
 Download:
Download:




-
Introduction: Human immunodeficiency virus (HIV) and hepatitis C virus (HCV) represent two major public health threats worldwide. However, the impact of HCV co-infection on HIV antiretroviral therapy (ART) outcomes remains debated.
Methods: Using data from the National Free Antiretroviral Treatment Program database, we employed stratified matching methods to extract two cohorts: HIV/HCV co-infected individuals and HIV mono-infected individuals. We compared differences in their ART outcomes — mortality, virological failure, and attrition — through stratified Cox regression and conditional logistic regression analyses.
Results: A total of 10,953 HIV/HCV co-infected and 17,348 HIV mono-infected individuals were included. Across all baseline CD4 strata, HIV/HCV co-infected individuals demonstrated a significantly higher risk of mortality, virological failure, and attrition compared to HIV mono-infected individuals. The risks were highest for all ART outcomes in the group with a baseline CD4 count of 200–349 cells/μL.
Conclusion: Given the adverse impact of HCV co-infection on treatment outcomes among people living with HIV (PLWH), enhanced prevention, screening, and management (including treatment) of HCV within PLWH should be prioritized and strengthened as part of routine clinical care.
-
The epidemics of human immunodeficiency virus (HIV) and hepatitis C virus (HCV) continue to impose substantial disease burdens worldwide (1–2), with both viruses facing the goal of ending epidemics and eliminating public health threats by 2030 (3–4). Due to similar transmission pathways, people living with HIV (PLWH) are prone to co-infection with HCV (5–6). However, evidence regarding the impact of HCV co-infection on antiretroviral therapy (ART) outcomes in PLWH remains debated across studies (7–8), and high-quality evidence to guide clinical practice is lacking. To address this knowledge gap, we utilized nearly two decades of national ART data to investigate how HCV co-infection may influence ART outcomes in PLWH.
We conducted a retrospective cohort study using the National Free Antiretroviral Treatment Program database, with follow-up extending from ART initiation through December 31, 2023. This database provided comprehensive, long-term, real-world data that accurately captured the complete treatment trajectory for PLWH. Participant inclusion criteria were: 1) age ≥18 years; 2) HBsAg negative; 3) ART initiation before 2023; and 4) availability of baseline CD4 count. Participants were stratified by baseline CD4 count into four groups: 0–199, 200–349, 350–499, and ≥500 cells/μL. Within each stratum, we performed individual matching, pairing HIV/HCV co-infected individuals with HIV mono-infected individuals. To enhance study efficiency, we applied a 1:2 matching ratio for the CD4 count strata of 0–199 and 200–349 cells/μL; for the remaining two strata with relatively fewer participants, we adopted a 1:1 matching ratio. Based on previous research identifying major factors influencing HIV treatment outcomes, matching variables included sex, ART initiation date, ART initiation institution, ART regimen, and age (8–9) (
Supplementary Figure S1 ). Unmatched individuals were excluded from the analysis. Due to limited availability of HCV-RNA data in the database, anti-HCV positivity served as the indicator of HCV infection in this study. Consequently, we were unable to distinguish between past and active HCV infection. We assessed three outcomes: mortality (all-cause mortality), virological failure (viral load >400 copies/mL after 6 months of ART), and attrition (including death, loss-to-follow-up, and treatment withdrawal). We evaluated the association between HCV seropositivity and both mortality and virological failure using stratified Cox regression models, while conditional logistic regression was applied to assess attrition due to its composite nature. Since major confounding factors influencing HIV treatment outcomes were controlled through stratification and matching, HCV status served as the sole covariate in both the Cox and logistic regression models. In sensitivity analyses, we redefined virological failure using different viral load thresholds (>50, >400, and >1,000 copies/mL) within the stratified Cox regression framework. All statistical analyses were performed using SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA), with statistical significance defined as P<0.05.This study included 10,953 HIV/HCV co-infected and 17,348 HIV mono-infected individuals. The two groups demonstrated excellent comparability, with well-balanced distributions of sex, ART initiation date, ART initiation institution, ART regimen, and age across all baseline CD4 cell count strata (Table 1). Across all baseline CD4 strata, HIV/HCV co-infected individuals exhibited a higher proportion of adverse ART outcomes compared to HIV mono-infected individuals, and both Cox and logistic regression analyses confirm the significance of this difference (
Supplementary Table S1 , Figure 1). When comparing co-infected to mono-infected groups, the odds ratio for attrition was lowest in the ≥500 cells/μL stratum (1.42) and highest in the 200–349 cells/μL stratum (1.92). Correspondingly, the hazard ratios for virological failure were 1.20 and 1.47, while those for death were 1.44 and 2.13, respectively. All differences achieved statistical significance (Figure 1). The effect size of HCV co-infection on ART outcomes varied substantially across baseline CD4 strata, with the highest risks for all outcomes observed in the group with baseline CD4 counts of 200–349 cells/μL.Baseline characteristics Baseline CD4: 0–199 cells/μL Baseline CD4: 200–349 cells/μL Baseline CD4: 350–499 cells/μL Baseline CD4: ≥500 cells/μL HIV/HCV
(N=3,793, %)HIV
(N=7,586, %)HIV/HCV
(N=2,602, %)HIV
(N=5,204, %)HIV/HCV
(N=2,783, %)HIV
(N=2,783, %)HIV/HCV
(N=1,775, %)HIV
(N=1,775, %)Gender Male 3,169 (83.5) 6,338 (83.5) 2,015 (77.4) 4,030 (77.4) 2,188 (78.6) 2,188 (78.6) 1,407 (79.3) 1,407 (79.3) Female 624 (16.5) 1,248 (16.5) 587 (22.6) 1,174 (22.6) 595 (21.4) 595 (21.4) 368 (20.7) 368 (20.7) Initial ART age (IQR) 40.6 (35.1, 46.7) 40.7 (35.2, 46.8) 37.7 (31.8, 44.2) 37.8 (31.8, 44.2) 36.2 (31.1, 42.3) 36.2 (30.8, 42.5) 35.2 (30.0, 41.1) 35.3 (29.9, 41.0) Initial ART sites General hospitals 1,665 (43.9) 3,330 (43.9) 1,442 (55.4) 2,884 (55.4) 1,876 (67.4) 1,876 (67.4) 1,286 (72.5) 1,286 (72.5) Infectious disease hospitals 1,798 (47.4) 3,596 (47.4) 977 (37.5) 1,954 (37.5) 628 (22.6) 628 (22.6) 318 (17.9) 318 (17.9) Community clinics 47 (1.2) 94 (1.2) 51 (2.0) 102 (2.0) 109 (3.9) 109 (3.9) 77 (4.3) 77 (4.3) Other sites 283 (7.5) 566 (7.5) 132 (5.1) 264 (5.1) 170 (6.1) 170 (6.1) 94 (5.3) 94 (5.3) Initial ART date 2002–2009 95 (2.5) 190 (2.5) 49 (1.9) 98 (1.9) − − − − 2010–2014 1,411 (37.2) 2,822 (37.2) 976 (37.5) 1,952 (37.5) 884 (31.8) 884 (31.8) 449 (25.3) 449 (25.3) 2015–2019 1,657 (43.7) 3,314 (43.7) 1,220 (46.9) 2,440 (46.9) 1,511 (54.3) 1,511 (54.3) 1,074 (60.5) 1,074 (60.5) 2020–2022 630 (16.6) 1,260 (16.6) 357 (13.7) 714 (13.7) 388 (13.9) 388 (13.9) 252 (14.2) 252 (14.2) Initial ART regimens AZT/D4T+3TC+NVP/EFV 930 (24.5) 1,860 (24.5) 693 (26.6) 1,386 (26.6) 495 (17.8) 495 (17.8) 184 (10.4) 184 (10.4) TDF+3TC+NVP/EFV 2,691 (70.9) 5,382 (70.9) 1,858 (71.4) 3,716 (71.4) 2,208 (79.3) 2,208 (79.3) 1,519 (85.6) 1,519 (85.6) AZT/TDF+3TC+DTG/LPV/r 87 (2.3) 174 (2.3) 32 (1.2) 64 (1.2) 62 (2.2) 62 (2.2) 57 (3.2) 57 (3.2) Other regimens 85 (2.2) 170 (2.2) 19 (0.7) 38 (0.7) 18 (0.6) 18 (0.6) 15 (0.8) 15 (0.8) Abbreviation: HIV=human immunodeficiency virus; HCV=hepatitis C virus; CD4=cluster of differentiation 4 T-lymphocyte; ART=antiretroviral therapy; IQR=interquartile range; AZT=zidovudine; D4T=stavudine; 3TC=lamivudine; NVP=nevirapine; EFV=efavirenz; TDF=tenofovir; DTG=dolutegravir; LPV/r=lopinavir/ritonavir. Table 1. Baseline characteristics of HIV/HCV co-infected and HIV mono-infected individuals by baseline CD4 count.
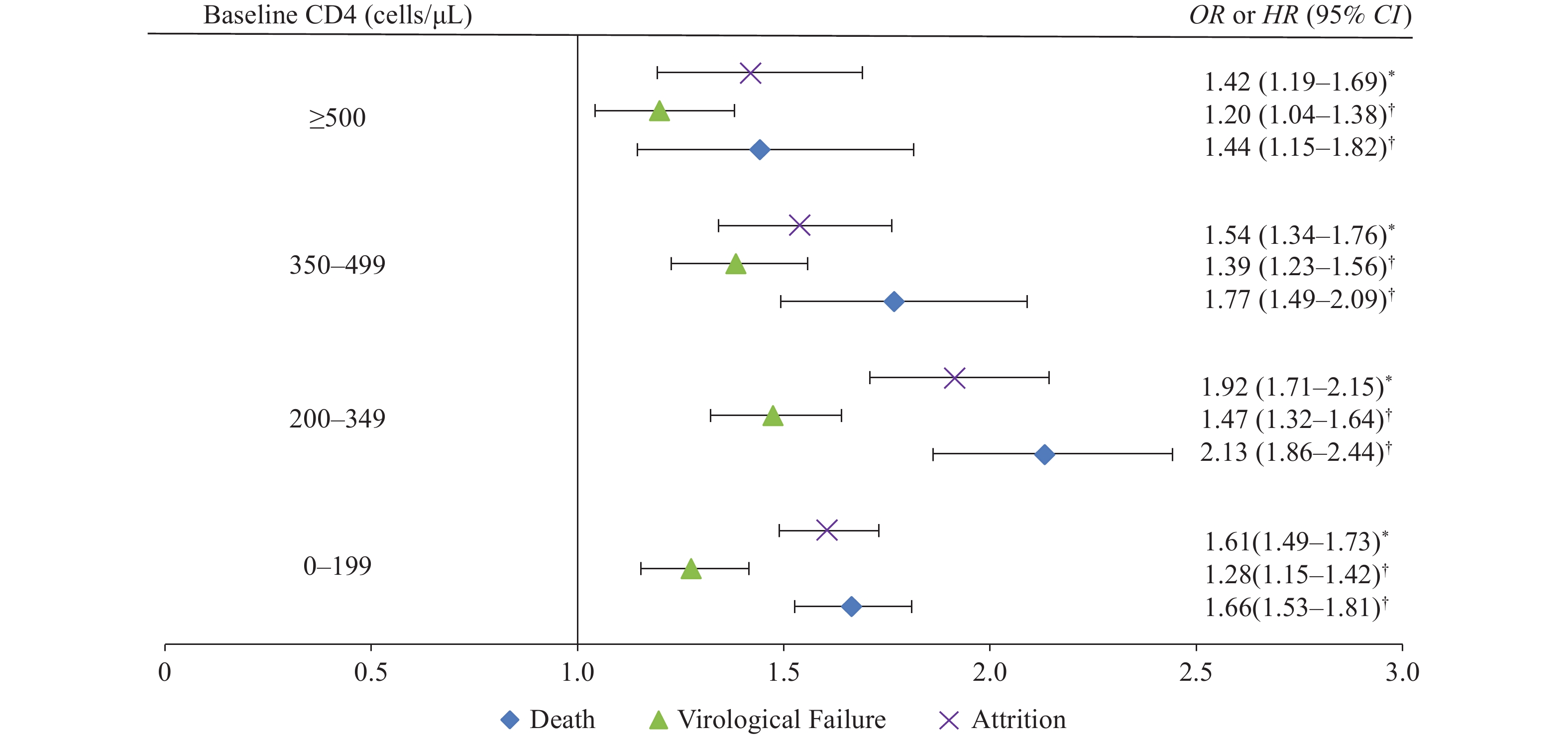 Figure 1.
Figure 1.Impact of hepatitis C virus co-infection on antiretroviral therapy outcomes in people living with HIV.
Abbreviation: OR=odds ratio; HR=hazard ratio; CD4=cluster of differentiation 4 T-lymphocyte; HIV=human immunodeficiency virus.Sensitivity analysis revealed a consistent pattern in which HCV co-infection remained associated with an increased risk of virological failure across subgroups. Hazard ratio values ranged from 1.10 to 1.47, with the exception of one subgroup characterized by a baseline CD4 count ≥500 cells/μL and a viral load threshold >50 copies/mL. The results achieved statistical significance in the remaining 11 subgroups (Figure 2).
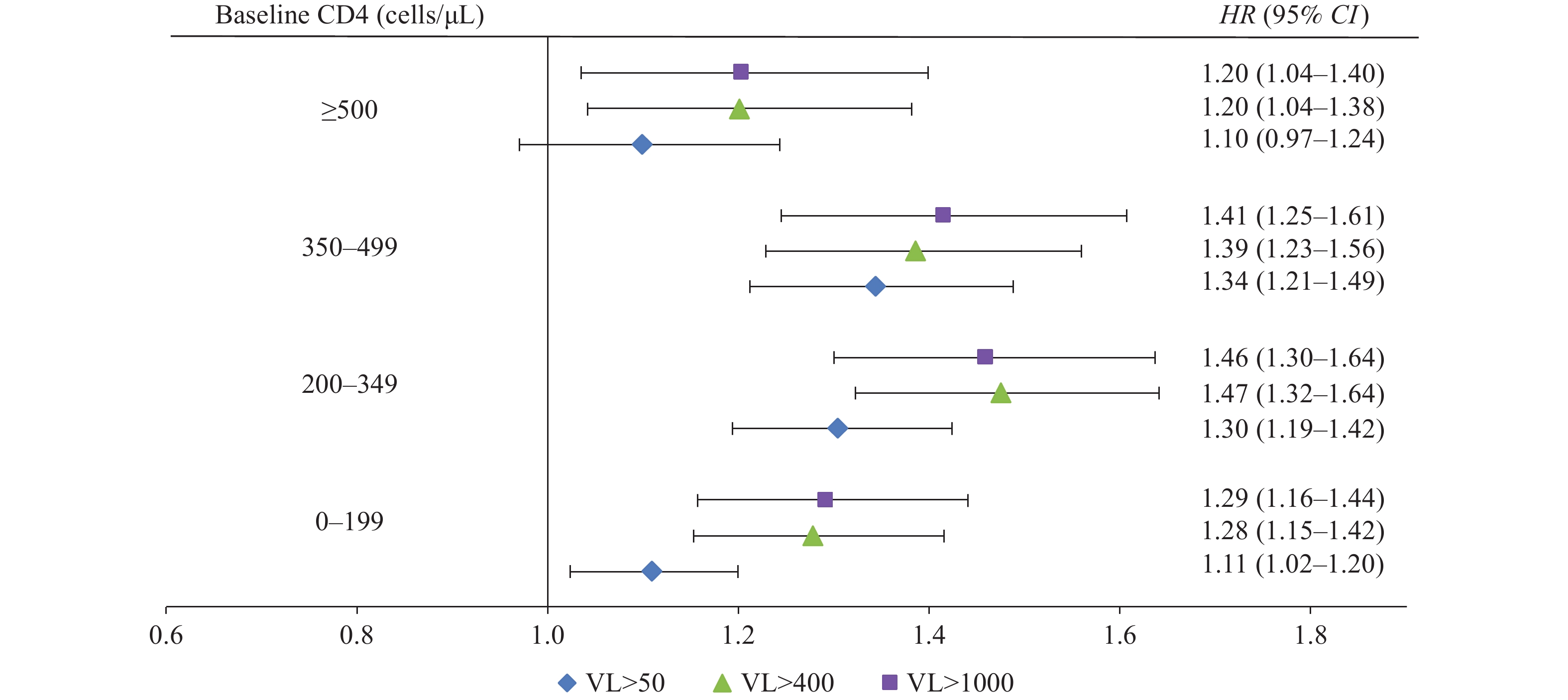 Figure 2.
Figure 2.Sensitivity analysis of hepatitis C virus co-infection on virological failure in people living with HIV.
Abbreviation: VL=HIV viral load; HR=hazard ratio; CD4=cluster of differentiation 4 T-lymphocyte; HIV=human immunodeficiency virus. -
This nationwide cohort study, spanning two decades and encompassing over 28,000 participants, demonstrates that HCV co-infection significantly increases the risks of death, virological failure, and attrition among PLWH. The elevated risk was most pronounced in individuals with baseline CD4 counts of 200–349 cells/μL. Our findings regarding mortality and attrition align with both domestic and international research. However, some studies have reported no significant difference in virological failure risk between HIV/HCV co-infected and HIV mono-infected individuals — discrepancies that may stem from variations in study populations, follow-up duration, and analytical approaches (8,10). The effect magnitude of HCV co-infection on treatment outcomes varied across baseline CD4 strata, with the strongest associations observed in the 200–349 cells/μL group. Furthermore, sensitivity analyses confirmed the robustness of the relationship between HCV co-infection and virological response, consistently demonstrating elevated failure risk among co-infected individuals across different viral load thresholds.
This study leverages large-scale real-world data from the nationwide ART database. Through rigorous study design, we employed stratification and matching methods to balance major confounding factors — rather than relying solely on statistical adjustments — and carefully selected eligible, high-quality data to construct two comparable observational cohorts. This methodology enables relatively precise estimation of the “net effect” of HCV co-infection on HIV treatment outcomes. Although observational studies cannot control all potential confounders with the same rigor as a two-arm randomized controlled trial (RCT), our approach represents an innovative strategy to enhance research efficiency by controlling major confounders through thoughtful study design. This is particularly valuable given that conducting an RCT to evaluate the impact of HCV co-infection on HIV outcomes would be neither ethical nor feasible.
Several limitations warrant consideration. First, the absence of HCV-RNA testing data prevented us from distinguishing between active and resolved HCV infections. Anti-HCV positivity, which encompasses both HCV-RNA negative and HCV-RNA positive individuals, may attenuate the observed impact of active HCV infection on adverse ART outcomes. Second, HCV treatment status can influence HIV treatment outcomes, but we were unable to analyze this variable due to its absence from our database. Third, as a retrospective observational study, we could not control for all possible residual confounders (e.g., tuberculosis co-infection, liver disease severity, socioeconomic factors). Nevertheless, by employing stratification and matching in our study design, we successfully controlled for major confounding factors. In the absence of available RCTs, this study represents a valuable contribution to understanding HCV’s impact on HIV treatment outcomes.
In conclusion, given the substantial negative impact of hepatitis C virus co-infection on antiretroviral therapy outcomes among people living with human immunodeficiency virus, enhanced prevention, screening, and comprehensive management (including treatment) of hepatitis C virus infection within this population should be prioritized and strengthened as an integral component of routine clinical care.
-
All individuals involved in data collection and management.
-
Approved by the Institutional Review Board of the National Center for AIDS/STD Control and Prevention, Chinese Center for Disease Control and Prevention (X191030594).
HTML
| Citation: |

|