women at both provincial and national levels, revealing substantial temporal, demographic, and regional heterogeneity. These results offer robust scientific evidence to inform the identification of high-risk subpopulations and the development of targeted, stratified anemia prevention and control strategies.
The WHO classifies anemia prevalence below 20% as a mild public health burden, 20%–40% as moderate, and above 40% as severe (7). By this criterion, the overall anemia burden among Chinese urban women remains mild. While the latest WHO global anemia assessment report indicates a stagnation in progress toward reducing anemia among women of reproductive age worldwide, anemia prevalence among urban Chinese women of reproductive age declined from 2019 to 2024, with decreases observed in most PLADs. This trend demonstrates that China has achieved measurable progress in maternal anemia prevention and control, likely attributable to the implementation of national nutrition and health policies. These include the Healthy China Initiative (2019–2030), which explicitly outlines targeted actions for rational dietary practices, and the National Nutrition Plan (2017–2030), which establishes specific goals for reducing population anemia prevalence (8–9). Nevertheless, anemia prevalence among urban women has risen over the past five years in several provinces, with prevalence reaching or exceeding the 20% threshold in Tibet, Shandong, and Hebei—indicating a moderate disease burden in these regions that warrants heightened public health attention.
This study confirmed age as an independent risk factor for anemia, consistent with previous findings. Although overall anemia prevalence did not differ significantly between 2019 and 2024, age-year interaction effects revealed substantial heterogeneity in temporal risk patterns across age groups. Anemia risk decreased significantly over time among women aged 30–39, 50–59, 60–69, and 70+ years, while remaining stable in the 40–49 age group. This distinctive pattern likely reflects the higher susceptibility to abnormal uterine bleeding in women aged 40–49 years — often attributable to conditions such as uterine fibroids and perimenopausal endocrine disorders (10–12). These findings underscore the need for age-differentiated anemia prevention and control strategies, with particular emphasis on strengthening health management for women aged 40–49 years to further reduce the overall anemia burden.
Women with a history of cesarean section demonstrated a significantly elevated anemia risk, consistent with previous research (2). This association likely stems from both greater perinatal blood loss and increased risk of uterine impairment associated with cesarean delivery, either of which can substantially increase anemia susceptibility (13–14). Moreover, this study revealed that the association between cesarean section history and anemia risk strengthened significantly over time. These findings highlight the importance of increasing clinical awareness of cesarean section history as an anemia risk factor and reducing unnecessary cesarean deliveries.
This study has several limitations. First, the cross-sectional design precludes definitive causal inferences regarding factors contributing to anemia in women. Second, due to practical constraints on data processing timelines, this study compared anemia prevalence at only two discrete time points, failing to capture potential fluctuations during the intervening period—a limitation that may affect the precision of temporal trend assessments. Third, although automated hematology analyzers were used to measure hemoglobin levels at all examination centers with standardized calibration protocols, variations in specific instrument models and testing reagents across sites may have introduced measurement variability.
In conclusion, China has made measurable progress in maternal anemia prevention and control, yet substantial disease burden persists in certain provinces and population subgroups. Targeted and risk-stratified public health interventions are warranted, with priority given to women aged 40–49 years, women with a history of cesarean section, and provinces where anemia prevalence has increased or exceeded 20%.
-
Approval by the Peking University Institutional Review Board (IRB-0000152-19077).
HTML
| Citation: |

|