
 Download:
Download:




-
Introduction: Echinococcosis, a neglected zoonotic disease, imposes a substantial global health burden. Enhancing health literacy and facilitating practice changes among pastoral communities through innovative technological interventions are essential for reducing disease transmission and impact. We evaluated the effectiveness of the Smart Health Education Pillbox (SHEP) on the knowledge, attitudes, and practices (KAP) of dog owners in controlling echinococcosis.
Methods: We conducted a cluster-randomized trial among 2,700 dog owners across nine endemic counties in western China, selecting two townships per county. Within each township, 150 enrolled dog owners were randomly allocated in equal numbers to either the Smart Health Education Pillbox (SHEP) or routine health education (RHE) group. Data were collected through a validated online questionnaire (Cronbach’s α=0.85) distributed via the Wenjuanxing platform. Primary outcomes included knowledge, attitude, and practice rates, as well as practice conversion efficiency. Statistical analyses were performed to calculate absolute risk reduction (ARR), relative risk (RR), relative risk reduction (RRR), protective efficacy (1/RR), and conversion efficiency index (η).
Results: Implementation of the SHEP significantly enhanced dog owners’ knowledge, attitudes, and practices by 6.78%, 3.30%, and 7.50%, respectively, while reducing misconceptions, negative attitudes, and improper practices by 43.92%, 28.60%, and 13.74% compared to RHE (all P<0.001). The intervention demonstrated protective efficacy ratios of 1.82, 1.40, and 1.16 across these domains and increased the overall conversion efficiency index by 7.88% (all P<0.001).
Conclusion: The SHEP represents a superior intervention for improving echinococcosis-related knowledge, attitudes, and practices (KAP), demonstrating particular strength in enhancing knowledge-to-practice conversion. As an innovative solution addressing health education challenges in plateau pastoral areas, the SHEP is recommended for integration into the national echinococcosis control program.
-
Echinococcosis, a neglected tropical zoonosis with cross-species transmission potential, manifests primarily as cystic echinococcosis (CE) and alveolar echinococcosis (AE), caused by Echinococcus granulosus sensu lato and E. multilocularis, respectively. These forms are endemic across 370 counties in northwestern China, with 115 experiencing co-endemicity (1). Annually, CE accounts for approximately 18,800 new cases and 1 million disability-adjusted life years (DALYs), with China bearing 40% of this global burden. AE is responsible for an estimated 18,200 cases and 666,000 DALYs annually, over 90% occurring within China. The combined annual economic burden reaches approximately 3 billion US dollar (USD), predominantly borne by China (2–3). Consequently, echinococcosis has been designated a priority infectious disease for control within China’s One Health framework (4).
Health education represents a cost-effective foundational intervention for echinococcosis control. New Zealand achieved elimination through legislative measures enforcing “canine management+public health education.” South American nations including Argentina and Chile achieved human incidence reductions exceeding 60% through sustained “dog deworming+community education” campaigns (5). In China, the National Echinococcosis Control Program (2010–2015) and subsequent implementation plan (2024–2030) emphasize integrated strategies combining source control, health education, intermediate host management, and case treatment, prioritizing culturally tailored health materials for pastoral areas (6). After two decades of sustained efforts, improvements in knowledge, attitudes, and practices (KAP) among residents have contributed to reduced transmission (7–8). However, conventional health education approaches — including pamphlets, lectures, social media, and targeted training — face persistent challenges from low literacy levels, linguistic diversity, sporadic outreach, and coverage disparities (6,9). Lower awareness of echinococcosis control (P<0.01) was observed among high-altitude pastoral residents compared to urban/peri-urban residents (9). Addressing these gaps requires smart, precise, digitalized health education tools ensuring sustainable, equitable, and effective delivery of control messages to reduce disease burden.
Between 2021 and 2023, we developed an AI and IoT-enabled SHEP with a dedicated anthelmintic bait compartment, two reminder lights, a liquid-crystal display, six function buttons, and an integrated speaker and charging port (Figure 1). Core functions include automated deworming reminders and delivery of at least three daily health education broadcasts per household. We conducted a 12-month cluster-randomized trial from 2023 to 2024 across nine endemic counties (10). Within each county, two townships were randomly assigned to intervention arms using a computer-generated random number table. The SHEP group received automated intervention with digitized core knowledge delivery, while the routine health education (RHE) group received standard health education through pamphlets, WeChat, and conventional methods. Sample size calculations determined that 150 eligible dog owners per township would provide 90% power to detect significant differences at the two-sided 5% significance level.
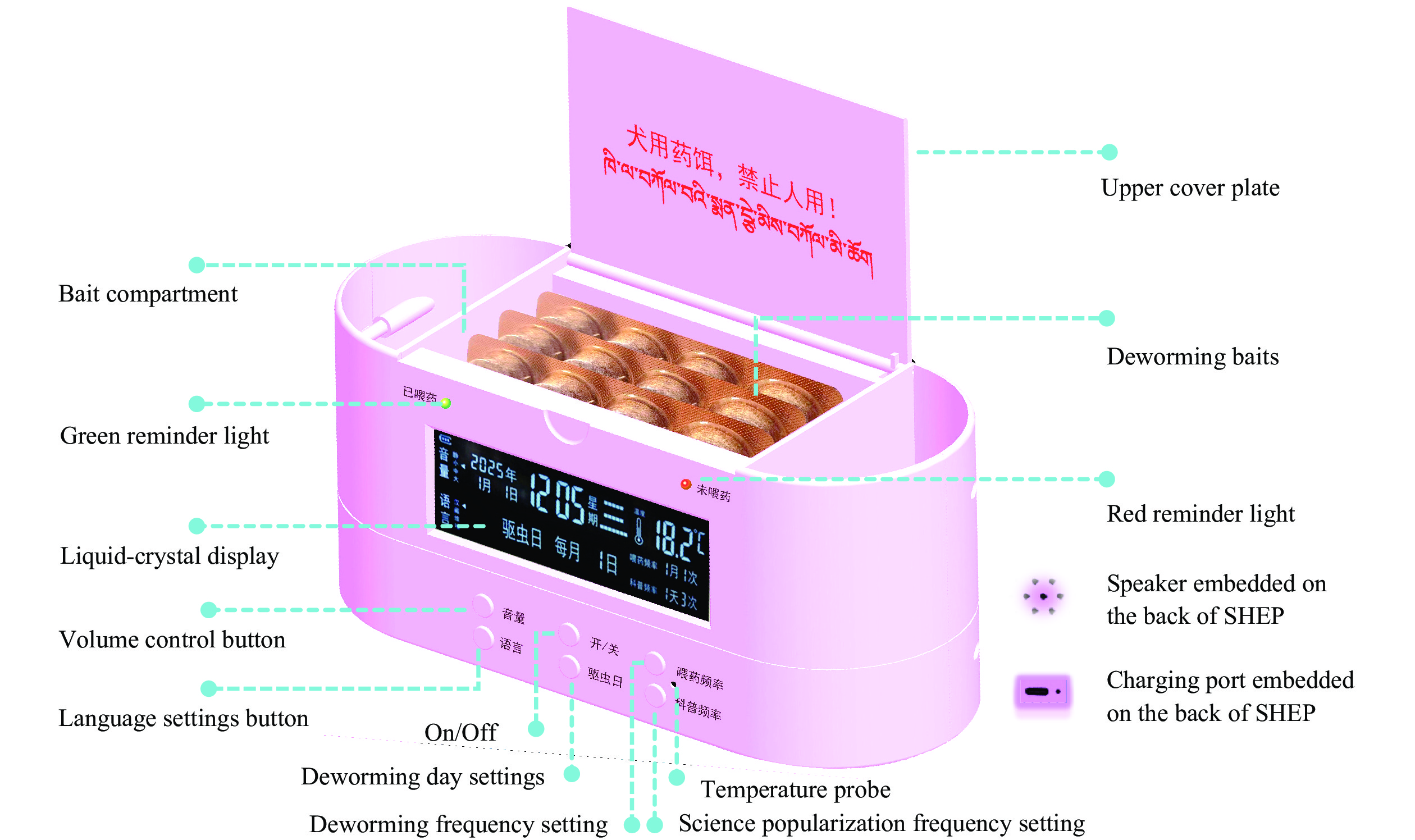 Figure 1.
Figure 1.Structure and functionalities of Smart Health Education Pillbox.
Abbreviation: SHEP=Smart Health Education Pillbox.A baseline survey was conducted in 2023 using a questionnaire with satisfactory internal consistency (Cronbach’s α=0.85) through face-to-face, in-home interviews with all 2,700 eligible dog owners. One year later, a follow-up assessment was administered to both randomized groups of 1,350 participants each. Data were collected using a validated online questionnaire on the Wenjuanxing platform, capturing demographic characteristics, socioeconomic status, and KAP related to echinococcosis. A pilot survey was conducted and multilingual versions were provided to ensure data quality. Blinding was maintained through separate surveyors for each group and independent WeChat groups for survey administration.
Data from the Wenjuanxing platform were entered into MS-Excel and analyzed using SPSS software (version 27.0, IBM Corp., NY, USA). Categorical variables were reported as counts (n) and percentages (%). Primary outcomes included knowledge, attitude, and practice rates related to echinococcosis control, and conversion efficiency. These were assessed using absolute risk reduction (ARR), relative risk (RR), relative risk reduction (RRR), protective efficacy (1/RR), and conversion efficiency index (η). Between-group comparisons used the chi-square test or Fisher’s exact test, with two-tailed testing and statistical significance at P<0.05.
At baseline, all 2,700 dog owners completed the survey. At one-year follow-up, retention rates were 75.63% (n=1,021) in SHEPG and 68.89% (n=930) in RHEG. The survey employed a nine-item knowledge questionnaire across five domains: basic knowledge, policy awareness, transmission routes, key practices, and livestock management. The knowledge rate in SHEPG reached 91.35%, significantly exceeding both RHEG and baseline by 6.78% [ARR=6.78%; 95% confidence interval (CI): 5.95, 7.61; P<0.001] and 6.50% (ARR=6.50%; 95% CI: 5.71, 7.29; P<0.001), respectively. SHEP intervention substantially reduced the risk of knowledge gaps and misconceptions compared to both groups. The relative risk reduction was 43.92% (RRR, 95% CI: 40.23, 47.61; P<0.001) versus RHEG and 42.97% (RRR, 95% CI: 39.38, 46.56; P<0.001) versus Baseline. Relative probabilities of incomplete or incorrect knowledge were reduced to 0.55 times RHEG (RR, 95% CI: 0.51, 0.59; P<0.001) and 0.57 times Baseline (RR, 95% CI: 0.53, 0.61; P<0.001). SHEP demonstrated protective efficacy of 1.82-fold against knowledge inaccuracies relative to RHE (1/RR, 95% CI: 1.70, 1.96; P<0.001) and 1.75-fold relative to Baseline (1/RR, 95% CI: 1.64, 1.88; P<0.001) (Table 1;
Supplementary Table S1 ). RHEG showed marginal, non-significant decrease in knowledge rate versus Baseline (ARR=−1.85; 95% CI: −8.32 to 4.62; P=0.575; RR=1.02; 95% CI: 0.96–1.08; P=0.569) (Supplementary Table S2 ). Detailed knowledge rates and response frequencies for questions 1–9 are in Table 1 andSupplementary Tables S1–S2 .Question Response Baseline
[% (n/N)]SHEPG
[% (n/N)]CHEG
[% (n/N)]ARR RRR RR 1/RR 95% CI P 95% CI P 95% CI P 95% CI P Q1. Have you heard of echinococcosis? Yes (correct) 93.89 (2,535/2,700) 96.87 (989/1,021) 90.97 (846/930) 5.90 (3.56, 8.24) <0.001 65.33 (39.41, 91.24) <0.001 No 3.96 (107/2,700) 0.59 (6/1,021) 4.95 (46/930) 4.36 (3.07, 5.65) <0.001 88.08 (72.96, 95.04) <0.001 0.12 (0.05, 0.28) <0.001 8.47 (3.57, 20.08) <0.001 Not sure 2.15 (58/2,700) 2.55 (26/1,021) 4.09 (38/930) 1.54 (0.19, 2.89) 0.026 37.65 (3.59, 61.52) 0.026 0.62 (0.38, 1.02) 0.058 1.61 (0.98, 2.63) 0.058 Q2. How do people get echinococcosis? Get infected if they accidentally ingest worm eggs excreted by dogs or foxes (correct) 66.33 (1,791/2,700) 71.69 (732/1,021) 66.92 (615/919)† 4.77 (0.90, 8.64) 0.016 14.43 (2.73, 26.14) 0.016 By eating unclean internal organs of cattle or sheep 29.67 (801/2,700) 27.23 (278/1,021) 30.47 (280/919)† 3.24 (−0.57, 7.05) 0.095 14.43 (2.73, 26.14) 0.016 0.89 (0.78, 1.03) 0.126 1.12 (0.97, 1.28) 0.126 Human-to-human 4.00 (108/2,700) 1.08 (11/1,021) 2.61 (24/919)† 1.53 (0.41, 2.65) 0.007 58.62 (17.30, 79.86) 0.007 0.41 (0.21, 0.83) 0.013 2.44 (1.20, 4.76) 0.013 Q3. How do dogs get infected with Echinococcus? By consuming the diseased internal organs of cattle or sheep (correct) 93.03 (1,976/2,124)† 98.53 (1,006/1,021) 96.34 (896/930) 2.19 (0.87, 3.51,) 0.001 59.46 (23.64, 95.28) 0.001 Dog-to-dog 6.50 (138/2,124)† 0.98 (10/1,021) 2.15 (20/930) 1.17 (0.20, 2.14) 0.018 54.42 (5.26-79.63) 0.018 0.45 (0.22-0.95) 0.036 2.22 (1.05-4.55) 0.036 Human-to-dog 0.47 (10/2,124)† 0.49 (5/1,021) 1.51 (14/930) 1.02 (0.22, 1.82) 0.012 67.55 (12.33, 87.80) 0.012 0.32 (0.12, 0.88) 0.028 3.13 (1.14, 8.33) 0.028 Q4. Are you aware of the national policies for echinococcosis patients? Fully aware (correct) 43.85 (1,184/2,700) 73.16 (747/1,021) 49.13 (450/916)† 24.03 (20.32, 27.74) <0.001 47.30 (39.98, 54.61) <0.001 Partially aware 46.33 (1,251/2,700) 25.86 (264/1,021) 41.48 (380/916)† 15.62 (11.48, 19.76) <0.001 37.66 (27.68, 47.63) <0.001 0.62 (0.55, 0.71) <0.001 1.60 (1.41, 1.82) <0.001 Not aware 9.81 (265/2,700) 0.98 (10/1,021) 9.39 (86/916)† 8.41 (6.73, 10.09) <0.001 89.56 (82.71, 94.99) <0.001 0.10 (0.05, 0.20) <0.001 9.58 (5.01, 18.33) <0.001 Q5. Is deworming dogs a preventive measure for echinococcosis? Yes (correct) 96.96 (2,618/2,700) 99.80 (1,019/1,021) 95.46 (799/837)† 4.34 (2.92, 5.76) <0.001 95.45 (64.10, 126.80) <0.001 No 1.56 (42/2,700) 0.00 (0/1,021) 2.03 (17/837)† 2.03 (1.01, 3.05) <0.001 100.00 (58.04, 100.00)* <0.001 0.05 (0.00, 0.79)* 0.033 19.61 (1.27, ∞)* 0.033 Not sure 1.48 (40/2,700) 0.20 (2/1,021) 2.51 (21/837)† 2.31 (1.30, 3.32) <0.001 92.03 (67.18, 98.48) <0.001 0.08 (0.02, 0.33) <0.001 12.82 (3.03, 50.00) <0.001 Q6. Is the safe disposal (deep burial) of dog feces a preventive measure for echinococcosis? Yes (correct) 90.70 (2,449/2,700) 93.83 (958/1,021) 89.35 (831/930) 4.48 (2.16, 6.80) <0.001 42.11 (20.32, 63.90) <0.001 No 5.15 (139/2,700) 4.80 (49/1,021) 4.19 (39/930) −0.61 (−2.46, 1.24) 0.518 −14.56 (−71.49, 42.37) 0.518 1.15 (0.77, 1.71) 0.498 0.87 (0.58, 1.30) 0.498 Not sure 4.15 (112/2,700) 1.37 (14/1,021) 6.45 (60/930) 5.08 (3.55, 6.61) <0.001 78.76 (63.45, 88.12) <0.001 0.21 (0.12, 0.37) <0.001 4.76 (2.70, 8.33) <0.001 Q7. Is not feeding raw livestock internal organs to dogs a preventive measure for echinococcosis? Yes (correct) 90.74 (2,450/2,700) 92.26 (942/1,021) 86.56 (805/930) 5.70 (3.10, 8.30) <0.001 42.54 (23.13, 61.94) <0.001 No 6.26 (169/2,700) 6.95 (71/1,021) 6.02 (56/930) −0.93 (−3.24, 1.38) 0.430 −15.45 (−53.76, 22.86) 0.430 1.15 (0.77, 1.71, 0.498) 0.498 0.87 (0.58, 1.30) 0.498 Not sure 3.00 (81/2,700) 0.78 (8/1,021) 7.42 (69/930) 6.64 (4.96, 8.32) <0.001 89.49 (78.22, 94.97) <0.001 0.11 (0.05, 0.22) <0.001 9.09 (4.55, 20.00) <0.001 Q8. Is not playing with dogs a preventive measure for echinococcosis? Yes (correct) 93.30 (2,519/2,700) 96.57 (986/1,021) 90.32 (840/930) 6.25 (4.17, 8.33) <0.001 64.52 (43.02, 86.02) <0.001 No 4.04 (109/2,700) 2.84 (29/1,021) 4.84 (45/930) 2.00 (0.41, 3.59) 0.014 41.32 (8.97, 62.45) 0.014 0.59 (0.38, 0.91) 0.018 1.70 (1.10, 2.63) 0.018 Not sure 2.67 (72/2,700) 0.59 (6/1,021) 4.84 (45/930) 4.25 (2.85, 5.65) <0.001 87.81 (71.43, 94.74) <0.001 0.12 (0.05, 0.27) <0.001 8.26 (3.70, 20.00) <0.001 Q9. Is washing hands before meals a preventive measure for echinococcosis? Yes (correct) 96.56 (2,607/2,700) 99.41 (1,015/1,021) 90.65 (843/930) 8.76 (6.92, 10.60) <0.001 93.75 (74.07, 113.44) <0.001 No 1.22 (33/2,700) 0.49 (5/1,021) 5.16 (48/930) 4.67 (3.22, 6.12) <0.001 90.50 (77.91, 96.15) <0.001 0.09 (0.04, 0.23) <0.001 11.11 (4.35, 25.00) <0.001 Not sure 2.22 (60/2,700) 0.10 (1/1,021) 4.19 (39/930) 4.09 (2.94, 5.24) <0.001 97.61 (85.00, 99.85) <0.001 0.02 (0.00, 0.15) <0.001 50.00 (6.67, ∞)* <0.001 Total (Q1–Q9) Yes (correct) 84.85 (20,129/23,724) 91.35 (8,394/9,189) 84.57 (6,925/8,252) 6.78 (5.95, 7.61) <0.001 43.92 (40.23, 47.61) <0.001 Other responses (incorrect) 15.15 (3,595/23,724) 8.65 (795/9,189) 15.43 (1,327/8,252) 6.78 (5.95, 7.61) <0.002 43.92 (40.23, 47.61) <0.001 0.55 (0.51, 0.59) <0.001 1.82 (1.70, 1.96) <0.001 Abbreviation: ARR=absolute risk reduction; RR=relative risk; RRR=relative risk reduction; 1/RR=protective efficacy; CI=confidence interval; SHEPG=smart health education pillbox group; RHEG =routine health education group.
*For cells containing zero counts (Q5-No, Q9-Not sure), the Haldane-Anscombe correction was implemented by adding 0.5 to each cell. The RRR for Q5-No was set at 100% when the intervention group risk equaled 0; the corresponding CI was calculated using this correction.
†All responses were considered valid except for 576 logical errors in Q3 at baseline and 11, 14, and 93 logical errors in Q2, Q4, and Q5 in RHEG, respectively.
Note: Chi-square tests were employed for all comparisons; however, Fisher’s exact test was applied when the expected frequency of any cell fell below 5. Blank cells indicate values that were not calculated (with no need for calculation).Table 1. Knowledge rates from Baseline, SHEPG, and RHEG; ARR, RRR, RR, and 1/RR between SHEPG and RHEG after the 12-month follow-up, 2023–2024.
The attitude questionnaire evaluated participants’ willingness to adopt eight key control measures: handwashing, dog tethering, deworming, safe fecal disposal, centralized slaughtering, abstaining from feeding viscera to dogs, lamb vaccination, and health screening. Participants demonstrated overwhelmingly positive attitudes at all time points (Baseline: 89.97%; SHEPG: 91.76%; RHEG: 88.46%). One year post-initiation, SHEPG showed substantial improvements versus both controls. The absolute risk reduction was 3.30% (95% CI: 2.28–4.32; P<0.001) versus RHEG and 1.79% (95% CI: 0.95–2.63; P<0.0001) versus Baseline. These improvements corresponded to meaningful reductions in negative attitudes: RRR was 28.60% (95% CI: 19.76–37.38; P<0.001) versus RHEG and 17.85% (95% CI: 9.48–26.22; P<0.0001) versus Baseline. The RR of negative attitudes decreased to 0.71 (95% CI: 0.65–0.78; P<0.001) versus RHEG and 0.82 (95% CI: 0.76–0.89; P<0.0001) versus Baseline. Consequently, SHEP provided protective effects against unfavorable attitudes that were 1.40-fold (1/RR, 95% CI: 1.28–1.54; P<0.001) and 1.22-fold (1/RR, 95% CI: 1.12–1.32; P<0.0001) stronger than RHEG and Baseline, respectively (Table 2 and
Supplementary Table S3 ). Conversely, RHEG showed significant decline in positive attitudes (ARR=−1.51; 95% CI: −2.31 to –0.71; P=0.0002) with increased RR of 1.15 (95% CI: 1.07–1.24; P<0.0001) (Supplementary Table S4 ). SHEP acceptability among dog owners was high at 89.72% (916/1,021) (Q9, Table 2). Detailed attitude data for questions 1–8 are presented in Table 2 andSupplementary Tables S3–S4 .Question Response Baseline
[% (n/N)]SHEPG
[% (n/N)]CHEG
[% (n/N)]ARR RRR RR 1/RR 95% CI P 95% CI P 95% CI P 95% CI P Q1. Would you like to wash your hands before meals? Yes 97.30 (2, 627/2,700) 98.33 (1, 004/1,021) 97.74 (909/930) 0.59 (−0.49, 1.67) 0.288 25.93 (−21.67, 73.52) 0.288 No 2.70 (73/2,700) 1.67 (17/1,021) 2.26 (21/930) 0.59 (−0.49, 1.67) 0.288 26.11 (−21.74, 73.96) 0.288 0.74 (0.40, 1.37) 0.336 1.35 (0.73, 2.50) 0.336 Q2. Would you agree to tether all your dogs? Yes 95.63 (2, 582/2,700) 97.16 (992/1,021) 95.94 (803/837)* 1.22 (−0.40, 2.84) 0.137 29.76 (−9.76, 69.29) 0.137 No 4.37 (118/2,700) 2.84 (29/1,021) 4.06 (34/837)* 1.22 (−0.40, 2.84) 0.137 30.05 (−9.85, 69.95) 0.137 0.70 (0.44, 1.12) 0.139 1.43 (0.89, 2.27) 0.139 Q3. Would you agree to free regular dog deworming? Yes 97.22 (2, 625/2,700) 98.82 (1, 009/1,021) 98.17 (913/930)* 0.65 (−0.47, 1.77) 0.208 35.71 (−25.81, 97.22) 0.208 No 2.78 (75/2,700) 1.18 (12/1,021) 1.83 (17/930) 0.65 (−0.47, 1.77) 0.208 35.52 (−25.81, 97.22) 0.208 0.64 (0.32, 1.30) 0.218 1.56 (0.77, 3.13) 0.218 Q4. Would you agree to bury dog waste deeply after deworming? Yes 92.70 (2, 503/2,700) 96.38 (984/1,021) 92.95 (778/837)* 3.43 (1.37, 5.49) <0.001 48.57 (19.42, 77.72) <0.001 No 7.30 (197/2,700) 3.62 (37/1,021) 7.05 (59/837)* 3.43 (1.37, 5.49) <0.001 48.65 (19.42, 77.72) <0.001 0.51 (0.35, 0.75) <0.001 1.96 (1.33, 2.86) <0.001 Q5. Would you support centralized slaughter? Yes 49.74 (939/1, 888)* 61.76 (533/863)* 50.32 (419/852)* 11.44 (6.30, 16.58) <0.001 22.73 (12.52, 32.94) <0.001 No 50.26 (949/1, 888)* 38.24 (330/863)* 49.68 (433/852)* 11.44 (6.30, 16.58) <0.001 23.03 (12.68, 33.33) <0.001 0.77 (0.69, 0.86) <0.001 1.30 (1.16, 1.45) <0.001 Q6. Would you agree to free lamb vaccination? Yes 87.16 (1, 147/1, 316)* 88.02 (507/576)* 86.81 (553/637)* 1.21 (−2.78, 5.20) 0.490 8.75 (−20.08, 37.58) 0.490 No 12.84 (169/1, 316)* 11.98 (69/576)* 13.19 (84/637)* 1.21 (−2.78, 5.20) 0.490 9.17 (−21.08, 39.42) 0.490 0.91 (0.68, 1.21) 0.509 1.10 (0.83, 1.47) 0.509 Q7. Would you avoid feeding dogs raw livestock organs? Yes 86.86 (1, 342/1, 545)* 90.70 (634/699)* 85.53 (668/781)* 5.17 (1.66, 8.68) 0.001 35.71 (11.46, 59.96) 0.001 No 13.14 (203/1, 545)* 9.30 (65/699)* 14.47 (113/781)* 5.17 (1.66, 8.68) 0.001 35.73 (11.46, 59.96) 0.001 0.64 (0.49, 0.84) 0.001 1.56 (1.19, 2.04) 0.001 Q8. Would you agree to free regular check-ups (screening)? Yes 98.26 (2, 653/2,700) 98.33 (1, 004/1,021) 98.28 (914/930) 0.05 (−0.91, 1.01) 0.901 2.78 (−50.00, 55.56) 0.901 No 1.74 (47/2,700) 1.67 (17/1,021) 1.72 (16/930) 0.05 (−0.91, 1.01) 0.901 2.91 (−55.56, 55.56) 0.901 0.97 (0.50, 1.88) 0.929 1.03 (0.53, 1.99) 0.929 Q9. Would you use our Smart Health Education Pillbox? Yes N/A 89.72 (916/1,021)** N/A N/A N/A N/A N/A No N/A 10.28 (105/1,021)** N/A N/A N/A N/A N/A Total (Q1-8) Yes 89.97 (16, 418/18, 249) 91.76 (7, 583/8, 264) 88.46 (5, 957/6, 734) 3.30 (2.28, 4.32) <0.001 28.57 (19.76, 37.38) <0.001 No 10.03 (1, 831/18, 249) 8.24 (681/8, 264) 11.54 (777/6, 734) 3.30 (2.28, 4.32) <0.001 28.60 (19.76, 37.38) <0.001 0.71 (0.65, 0.78) <0.001 1.40 (1.28, 1.54) <0.001 Note: Chi-square tests were applied for all comparisons; however, Fisher's exact test was employed when the expected frequency of any cell fell below 5. Blank cells indicate “not calculated (with no need for calculation)”.
Abbreviation: ARR=absolute risk reduction; RR=relative risk; RRR=relative risk reduction; 1/RR=protective efficacy; CI=confidence interval; SHEPG=smart health education pillbox group; RHEG=routine health education group; N/A=not applicable.
* N=2,700 at baseline. At the one-year follow-up, SHEPG (N=1,021) and RHEG (N=930). Valid response counts in RHEG for Q2 and Q4 totaled 837. For Q5, valid response counts among households raising livestock were 1,888,863, and 852 across the three groups, respectively; for Q6, among households raising sheep, counts were 1,316,576, and 637, respectively; for Q7, among households raising livestock, counts were 1,545,699, and 781, respectively.
** The attitude survey regarding SHEP usage was administered exclusively in the SHEPG.Table 2. Attitude rates from Baseline, SHEPG, and RHEG; ARR, RRR, RR, and 1/RR between SHEPG and RHEG after the 12-month follow-up, 2023–2024.
The questionnaire evaluated dog owners’ adoption of recommended echinococcosis control practices. Correct practice rates remained low across all groups (SHEPG: 52.90%; RHEG: 45.40%; Baseline: 46.12%). SHEP intervention achieved significant improvements, with absolute increases of 7.50% over RHEG (ARR=7.50%, 95% CI: 5.96–9.04; P<0.001) and 6.78% over Baseline (ARR=6.78%, 95% CI: 5.35–8.21; P<0.001). These corresponded to relative reductions in incomplete compliance of 13.74% versus RHEG (RRR=13.74%, 95% CI: 10.91–16.56; P<0.001) and 12.58% versus Baseline (RRR=12.58%, 95% CI: 9.92–15.24; P<0.001). RR of “partly correct+incorrect” practices was significantly lower in SHEPG versus RHEG (RR=0.86, 95% CI: 0.84–0.89; P<0.001) and Baseline (RR=0.87, 95% CI: 0.85–0.90; P<0.001). SHEP participants were 1.16 times more likely to adopt correct practices than RHEG (1/RR=1.16, 95% CI: 1.14–1.19; P<0.001) and 1.15 times more likely than Baseline (1/RR=1.15, 95% CI: 1.11–1.18; P<0.001) (Table 3;
Supplementary Table S5 ). RHEG showed no significant changes versus Baseline (ARR=−0.72%, 95% CI: −1.70 to 0.26; P=0.150; RR=1.01, 95% CI: 0.99–1.04; P=0.180). Detailed responses are in Table 3 andSupplementary Table S5–6 .Question Response Baseline
[% (n/N)]SHEPG
[% (n/N)]CHEG
[% (n/N)]ARR RRR RR 1/RR 95% CI P 95% CI P 95% CI P 95% CI P 1. Do you wash your hands before meals? Three times a day or more (correct) 53.89 (1, 455/2,700) 59.94 (612/1,021) 54.73 (509/930) 5.21 (1.37, 9.05) 0.015 11.52 (3.03, 20.01) 0.015 1-2 times a day (partly) 23.96 (6, 47/2,700) 27.13 (277/1,021) 24.95 (232/930) −2.18 (−6.35, 1.99) 0.250 −8.74 (−25.45, 7.97) 0.250 1.09 (0.94, 1.26) 0.250 0.92 (0.79, 1.07) 0.250 Occasionally (incorrect) 22.15 (598/2,700) 12.93 (132/1,021) 20.32 (189/930) 7.39 (4.35, 10.43 ) <0.001 36.36 (21.41, 51.33) <0.001 0.64 (0.52-0.78, P<0.001) 1.57 (1.28, 1.92 ) <0.001 2. How is your dog typically restrained? Always tethered (correct) 27.89 (753/2,700) 31.73 (324/1,021) 28.84 (265/919) 2.89 (−0.97, 6.75) 0.150 4.06 (−1.36, 9.49) 0.150 Tethered during the day, free at night (partly) 14.96 (404/2,700) 13.22 (135/1,021) 14.79 (136/919) 1.57 (−2.18, 5.32) 0.330 10.62 (−14.74, 35.97) 0.330 0.89 (0.72, 1.11) 0.300 1.12 (0.90, 1.39) 0.300 Tethered in settlements, free during migration (partly) 47.78 (1, 290/2,700) 48.09 (491/1,021) 48.42 (445/919) 0.33 (−3.69, 4.35) 0.900 0.68 (−7.62, 8.98) 0.900 0.99 (0.90, 1.10) 0.90 1.01 (0.91, 1.11) 0.900 Never tethered (incorrect) 9.37 (253/2,700) 6.95 (71/1,021) 7.94 (73/919) 0.99 (−1.30, 3.28) 0.400 12.47 (−16.37, 41.31) 0.400 0.87 (0.65, 1.18) 0.380 1.15 (0.85, 1.55) 0.380 3. Do you often pet or hug your dog? Never (correct) 8.24 (175/2, 124) 10.19 (104/1,021) 9.25 (86/930) 0.94 (−1.96, 3.84) 0.480 1.04 (−2.16, 4.23) 0.480 Occasionally (partly) 53.95 (1, 146/2, 124) 52.69 (538/1,021) 53.01 (493/930) 0.32 (−3.71, 4.35) 0.880 0.60 (−7.00, 8.21) 0.880 0.99 (0.91, 1.09) 0.880 1.01 (0.92, 1.10) 0.880 Often (incorrect) 37.81 (803/2, 124) 37.12 (379/1,021) 37.74 (351/930) 0.62 (−3.73, 4.97) 0.750 1.64 (−9.88, 13.17) 0.750 0.98 (0.87, 1.11) 0.750 1.02 (0.90, 1.15) 0.750 4. Do you deworm your dog regularly? Yes (correct; 9-12 times/yr) 61.00 (1, 647/2,700) 91.38 (933/1,021) 59.89 (557/930) 31.49 (28.17, 34.81) <0.001 78.57 (70.15, 86.99) <0.001 Frequently (4-8 times/yr) (partly) 18.11 (489/2,700) 7.44 (76/1,021) 16.88 (157/930) 9.44 (6.67-12.21, P) <0.001 55.92 (39.51, 72.34) <0.001 0.44 (0.34, 0.57) <0.001 2.27 (1.75, 2.94 ) <0.001 Occasionally (1-3 times/year) (partly) 17.19 (464/2,700) 0.69 (7/1,021) 20.65 (192/930) 19.96 (18.06, 21.86) <0.001 96.66 (87.48, 105.83 ) <0.001 0.03 (0.02, 0.07) <0.001 33.33 (14.29, 50.00) <0.001 Never dewormed (incorrect) 3.70 (100/2,700) 0.49 (5/1,021) 2.58 (24/930) 2.09 (1.10, 3.08) <0.001 81.01 (42.64, 119.38 ) <0.001 0.19 (0.07, 0.50) <0.001 5.26 (2.00, 14.29 ) <0.001 5. Do you properly dispose of your dog's waste after deworming? Yes (correct; deep burial) 51.04 (1, 378/2,700) 54.65 (558/1,021) 51.73 (433/837) 2.92 (−1.34, 7.18) 0.180 6.06 (−2.78, 14.91) 0.180 Occasionally (partly) 21.81 (589/2,700) 25.17 (257/1,021) 21.39 (179/837) −3.78 (−7.80, 0.24) 0.052 −17.67 (−36.46, 1.12) 0.052 1.18 (1.00, 1.39) 0.052 0.85 (0.72, 1.00) 0.052 Untreated (incorrect) 27.15 (733/2,700) 20.18 (206/1,021) 26.88 (225/837) 6.70 (2.51, 10.89) <0.001 24.93 (9.34, 40.52) <0.001 0.75 (0.64, 0.88) <0.001 1.33 (1.14, 1.56) <0.001 6. Do you often slaughter cattle and sheep at home? No (correct) 18.17 (343/1, 888)* 19.00 (164/863)* 17.72 (151/852)* 1.28 (−2.97, 5.53) 0.480 7.22 (−16.76, 31.21) 0.480 Yes (incorrect) 81.83 (1, 545/1, 888)* 81.00 (699/863)* 82.28 (701/852)* 1.28 (−2.97, 5.53) 0.480 1.56 (−3.61, 6.72) 0.480 0.98 (0.94, 1.03) 0.480 1.02 (0.97, 1.06) 0.480 7. Do you feed the internal organs of the cattle and sheep to dogs? Never (correct) 61.04 (943/1, 545)* 67.81 (474/699)* 60.95 (476/781)* 6.86 (2.06, 11.66) 0.006 17.62 (5.29, 29.95) 0.006 Occasionally (partly) 25.18 (389/1, 545)* 22.03 (154/699)* 25.74 (201/781)* 3.71 (−0.70, 8.12) 0.100 14.41 (−2.72, 31.54) 0.100 0.86 (0.71, 1.03) 0.100 1.17 (0.97, 1.41) 0.100 Frequently (incorrect) 13.79 (213/1, 545)* 10.16 (71/699)* 13.32 (104/781)* 3.16 (−0.63, 6.95) 0.064 23.72 (−4.73, 52.18) 0.064 0.76 (0.58, 1.01) 0.058 1.32 (0.99, 1.72) 0.058 8. Are your lambs vaccinated regularly? Regularly (correct) 55.02 (724/1, 316)* 55.21 (318/576)* 54.79 (349/637)* 0.42 (−4.86, 5.70) 0.890 0.93 (−10.71, 12.57) 0.890 Irregularly (partly) 25.23 (332/1, 316)* 27.60 (159/576)* 26.06 (166/637)* −1.54 (−6.66, 3.58) 0.560 −5.91 (−25.56, 13.74) 0.560 1.06 (0.88, 1.27) 0.560 0.94 (0.79, 1.14) 0.560 No (incorrect) 19.76 (260/1, 316)* 17.19 (99/576)* 19.15 (122/637)* 1.96 (−2.38, 6.30) 0.37 10.24 (−12.43, 32.91) 0.37 0.90 (0.71, 1.14) 0.37 1.11 (0.88, 1.41) 0.37 9. Do you regularly participate in echinococcosis screening? Regularly (correct) 73.30 (1, 979/2,700) 86.68 (885/1,021) 74.30 (691/930) 12.38 (9.16, 15.60) <0.001 48.15 (35.67, 60.63) <0.001 Irregularly (partly) 24.04 (649/2,700) 12.83 (131/1,021) 24.84 (231/930) 12.01 (8.81, 15.21) <0.001 48.35 (35.47, 61.23 ) <0.001 0.52 (0.43, 0.62) <0.001 1.92 (1.61, 2.33) <0.001 No (incorrect) 2.67 (72/2,700) 0.49 (5/1,021) 0.86 (8/930) 0.37 (−0.37, 1.11) 0.32 43.02 (−43.02, 129.07) 0.320 0.57 (0.19, 1.71) 0.320 1.75 (0.59, 5.26) 0.320 Total (Q1-9) Correct 46.12 (9, 397/20, 373) 52.90 (4, 372/8, 264) 45.40 (3, 517/7, 746) 7.50 (5.96, 9.04) <0.001 13.74 (10.91, 16.56) <0.001 Partly correct+incorrect 53.88 (10, 976/20, 373) 47.10 (3, 892/8, 264) 54.60 (4, 229/7, 746) 7.50 (5.96, 9.04) <0.001 13.74 (10.91, 16.56) <0.001 0.86 (0.84, 0.89) <0.001 1.16 (1.14, 1.19) <0.001 Note: Chi-square tests were applied for all comparisons; however, Fisher's exact test was employed when the expected frequency of any cell fell below 5. Blank cells indicate “not calculated (with no need for calculation)”.
Abbreviation: ARR=absolute risk reduction; RRR=relative risk reduction; RR=relative risk; 1/RR=protective efficacy; CI=confidence interval; SHEPG=smart health education pillbox group; RHEG=routine health education group.
* N=2,700 at Baseline. At the one-year follow-up, SHEPG (N=1,021) and RHEG (N=930). Valid response counts for Q2 in RHEG totaled 919; for Q3 in Baseline, 2, 124; for Q5 in RHEG, 837. For Q6, among households raising livestock, counts across the three groups were 1, 888, 863, and 852, respectively; for Q7, among households raising livestock, counts were 1, 545, 699, and 781, respectively; for Q8, among households raising sheep, counts across the three groups were 1, 316, 576, and 637, respectively.Table 3. Practice rates from Baseline, SHEPG, and RHEG; ARR, RRR, RR, and 1/RR between SHEPG and RHEG after the 12-month follow-up, 2023–2024.
To quantitatively elucidate the knowledge-to-practice conversion mechanism, we developed a path model positing that knowledge (K) influences attitude (A), which shapes practices (P). Three parameters were defined: α (knowledge-to-attitude coefficient), representing attitude generated per unit knowledge (α=A/K); β (attitude-to-practice coefficient), representing practice generated per unit attitude (β=P/A); and η (conversion efficiency index), representing overall knowledge-to-practice efficiency (η=P / K=α × β). The derived formulae are: A=α × K, P=β × A=β × α × K. Results demonstrated superior attitude-to-practice conversion in SHEPG, with β=0.5765 (95% CI: 0.5642–0.5888) significantly exceeding RHEG (0.5132, 95% CI: 0.4999–0.5265) and Baseline (0.5126, 95% CI: 0.5046–0.5206). The β differences were substantial: Δβ=0.0633 for SHEPG versus RHEG and Δβ=0.0639 for SHEPG versus Baseline (all P<0.0001). SHEPG achieved relative increases in conversion efficiency of 7.88% (0.0423/0.5368) versus RHEG and 6.55% (0.0356/0.5435) versus Baseline, demonstrating greater overall efficiency in translating knowledge into practice (all P<0.0001) (Table 4–5). Conversely, RHEG showed only a 1.23% (0.0067/0.5435) increase in conversion efficiency versus Baseline, which was not statistically significant (Z=0.799, P=0.424) (Table 4–5).
Group K A P α (95% CI) β (95% CI) η (95% CI) SHEPG 0.9135 0.9176 0.5290 1.0045 (0.9954, 1.0136) 0.5765 (0.5642, 0.5888) 0.5791(0.5668, 0.5914) RHEG 0.8457 0.8846 0.4540 1.046 (1.0328, 1.0592) 0.5132 (0.4999, 0.5265) 0.5368 (0.5228, 0.5508) Baseline 0.8485 0.8997 0.4612 1.0603 (1.0526, 1.0680) 0.5126 (0.5046, 0.5206) 0.5435 (0.5349, 0.5521) Abbreviation: K=knowledge; A=attitude; P=practice; α=knowledge-to-attitude coefficient; β=attitude-to-practice coefficient; η=conversion efficiency index; CI=confidence interval; SHEPG=smart health education pillbox group; RHEG=routine health education group. Table 4. The K, A, P, α, β, and η across SHEPG, RHEG, and Baseline after the 12-month follow-up, 2023–2024.
Group Δα Z (P) Δβ Z (P) Δη Z (P) SHEPG vs. RHEG −0.0415 −5.08 (<0.001) 0.0633 6.85 (P<0.001) 0.0423 5.32 (<0.001) SHEPG vs. Baseline −0.0558 −9.21 (<0.001) 0.0639 8.53 (<0.001) 0.0356 4.87 (<0.001) RHEG vs. Baseline 0.0143 1.835 (0.067) −0.0006 −0.0758 (0.940) 0.0067 0.799 (0.424) Note: To maintain consistency across all comparisons, data in this table are retained to four decimal places because Δβ in RHEG versus Baseline equals −0.0006.
Abbreviation: Δα=difference in knowledge-to-attitude conversion coefficients between groups; Δβ=difference in attitude-to-practice conversion coefficients between groups; Δη=difference in conversion efficiency index between groups; Z=Z-test statistic; SHEPG=smart health education pillbox group; RHEG=routine health education group.Table 5. The Δα, Δβ, and Δη across SHEPG, RHEG, and Baseline after the 12-month follow-up, 2023–2024.
-
The SHEP represents an innovative integration of artificial intelligence and Internet of Things technologies for echinococcosis control, transitioning from RHE to precision-targeted interventions. Its core functionalities include: 1) Systematic Knowledge Delivery: Prerecorded messages broadcast at predetermined intervals (at least three times daily, exceeding 1,095 times annually) strengthen policy comprehension and promote sustained behavioral change. 2) Automated Deworming Reminders: Audio and visual alerts prompt dog owners on scheduled deworming days, enhancing compliance and reducing missed treatments. 3) Precision Targeting: Distribution specifically to dog owners — the primary target population — enables efficient, focused educational outreach and practice promotion. 4) Cultural Adaptability: Multilingual modules (Standard Chinese, Tibetan, Uyghur, Kazakh, and others) ensure accessibility across diverse endemic regions, overcoming literacy barriers through audio-based communication. 5) Technical Reliability: With six-month battery life, compact design, and portability, the platform supports continuous education during pastoral migrations and in remote pasturages, addressing “last-mile” challenges in disease control programs. 6) Dedicated Bait Storage: A secure compartment protects anthelmintic baits, resolving storage challenges.
The 12-month SHEP implementation resulted in substantial improvements in echinococcosis-related knowledge. The SHEPG demonstrated significantly higher overall correct response rates compared to both RHEG and Baseline (Table 1 and
Supplementary Table S1 ). These enhancements were particularly notable across key knowledge domains, validating SHEP’s effectiveness as a persistent, interactive tool that reinforces essential health messages and surpasses the less engaging, one-time RHE. The intervention effectively dispelled misconceptions and reduced uncertainty (Table 1 andSupplementary Table S1 ). Additionally, SHEP demonstrated significant protective value by countering the observed decline in correct response rates on several crucial questions (e.g., Q7, Q8, Q9) within the RHEG, preventing knowledge deterioration and emergence of new misconceptions over time (Table 1 andSupplementary Table S1 ). Comparison of RHEG to Baseline revealed minimal knowledge improvement; the overall knowledge rate showed no statistically significant change (Table 1 andSupplementary Table S2 ). These findings suggest that routine, one-time health education is inadequate for consolidating and retaining complex knowledge over time and may prove ineffective against knowledge erosion or misinformation spread without sustained, reinforced messaging.The SHEP intervention notably influenced dog owners’ attitudes, as evidenced in Table 2 and
Supplementary Table S3 . The 3.30% increase in ARR confirmed SHEP’s effectiveness in disseminating information and positively shaping behavioral intentions. The 28.57% reduction in risk of negative attitudes demonstrated that the intervention strengthened positive intentions while mitigating resistance and hesitancy (P<0.001). Significant improvements were observed in key practice-related attitudes, including proper burial of dog waste (Q4), support for centralized slaughter (Q5), and avoidance of feeding raw viscera to dogs (Q7). All changes were statistically significant (P<0.001) and critical for interrupting the parasite’s transmission cycle (Table 2). Furthermore, 89.72% of SHEPG participants expressed willingness to use the smart pillbox (Q9), indicating high acceptability of this innovative technology and promising potential for large-scale implementation.The ultimate measure of an intervention’s effectiveness lies in its capacity to transform knowledge and attitudes into meaningful behavioral change. Our analysis of conversion efficiency quantified the SHEP’s impact across the knowledge-attitude-practice pathway (Table 4). This study revealed a persistent disconnect between high knowledge levels (Table 1) and positive attitudes (SHEPG, 91.76%; RHEG, 88.46%; Baseline, 89.97%; Table 2), contrasted with substantially lower adoption of recommended practices (SHEPG, 52.90%; RHEG, 45.40%; Baseline, 46.12%; Table 3). This pattern underscores the challenge of bridging the knowledge-attitude-practice gap in health education interventions. The SHEP intervention successfully addressed this challenge, markedly enhancing participants’ ability to translate positive attitudes into concrete actions. The device functioned as a behavioral facilitator, narrowing the knowledge-attitude-practice gap by delivering timely cues and reminders while simplifying execution of desired practices, such as adherence to deworming schedules.
This study has limitations warranting consideration. The 1-year follow-up period is brief for evaluating long-term sustainability of behavioral changes. The outcomes relied on self-reported data, susceptible to social desirability bias, recall bias, and cultural influences. Additionally, SHEP effectiveness may be constrained by inadequate internet connectivity in remote pastoral areas. Future research should prioritize scaling up the SHEP intervention and integrating it with complementary veterinary and public health measures to achieve synergistic effects in echinococcosis control.
In conclusion, the SHEP’s demonstrated efficacy and high acceptability among dog owners support its integration into national public health strategies for sustainable control of echinococcosis and other zoonotic diseases.
-
The support and collaboration of the Shangri-La CDC, Xiji County CDC, Emin County CDC, Hejing County CDC, Artux City CDC, Yushu Tibetan Autonomous Prefecture CDC, Qapqal Xibe Autonomous County CDC, and the CDC of the Fourth Division of Xinjiang Production and Construction Corps. We extend our sincere appreciation to all study participants for their valuable contributions to this research.
-
Approval by the National Institute of Parasitic Diseases, China CDC (Ethical Review Committee No. 2021019).
HTML
| Citation: |

|