
 Download:
Download:




-
Introduction: The influence of serum ferritin on gestational diabetes mellitus (GDM) development remains unclear. This study evaluated associations between longitudinal serum ferritin measurements in the first and second trimesters and GDM risk.
Methods: This multicenter, prospective cohort study enrolled participants from four hospitals across Beijing Municipality, and Shanxi and Shandong provinces in China between July 2021 and June 2024. Participants were stratified into tertiles based on serum ferritin concentrations measured at 11–13, 16–19, and 24–27 weeks’ gestation. Poisson regression and restricted cubic spline models were employed to examine associations between serum ferritin and GDM.
Results: Among 6,614 participants, 1,427 (21.6%) developed GDM. At 11–13 weeks’ gestation, a U-shaped relationship between serum ferritin and GDM was identified (Pnon-linear=0.008), demonstrating that both the lowest [risk ratio (RR): 1.31; 95% confidence interval (CI): 1.05, 1.63] and highest tertiles (RR: 1.33; 95% CI: 1.07, 1.66) were associated with elevated GDM risk after adjusting for demographic, socioeconomic, and clinical confounders. Women in the highest tertile of serum ferritin at 16–19 weeks’ (RR: 1.28; 95% CI: 1.03, 1.58) and 24–27 weeks’ gestation (RR: 1.18; 95% CI: 1.03, 1.35) had significantly greater GDM risk compared with the medium tertile.
Conclusion: Serum ferritin concentrations in the first and second trimesters were independently associated with GDM risk. Enhanced strategies are needed to improve understanding and clinical utility of serum ferritin measurements for early identification and prevention of GDM.
-
Gestational diabetes mellitus (GDM) has emerged as a major health concern during pregnancy worldwide. The prevalence of GDM has increased steadily over recent decades; by 2024, its global prevalence was estimated at 15.6%, with China reporting 15.7% (1). In the short term, GDM contributes to numerous adverse pregnancy complications and outcomes, including preeclampsia, cesarean delivery, shoulder dystocia, macrosomia, and neonatal hypoglycemia. Long-term consequences extend to both mothers and offspring, who face elevated risks of obesity, type 2 diabetes, and cardiovascular disease later in life (2).
Iron serves as an essential trace element for various life-sustaining processes, including hematopoiesis, oxygen transport, cell proliferation, and iron deficiency (3). Iron deficiency affects an estimated 45% of pregnant women in well-resourced countries and 80% in low- and middle-income countries, increasing the risk of adverse maternal and neonatal outcomes such as anemia, gestational hypertension, preterm birth, and low birth weight (3–4). Conversely, accumulating evidence indicates that elevated iron storage is associated with enhanced insulin resistance, reduced insulin secretion, and higher risk of type 2 diabetes in non-pregnant populations (3). However, the influence of iron storage across different trimesters on GDM occurrence remains unclear. Ferritin is widely recognized as the primary indicator of iron status in epidemiological studies, as it represents the stable storage form of iron in humans. Therefore, this study aimed to prospectively evaluate the magnitude and shape of associations between serum ferritin levels in the first and second trimesters and GDM risk.
This multicenter, prospective cohort study was conducted at four hospitals across Beijing Municipality, Shanxi Province, and Shandong Province in China between July 2021 and June 2024. Women at 11–13 weeks of gestation receiving antenatal care at these four hospitals were enrolled. Inclusion criteria required participants to be aged ≥18 years and to intend to receive routine antenatal care and delivery at the study hospitals. Exclusion criteria included severe chronic diseases and/or serious mental illnesses before pregnancy. The study was approved by the institutional review board of Peking University First Hospital, and all participants provided written informed consent. At enrollment, a well-trained investigator conducted a face-to-face interview with each participant using a structured questionnaire to collect demographic characteristics, lifestyle behaviors, and medical and obstetric history. Participants were followed up at 16–19, 24–27, 32–35, and 36–40 weeks of gestation. A total of 8,091 pregnant women were recruited. After excluding women diagnosed with anemia (n=319), diabetes (n=49), or hypertension before pregnancy (n=38); those with twin or multiple pregnancies (n=36); those lost to follow-up (n=212); those with spontaneous/induced abortions or stillbirths (n=124); and those missing all three serum ferritin measurements at 11–13, 16–19, and 24–27 weeks of gestation (n=1,012), the current analysis included 6,614 pregnant women (
Supplementary Figure S1 ). Serum ferritin levels at 11–13, 16–19, and 24–27 weeks of gestation were extracted from medical records and divided into three groups according to corresponding tertiles. Serum ferritin was measured using chemiluminescent microparticle immunoassay. All laboratory tests were performed according to standardized protocols and underwent regular quality control oversight by the National Center for Clinical Laboratories. GDM was diagnosed based on the International Association of Diabetes and Pregnancy Study Groups criteria (5), which recommend diagnosis when any one of the following plasma glucose values is met or exceeded during the 75g oral glucose tolerance test at 24–28 weeks of gestation: 5.1 mmol/L for fasting, 10.0 mmol/L at 1 hour, and 8.5 mmol/L at 2 hours. Pre-pregnancy body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters, measured at the first antenatal visit.Baseline characteristics are presented as numbers and frequencies for categorical variables and as medians with interquartile ranges (IQRs) for continuous variables. Mann-Whitney U tests and chi-square tests were used to compare skewed continuous variables and categorical variables, respectively. We conducted Poisson regression models to estimate risk ratios (RRs) and 95% confidence intervals (CIs) for GDM across tertiles of serum ferritin measured at 11–13, 16–19, and 24–27 weeks of gestation. The middle tertile of serum ferritin served as the reference group in all analyses. Models were adjusted for demographic and socioeconomic characteristics, including maternal age, education level, employment status, average monthly household income, and ethnicity. Subsequent models incorporated additional adjustments for pre-pregnancy BMI, alcohol consumption during pregnancy, smoking status before pregnancy, passive smoking exposure during pregnancy, parity, and iron supplementation. We further employed restricted cubic spline (RCS) models to examine the dose-response relationship between serum ferritin at 11–13, 16–19, and 24–27 weeks of gestation and GDM risk, with the median serum ferritin value as the reference point and 4 knots positioned at the 5th, 35th, 65th, and 95th percentiles of the distribution. Statistical significance was defined as P<0.05, and all P values were two-sided. All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC).
Among the 6,614 pregnant women enrolled, 1,427 (21.6%) developed GDM. The median (IQR) serum ferritin concentrations were 48.6 (27.5, 77.0), 40.2 (23.1, 66.1), and 21.4 (13.7, 33.1) μg/L at 11–13, 16–19, and 24–27 weeks of gestation, respectively (
Supplementary Table S1 ). Women with GDM demonstrated significantly higher serum ferritin levels at both 16–19 weeks [43.1 (23.7, 73.4) vs. 39.4 (23.0, 64.8) μg/L, P=0.008] and 24-27 weeks of gestation [22.7 (14.5, 36.7) vs. 21.1 (13.5, 32.3) μg/L, P<0.001] compared to non-GDM counterparts (Supplementary Table S1 ). At 11-13 weeks of gestation, GDM rates exhibited a U-shaped pattern across ferritin tertiles, with elevated rates in both the lowest and highest tertiles compared to the medium tertile (Tertile 1 vs. Tertile 2 vs. Tertile 3: 21.1% vs. 16.5% vs. 21.7%, P=0.012). In contrast, at 16-19 weeks (18.9% vs. 18.7% vs. 23.7%, P=0.018) and 24-27 weeks of gestation (20.7% vs. 21.4% vs. 25.6%, P<0.001), the highest ferritin tertile demonstrated the greatest GDM rates (Supplementary Table S2 ). Compared to women without GDM, participants with GDM were significantly older, had higher pre-pregnancy BMI and average household income, exhibited higher rates of Han ethnicity and iron supplementation, and were less likely to be employed or nulliparous (all P<0.05; Table 1).Characteristics Total (n=6,614) GDM (n=1,427) Non-GDM (n=5,187) P Maternal age, year, median (IQR) 31 (28,34) 32 (29,35) 31 (28,34) <0.001 Prepregnancy body mass index, kg/m2, median (IQR) 21.97 (20.03, 24.35) 22.95 (20.75, 25.29) 21.67 (19.84, 24.03) <0.001 Education, n (%) 0.817 Junior school and below 246 (3.7) 50 (3.5) 196 (3.8) Senior high school 493 (7.5) 103 (7.2) 390 (7.5) College or graduate school 5,875 (88.8) 1,274 (89.3) 4,601 (88.7) Employment, n (%) 0.013 Employed 5,782 (87.4) 1,220 (85.5) 4,562 (88.0) Unemployed 832 (12.6) 207 (14.5) 625 (12.0) Average household income per month, CNY, n (%) <0.001 <3,000 226 (3.4) 39 (2.7) 187 (3.6) 3,000 to <5,000 701 (10.6) 121 (8.5) 580 (11.2) 5,000 to <10,000 2,099 (31.7) 419 (29.4) 1,680 (32.4) ≥10,000 3,588 (54.3) 848 (59.4) 2,740 (52.8) Ethnicity 0.023 Han 6,377 (96.4) 1,390 (97.4) 4,987 (96.1) Others 237 (3.6) 37 (2.6) 200 (3.9) Drinking during pregnancy, n (%) 0.167 No 6,127 (92.6) 1,334 (93.5) 4,793 (92.4) Yes 487 (7.4) 93 (6.5) 394 (7.6) Smoking before pregnancy, n (%) 0.730 No 6,510 (98.4) 1,406 (98.5) 5,104 (98.4) Yes 104 (1.6) 21 (1.5) 83 (1.6) Passive smoking during pregnancy, n (%) 0.481 No 6,119 (92.5) 1,314 (92.1) 4,805 (92.6) Yes 495 (7.5) 113 (7.9) 382 (7.4) Parity, n (%) 0.018 0 4,833 (73.1) 1,003 (70.3) 3,830 (73.8) 1 1,623 (24.5) 391 (27.4) 1,232 (23.8) ≥2 158 (2.4) 33 (2.3) 125 (2.4) Iron supplementation, n (%) 0.007 No 4,223 (63.8) 868 (60.8) 3,355 (64.7) Yes 2,391 (36.2) 559 (39.2) 1,832 (35.3) Note: Data are presented as median (interquartile range) or n (%).
Abbreviation: GDM=gestational diabetes mellitus; IQR=interquartile range; CNY=Chinese Yuan.Table 1. Baseline characteristics of participants with and without gestational diabetes mellitus.
At 11–13 weeks of gestation, women in both the lowest (crude RR: 1.28; 95% CI: 1.03, 1.60; adjusted RR: 1.31; 95% CI: 1.05, 1.63) and highest tertiles (crude RR: 1.32; 95% CI: 1.06, 1.64; adjusted RR: 1.33; 95% CI: 1.07, 1.66) demonstrated significantly increased GDM risk in both unadjusted and adjusted models compared with the medium tertile. At 16–19 weeks of gestation, women in the highest serum ferritin tertile exhibited a 1.28-fold elevated risk of GDM (RR: 1.28; 95% CI: 1.03, 1.58) after full adjustment. Similarly, at 24–27 weeks of gestation, the highest tertile showed an adjusted RR of 1.18 (95% CI: 1.03, 1.35) for GDM compared with the medium tertile (Table 2). RCS analysis revealed a U-shaped association between serum ferritin at 11–13 weeks of gestation and GDM risk after adjusting for potential confounders (Poverall<0.001, Pnon-linear=0.008), demonstrating that both lower and higher serum ferritin levels were associated with elevated GDM risk relative to the median value of 48.6 μg/L (Figure 1A). Furthermore, continuous positive associations were observed between serum ferritin at 16–19 weeks (Poverall<0.001, Pnon-linear=0.265; Figure 1B) and 24–27 weeks of gestation (Poverall=0.001, Pnon-linear=0.331; Figure 1C) and GDM risk.
Serum ferritin Case/non-case Model 1 Model 2 Model 3 RR (95% CI) P RR (95% CI) P RR (95% CI) P 11–13 weeks’ gestation Tertile 1 179/669 1.28 (1.03, 1.60) 0.028 1.28 (1.03, 1.60) 0.029 1.31 (1.05, 1.63) 0.018 Tertile 2 140/710 Reference Reference Reference Tertile 3 184/664 1.32 (1.06, 1.64) 0.014 1.34 (1.07, 1.66) 0.010 1.33 (1.07, 1.66) 0.010 16–19 weeks’ gestation Tertile 1 157/673 1.01 (0.81, 1.26) 0.918 1.02 (0.82, 1.27) 0.868 1.05 (0.84, 1.31) 0.677 Tertile 2 155/674 Reference Reference Reference Tertile 3 196/632 1.27 (1.03, 1.56) 0.028 1.29 (1.04, 1.59) 0.019 1.28 (1.03, 1.58) 0.023 24–27 weeks’ gestation Tertile 1 389/1,490 0.97 (0.84, 1.11) 0.641 0.96 (0.83, 1.10) 0.531 0.97 (0.84, 1.11) 0.639 Tertile 2 400/1,469 Reference Reference Reference Tertile 3 479/1,390 1.20 (1.05, 1.37) 0.008 1.21 (1.06, 1.38) 0.005 1.18 (1.03, 1.35) 0.014 Abbreviation: CI=confidence interval; RR=risk ratio.
Note: Values in bold are statistically significant. Values represent risk ratios with 95% CIs. Model 1 presents unadjusted estimates. Model 2 were adjusted for demographic and socioeconomic characteristics, including maternal age, education level, employment status, average monthly household income, and ethnicity. Model 3 incorporates additional adjustments for pre-pregnancy body mass index, alcohol consumption during pregnancy, smoking status before pregnancy, passive smoking exposure during pregnancy, parity, and iron supplementation.Table 2. Risk ratios and 95% CIs of gestational diabetes mellitus according to tertiles of serum ferritin.
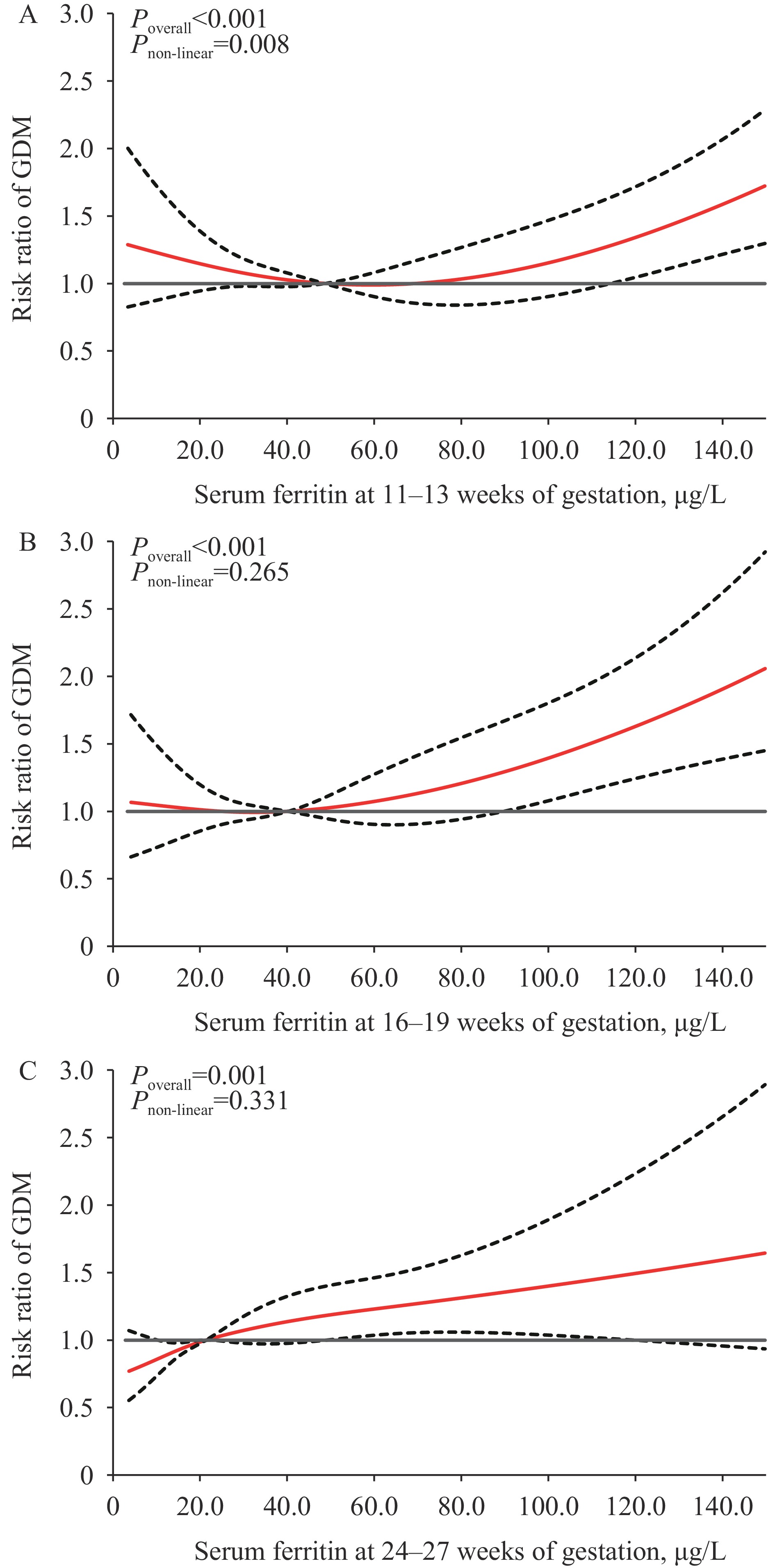 Figure 1.
Figure 1.Risk ratios and 95% confidence intervals for the association between serum ferritin at 11–13 weeks; (A) 16–19 weeks, (B) and 24–27 weeks of gestation, (C) with GDM.
Abbreviation: GDM=gestational diabetes mellitus.
Note: Models were adjusted for maternal age, education level, employment status, average monthly household income, ethnicity, pre-pregnancy body mass index, alcohol consumption during pregnancy, smoking status before pregnancy, passive smoking exposure during pregnancy, parity, and iron supplementation.
-
This multicenter, prospective cohort study provides longitudinal evidence on serum ferritin levels measured at multiple time points during the first and second trimesters. Most notably, this study identified a U-shaped association between serum ferritin at 11–13 weeks of gestation and GDM risk — the first study to demonstrate this relationship in a Chinese population. Additionally, we found that elevated ferritin levels at both 16–19 and 24–27 weeks of gestation were independently associated with increased GDM risk.
A key finding of this study was the U-shaped relationship between serum ferritin at 11–13 weeks of gestation and GDM, indicating that both lower and higher ferritin concentrations were associated with elevated GDM risk. Supporting our findings, a previous prospective study in Anhui province, China, reported a similar U-shaped relationship between first-trimester serum iron — another important indicator of iron status — and GDM risk (6). Earlier case-control studies in U.S., Danish, and Chinese populations with relatively small sample sizes revealed that excessive first-trimester ferritin levels were significantly associated with higher GDM risk, while several larger prospective and retrospective cohort studies demonstrated positive associations between first-trimester ferritin and GDM (3,7–8). However, the relationship between lower ferritin levels and GDM has received insufficient attention. To our knowledge, this represents the first prospective cohort study to demonstrate a U-shaped association between first-trimester serum ferritin and GDM risk in a Chinese population, contributing to a more comprehensive understanding of the ferritin-GDM relationship.
Our findings also demonstrated that higher ferritin levels at 16–19 and 24–27 weeks of gestation were independently associated with increased GDM risk, consistent with a prior meta-analysis showing that the highest ferritin category in the second trimester was associated with a 79% increase in GDM risk compared with the lowest category (9). Supporting our results, a prospective cohort study of central Chinese women reported that elevated ferritin concentrations around 16 weeks of gestation were independently associated with higher GDM risk (10). Similarly, a recent retrospective study of western Chinese women indicated that GDM patients exhibited higher ferritin levels than controls in the second trimester (11). Iron overload may explain the relationship between elevated serum ferritin during pregnancy and GDM through multiple pathways: inducing hepatic and peripheral insulin resistance, causing β-cell injury and apoptosis, heightening oxidative stress and inflammatory responses, and impairing insulin signaling pathways and hepatocyte insulin uptake (3). Conversely, iron deficiency may contribute to GDM by increasing lipogenic gene expression and altering lipid profiles, which could partially promote hyperglycemia (12). Additionally, serum ferritin during pregnancy is influenced by dietary patterns, particularly heme iron intake, which has been significantly associated with increased GDM risk (13). Future mechanistic research is needed to elucidate the precise pathways through which serum ferritin in the first and second trimesters affects GDM development.
These findings have important public health and clinical implications. The significant association between serum ferritin in the first and second trimesters and GDM risk supports the potential utility of ferritin monitoring for early identification and prevention of GDM. Our results suggest that serum ferritin measurement at 11–13 weeks of gestation should be incorporated into routine prenatal care, with pregnant women exhibiting either lower or higher levels undergoing enhanced glycemic screening before 24 weeks of gestation. Furthermore, iron supplementation during pregnancy should be individualized based on serum ferritin levels to prevent both deficiency and excess. Comprehensive screening strategies for serum ferritin during pregnancy are necessary to detect iron deficiency and overload, thereby optimizing the balance between the benefits and risks of iron supplementation.
This study has several limitations. First, we measured only serum ferritin as an indicator of iron stores and did not assess other markers such as serum iron and transferrin receptor, although serum ferritin is considered the preferred indicator of iron storage. Second, because serum ferritin levels can increase during acute inflammation and infections, the absence of inflammatory markers prevented us from examining how these factors might influence the association between serum ferritin and GDM. Third, we did not collect data on the dosage and duration of iron supplementation, limiting our ability to assess how these factors might modify GDM risk. Fourth, participants were recruited from four tertiary hospitals, which may not represent the general pregnant population in China. Therefore, multi-center, population-based studies are needed to validate these findings.
In conclusion, we identified a U-shaped association between first-trimester serum ferritin and GDM risk, and demonstrated that elevated second-trimester serum ferritin was independently associated with increased GDM risk. These findings underscore the need for strategies to enhance understanding and clinical application of serum ferritin measurements in the early identification and prevention of GDM.
-
Gratefully acknowledge all participants, investigators, and staff who contributed to this study.
-
Approval by the institutional review board of Peking University First Hospital (2018[267]). All participants provided written informed consent prior to enrollment.
HTML
| Citation: |

|