
 Download:
Download:




-
Introduction: To investigate the molecular epidemiological links among clustered cases of carbapenem-resistant Acinetobacter baumannii (CRAB) nosocomial infections occurring in different years within an intensive care unit (ICU) in Jiangsu Province, China and identify gaps in infection control in multibed ICU settings.
Methods: A retrospective study was conducted on five clusters of CRAB infections in 2016, 2019, and 2021. Twenty clinical and forty environmental A. baumannii isolates were analyzed using pulsed-field gel electrophoresis (PFGE) for molecular typing, and antimicrobial susceptibility testing for resistance profiling.
Results: PFGE revealed high genetic similarity (>90%) among clinical and environmental isolates from 2016, 2019, and 2021, indicating the persistent environmental transmission of CRAB over multiple years. All patient-derived strains were CRAB strains. No homologous strains were detected after thorough disinfection of the terminals in 2021.
Conclusions: CRAB demonstrated remarkable environmental persistence in ICUs, suggesting limitations in current disinfection practices. Enhanced disinfection strategies targeting high-touch complex surfaces are necessary to interrupt CRAB transmission and reduce nosocomial outbreaks.
-
Acinetobacter baumannii is a conditionally pathogenic gram-negative bacterium that has emerged as a major pathogen causing hospital infection outbreaks because of its ability to adapt to various environmental conditions. As a critical multidrug-resistant pathogen in nosocomial infections, A. baumannii has accounted for more than 10% of all gram-negative hospital infections in intensive care units (ICUs) in Europe and the United States over the last 10 years, and this proportion continues to rise (1–2). The mortality rate associated with nosocomial outbreaks, which were mainly reported from ICUs (104 in ICU/150 total), caused by A. baumannii is approximately 48% multi-drugresistant and 42.5% non-multidrug resistant (3). Moreover, the World Health Organization (WHO) has classified Carbapenem-resistant Acinetobacter baumannii (CRAB) as a critical group of bacteria that poses the most severe threat to human health (4).
In China, this situation is of equal concern and cannot be overlooked. The 2023 China Bacterial Drug Resistance Surveillance revealed that A. baumannii accounted for 87.6% of Acinetobacter spp. The resistance rates of these strains to all antibiotics except polymyxin and tigecycline exceeded 48%. The resistance rates of A. baumannii to meropenem and imipenem were 73.7% and 73.4%, respectively, ranking fourth among the top 20 most important clinical isolates (5). Owing to its pan-drug resistance, A. baumannii has become a formidable challenge for infection control in intensive care wards and a notable cause of death among patients with severe infections.
In a single ward with abundant hospital resources, isolation and terminal disinfection measures have effectively controlled drug-resistant bacteria, including A. baumannii (6). However, ICUs are rarely designed as single-room ward models. Instead, they generally have multibed, large-room layouts. Patients in ICUs have extended stays and are not easily moved. Once hospital infections occur, isolation becomes ineffective, and disinfection serves as the sole measure to cut off transmission routes. This study aimed to explore the molecular link between multiple clusters of CRAB nosocomial infections in different years and to identify gaps in the current disinfection protocols for multibed ICUs in a hospital in Jiangsu Province, China.
A tertiary hospital in Jiangsu Province with approximately 4,000 beds was selected for this study. The emergency ICU consisted of 8 wards with 25 beds. A. baumannii strains were obtained from different aggregated cases in the emergency ICU during 2016–2021 from different aggregated cases (According to the guidelines for the control of healthcare-associated infection outbreaks WS/T 524-2016, the occurrence of 3 cases of hospital-acquired infections with the same pathogenic microorganism was regarded as an aggregated case) and the related ICU circumstances. Related pathogen surveillance was conducted from 2021 to 2024, following thorough terminal disinfection. Samples were collected from the sputum, blood, and wounds (Figure 1).
 Figure 1.
Figure 1.PFGE dendrogram of A. baumannii aggregated case groups by bed number, location, and source.
Note: 60 isolates (20 clinical and 40 environmental isolates) were included. The cluster analysis dendrogram is a molecular analysis performed by BioNumerics software to classify different A. baumannii strains based on band similarity, with a similarity value greater than 90% indicating the same origin. Study ID refers to the research identification numbers assigned in this study to A. baumannii strains isolated from patients or the environment. The Study IDs with an asterisk denote non-carbapenem Acinetobacter baumannii isolates. Bed No. location/source indicates the bed number and the type of patient specimen/environmental location from which the strain was isolated. Type denotes clusters identified by the software as strains of the same origin.
Abbreviation: AB=A. baumannii=Acinetobacter baumannii; PFGE=pulsed-field gel electrophoresis; ID=Identity Document.
Environmental samples were collected by converting the high-contact surfaces of the ICU (bed rails, device controls/screens, charts, and call buttons) and general wards (door handles, carts, faucets, and sinks), nurses’ stations (staff white coats, work surfaces, faucets/sinks, and drawer handles/phones), and dispensing and cleaning rooms (countertops, carts, faucets/sinks, door handles, and cleaning tools).
Bacterial isolates were initially purified on chromogenic medium plates. Species identification was performed using matrix-assisted laser desorption ionization time-of-flight mass spectrometry, calibrated with Salmonella H9812, and the results were analyzed using the Myla system. Antimicrobial susceptibility testing (AST) of A. baumannii utilized the VITEK2 system with GN AST-09 cards. Molecular typing of isolates was conducted via pulsed-field gel electrophoresis (PFGE) using the CHEF MAPPER™ system (BIO-RAD); DNA was digested by the ApaI restriction enzyme. The PFGE process was carried out at a voltage gradient of 6.0 V/cm, an angle of 120°, a temperature of 14 ℃, with pulse time ranging from 5–20 s, and lasted 18.5 h. PFGE gel images were analyzed using BioNumerics software. A. baumannii strains exhibiting more than 90% similarity based on Dice coefficients were classified as related strains.
A total of 5 aggregated clusters involving 19 patients were identified in 2016 (1st cluster, 3 cases), 2019 (2nd cluster, 4 cases; 3rd cluster, 5 cases; 4th cluster, 2 cases), and 2021 (5th cluster, 2 cases). From these clusters, 20 A. baumannii strains were isolated (2 strains were isolated from the patient’s exudate and peritoneal drainage fluid, respectively) (
Supplementary Table S1 ). In addition, 40 A. baumannii strains were isolated from the environmental samples (Supplementary Table S2 ). Among the 19 patients, 10 were co-infected with other pathogens, specifically Klebsiella.The AST results for all isolates are presented in Supplementary Table S2. Among the 60 A. baumannii strains, 86.7% (52/60) were CRAB, including all 20 strains isolated from patients. Among the 52 strains exhibiting resistance to imipenem, 40 were resistant to meropenem and were recognized as CRAB.
PFGE was performed on 60 isolates, including 20 clinical and 40 environmental isolates. The 60 isolates were divided into 9 groups using a similarity cutoff of 90% (Figure 1). The largest group, A, comprised 29 isolates, including 10 from 9 patients (1st, 2nd, and 5th cluster patients in 2016, 2019, and 2021, respectively) and 19 from the relevant environment. The second largest group D had 16 isolates (3rd and 4th clusters in March and October-November in 2019, respectively) and the 9 related environmental isolates (notably including a sample from 2016).
As confirmed by PFGE, the aggregated cases in June 2016 (3 cases) were identified as the same type of CRAB infection. Notably, 4 patients in 2019 (XZ191010ABP001, XZ191012ABP003, XZ191012ABP002, and XZ191012ABP005) and 2 patients in 2021 (XZ210910ABP001 and XZ210916ABP003) were also infected with the same type of CRAB as in 2016 (Figure 1). With regard to the locations of the patient and environmental samples, in 2016, the aggregated cases came from 2 multibed rooms (bed 8 in room 2 and beds 13 and 14 in room 3). The contaminated environmental area included the adjacent multibed room (4), the more distant double room (7), and the multibed room where the cases were located. The collected environmental area included 7 beds and 13 locations. In 2019, the aggregated cases were from 3 multibed rooms (bed 6 in room 1; beds 8 and 9 in room 2; and bed 18 in room 4). The contaminated environmental areas included the more distant double room 7 and multibed rooms where the cases were located. The collection area consisted of 5 beds and 6 locations. In 2021, the aggregated cases came from 2 multibed rooms (bed 5 in room 1 and bed 23 in room 7), and the environmental areas in these rooms were not contaminated (Figure 2A).
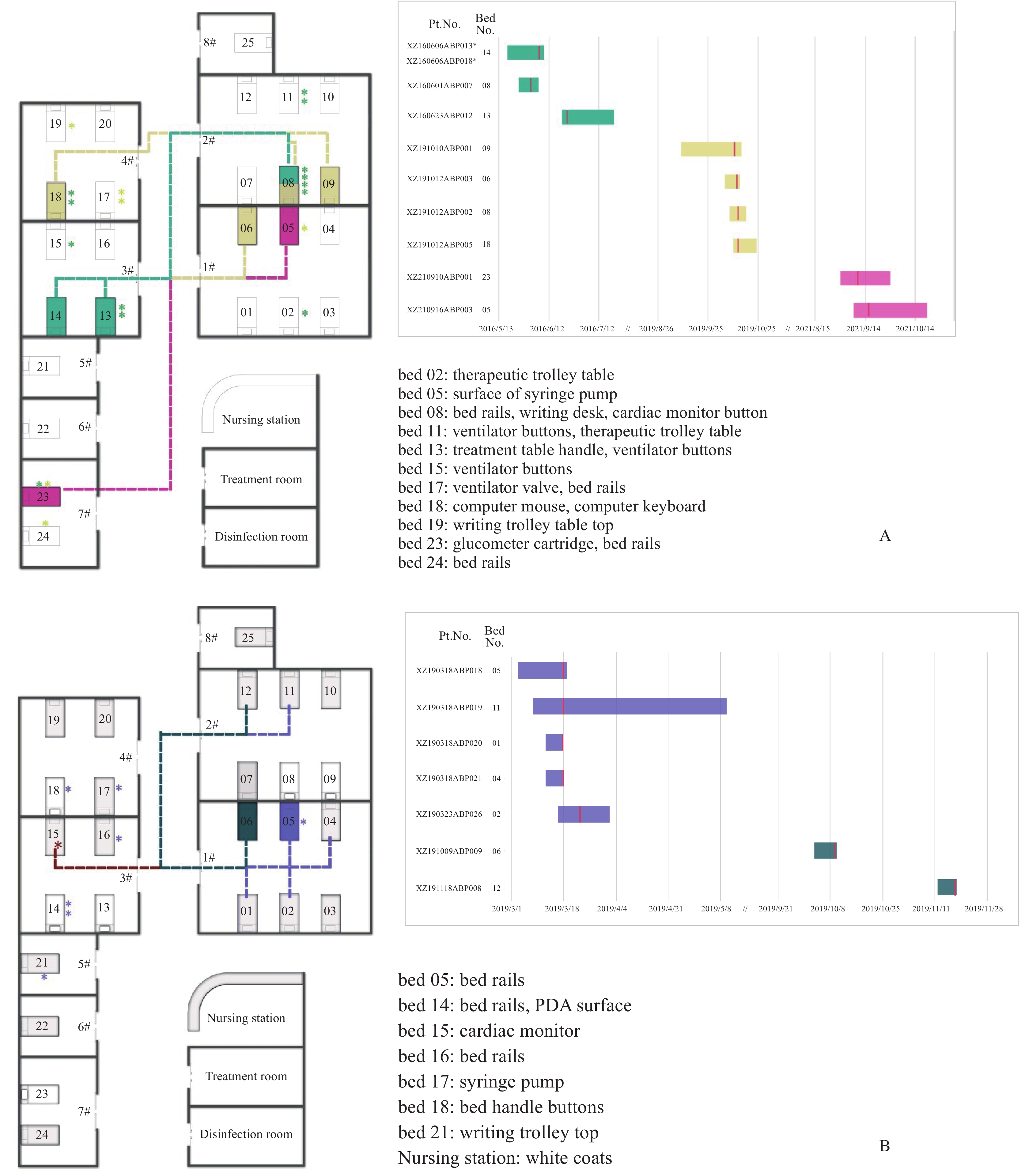 Figure 2.
Figure 2.Summary of environmental positive samples, bed sites of HAI patients, and timeline of aggregated cases in the emergency ICU. (A) The 2016-2019-2021 aggregated cases. Light green, yellow, and magenta represent all samples collected in 2016, 2019, and 2021, respectively; (B) The 2016–2019 (March, Oct–Nov) aggregated cases.
Note: For B, brown, purple, and dark green represent environmental samples collected in 2016, and all samples collected in 2019 and 2021, respectively. All environmental sample collection locations are marked with asterisks on the map, using the same color as the bed positions of clinical cases at the same time, with textual annotations beside the map. Dashed lines represent molecular homology between different clinical cases. The sample collection times of clinical cases are indicated with red vertical lines on the timeline.
Abbreviation: HAI=healthcare-associated Infection; ICU=intensive care unit.
The second largest group of aggregated cases (group D), identified by PFGE, consisted of 5 cases in March 2019 and 2 cases from October to November 2019. These cases are homologous to those of the 2016 single-strain environmental samples. In March 2019, the cases came from beds 1, 2, 4, and 5 in room 1 and bed 11 in room 2, situated in 2 adjacent multiplexes (rooms 1 and 2). The contaminated environmental areas extended beyond the rooms where the patients stayed, encompassing adjacent multibed rooms 3 and 4 and a single room 5. Environmental samples were collected from 6 locations in the study area. During October-November, the aggregated cases came from bed 6 in room 1 and bed 12 in room 2. The contaminated environmental areas included nurse stations (Figure 2B).
-
In this retrospective study, molecular biology methods were successfully employed to trace multiple cases of clustered hospital-acquired infections in 2016 and beyond. These infections originated from both patients and the environment. Given that the study setting was an acute-care ICU, the hospital did not screen every admitted patient for multidrug-resistant bacteria and prior pathogen preservation from this ICU was not available. Consequently, determining whether the initial infections in 2016 were community-acquired or hospital-acquired/colonized was difficult. Using molecular biology analyses, subsequent cases (XZ160620ABP012 in 2016, 4 cases in 2019, and 2 cases in 2021) were judged to be molecular epidemiology-related and may be of the same origin. This retrospective analysis found that CRAB infections in ICUs in China shared similarities with the colonization and infection of VIM-producing Pseudomonas aeruginosa and NDM-producing Enterobacteriaceae in adults admitted to the ICU of a tertiary care hospital in Belgium between 2018 and 2022 (7).
PFGE confirmed that the aggregated cases in March 2019 (5 cases) and October–November 2019 (2 cases) were possibly caused by the same CRAB strain. According to the analysis of the sample collection time, the source of these 2 clustered cases was likely an environmental pathogen (XZ160704ABE019) collected from a 15-bed cardiac monitor in 2016. This study hypothesized that the buttons of cardiac monitors are an environmental reservoir of A. baumannii, along with the ventilators (7 samples) and syringe pumps (3 samples) used in this study. Such equipment with buttons is difficult to disinfect (8) and can facilitate the spread of infection through contact transmission, which can lead to associated transmission when healthcare workers fail to change gloves or perform hand hygiene after touching the equipment.
The transmission routes of the aggregated cases were analyzed. Although the study spanned a long time, this study was able to initially rule out the sharing of medical equipment as a possible transmission route by determining the source of the environmental samples. In contrast to previously published studies (9), A. baumannii environmental isolates were collected from only a few shared medical devices. A possible reason for this is that this study was conducted in the ICU, which generally has better-equipped facilities than the average department and does not require multiple patients to share medical devices. This study found that the only possibility for sharing was in the case of treatment carts, which are mobile medical devices (Figure 2).
A. baumannii bloodstream infections pose a serious risk to human health due to their high mortality rates (10). In the present study, infection was detected in only one blood sample (
Supplementary Table S2 ). This finding is consistent with that reported by Kong et al. (11), who detected infections mainly in respiratory samples. This phenomenon may be related to the high number of mechanical ventilations in ICUs, which is a risk factor for hospital-acquired infections.Drug sensitivity analysis revealed that all patient specimens were classified as CRAB. Physicians tend to use high-dose ampicillin-sulbactam to treat CRAB infections (12). Of the 20 patient samples, 1 (XZ160623ABP012) was resistant to ampicillin, sulbactam, and imipenem. This may lead to difficulties in treatment. However, 32 environmental samples were resistant to both antibiotics, which is another cause for concern. A strain of A. baumannii resistant to polymyxin B, imipenem, and meropenem was collected by a nurse. Polymyxins are effective treatments for CRAB (13). Bacteria that demonstrate simultaneous resistance to these drugs represent a major obstacle to treatment in the ICU. However, this strain was not detected in the aggregated cases.
In 2016, this study’s authors implemented local disinfection measures in the ICU when they identified a short period of aggregated A. baumannii infection. No hospital-acquired infections with the same A. baumannii strain were recorded during the subsequent period. However, the retrospective discovery of molecularly linked cases in 2019 and 2021 suggests the presence of unidentified environmental reservoirs. Pathogenic microorganisms may still be present in 50% of patients after routine disinfection (14). Based on this evidence, the ICU transferred patients temporarily and instituted comprehensive terminal disinfection; no reappearance of relevant strains has been detected since then.
In conclusion, the data strongly imply that CRAB, which is responsible for aggregated cases of infections in ICUs, exhibits remarkable environmental persistence. This study observed that clustered cases occurring in different years over a five-year period may have close molecular epidemiological connections, suggesting that CRAB may pose a potential ongoing risk and could be one of the causes contributing to the occurrence of clustered infections in the ICU. Developing and implementing advanced disinfection techniques (such as vaporized or aerosolized hydrogen peroxide disinfection and the use of antimicrobial surface materials) and protocols tailored specifically to ICU settings are imperative for effectively mitigating CRAB transmission and reducing the incidence of hospital-acquired infections and outbreaks. Improved disinfection measures should target the unique characteristics of CRAB and the ICU environment, interrupt its transmission routes, and safeguard patient health.
This study has some limitations. Due to financial and human resource constraints, it did not follow up or analyze every case of hospital-acquired infection. Patient and environmental samples were collected only when aggregated cases were found in the hospitals. Therefore, the presence of individual cases among the aggregated cases was unclear. This study can only surmise from the molecular correlation that the subsequent aggregated cases might be from the aggregated cases and environmental samples collected in 2016. A clearer molecular epidemiological chain could be established with more comprehensive case tracking. However, the impact of this limitation is constrained, as the conclusions of this study are well supported by the molecular data from the aggregated cases that were collected.
-
Approved by Clinical Research and Ethics Committee of the tertiary hospital (approval no. XYFY2022-KL027-01).
-
The CDC sampling team and hospital staff who helped with data collection and supported our study.
HTML
| Citation: |

|