
 Download:
Download:




-
The rabies virus belongs to the Rhabdoviridae family and Lyssavirus genus and causes the fatal zoonotic disease, rabies (1). Once the symptoms of rabies appear, the fatality rate is 100%. Globally, an estimated 59,000 people die from rabies each year, with the majority of cases occurring in Asia and Africa (2). Effective prevention of rabies relies on timely vaccination, which is both a core component of post-exposure prophylaxis (PEP) and an important measure for pre-exposure immunization in high-risk populations (3).
Following rabies vaccination, a serum rabies virus neutralizing antibody titer of at least 0.5 IU/mL is considered indicative of an adequate immune response for effective protection (4-5). Serological testing is crucial for assessing the immunogenicity of rabies vaccines and for verifying protective antibody levels in vaccinated individuals. Of the existing testing methods, rapid fluorescent focus inhibition test (RFFIT) is considered the gold standard for the quantitative detection of rabies virus neutralizing antibodies (RVNA) (6).
RFFIT is a cell-based viral neutralization assay widely used to evaluate the biological efficacy of rabies vaccines and determine protective antibody levels in humans and animals. However, the complex analytical procedures of the assay may be affected by multiple factors, including cell line growth, reagent batch variations, and sample quality (7–8). A comprehensive validation of RFFIT was conducted in this study and confirmed RFFIT to be a reliable and standardized testing tool suitable for the serological surveillance and immunological assessment of rabies.
HTML
-
Fifty serum samples were prepared. 20 RVNA-positive serum samples (RVNA ≥0.5 IU/mL), 20 corresponding 1∶10 diluted RVNA-positive samples, and 10 RVNA-negative samples (
Supplementary Table S1 ). Negative samples were obtained from pooled human serum. The RVNA-positive samples were prepared by mixing the third World Health Organization international standard for anti-rabies immunoglobulin (WHO-3 SRIG) (164 IU/mL) with pooled human serum. All samples were heat inactivated at 56 °C for 30 min prior to use.In this study, the number of samples in the different serum groups aimed to efficiently use limited standard and serum matrices while covering all necessary concentration ranges. This approach also simulated the distribution of antibodies in real-world scenarios. Following vaccination, antibody levels in most individuals cluster within the low-to-moderate concentration range (close to the 0.5 IU/mL threshold). The validation results accurately reflected real-world testing scenarios by allocating more replicate samples to common concentrations, thereby enabling a more representative assessment of the reliability of the method.
-
The BSR cells are a clone of hamster kidney cells (BHK-21). BSR cells were maintained in Dulbecco’s modified Eagle’s medium (DMEM; Gibco, Cat. 11965092) supplemented with 10% fetal bovine serum (FBS; Gibco, Cat. 10091-148), 1% Penicillin–Streptomycin at 37 °C in a 5% CO2 atmosphere. The challenge virus standard (CVS)-11 is a fixed strain that serves as an international standard challenge virus for rabies.
-
Heterologous virus antigens were provided by Sinovac, China: Hepatitis A (38,355 U/mL, Batch No. 01-E2108-012); H1N1 flu (434 μg/mL, Batch No. A1-2205-037-SD); and EV71 (340 U/μg, Batch No. 08-E2111-006).
-
Pooled human serum was donated by volunteers at Synermore, all confirmed to be without a history of rabies virus exposure and with an RVNA titer of <0.5 IU/mL. A total of 13 individual serum samples were pooled and stored at −75±15 °C.
-
A 2% hemolytic matrix was prepared by mixing a hemolysis blood collection with an RVNA-negative whole blood sample. A lipemic matrix, a stock solution of 200 mg/mL triglycerides, was first prepared from glycerol trioleate (Aladdin, Catalog No. G105172-1g). The lipemic matrix, which contained 4.0 mg/mL triglycerides, was achieved by mixing the stock solution with the pooled human serum. The icteric matrix was formed by mixing 200 mg/L bilirubin with the pooled human serum (final concentration of bilirubin was 34.2 μmol/L; bilirubin was from MeilunBio, Dalian, China; Catalog No. MB1035-1).
-
WHO-3 SRIG (Cat. No. 19/244, 164 IU) was diluted to 54.6667 IU/mL according to the manufacturer’s instructions, and was used as a calibrator to calculate the RVNA titers (IU/mL) in the test serum samples.
-
The RFFIT procedure (9–10) was used to measure the level of RVNA against the CVS-11 strain of rabies virus in the serum samples. Heat-inactivated serum samples were serially diluted in a three-fold series and incubated with the CVS-11 strain in 96-well tissue culture plates at 37 °C for 60 min.
BSR cells were then added to the serum–virus mixture and incubated for an additional 24 h at 37 °C in a 5% CO2 environment. The culture plates were fixed with acetone and stained with an anti-rabies N-FITC (fluorescein isothiocyanate) conjugate. Observation was conducted using a fluorescence microscope (IX2-ILL100, Tokyo, Japan, Olympus), and the percentage of infected cells was estimated by the reader; the percentage within two wells was recorded before and after 50% of the cells were infected. Finally, the Reed–Muench method (11) was applied to calculate the 50% end-point titer using the percentage of infected values.
-
The validation plan was based on the Food and Drug Administration (FDA) Guidance for Industry (12) and International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Q2 (R1) guidelines (13), considering the limitations and variability of cell-based virus neutralization assays. The FDA and ICH guidelines recommend a coefficient of variation (CV) of 15%–20% as the acceptance criterion for precision and accuracy in analytical method validation (12). However, the WHO notes that cell-based assays are expected to have a much higher CV (14). The RFFIT is a bioassay. Therefore, this RFFIT validation, a geometric coefficient of variation (GCV) of ≤30% was implemented. The validation parameters and acceptance criteria are listed in Table 1.
Validation parameter Acceptance criterion Remark Intra-assay precision
(repeatability)GCV ≤30% Criteria adjusted to cell-based assay performance Intermediate precision GCV ≤30% Criteria adjusted to cell-based assay performance Dilutability ≥80% samples show ≤30% GMC difference compared to undiluted control samples Determination of range
(LLOQ, LLD, and ULOQ)LLOQ: GCV ≤30% Criteria adjusted to cell-based assay performance Linearity Linear regression slope must be 0.80–1.25
R2 must be ≥0.95Accuracy 80% of the spiked SRIGs with results ≥LLOQ, with 70%–130% recovery of SRIG Accuracy criteria should be met for the samples near the LLOQ level Specificity-competition studies (1) High-titer samples: Dose-dependent inhibition observed; ≥80% titer drop at highest concentration
(2) Low-titer samples: Titer <LLOQ at highest concentration
(3) Titer drop ≤30% vs. no-competition control(1)(2) Applicable to competition with homologous antigens
(3) Applicable to competition with heterologous antigensSpecificity - matrix effect ≥80% of matrix samples differed by ≤30% Compared with normal serum Robustness RVNA titer differences within ±30% under varied conditions Stability RVNA titer differences are within ±30% Abbreviation: RFFIT=rapid fluorescent focus inhibition test; RVNA=rabies virus neutralizing antibodie; GCV=geometric coefficient of variation; GMC=geometric mean concentration; LLOQ=lower limit of quantification; LLD=lower limit of detection; ULOQ=upper limit of quantification; WHO-3 SRIG=third World Health Organization international standard for anti-rabies immunoglobulin. Table 1. Validation parameters and acceptance criteria for the RFFIT for quantifying RVNA.
-
Precision was evaluated at two levels: intra-assay precision (repeatability) and intermediate precision. Precision and dilutability were evaluated using the same set of 50 serum samples and analyzed in triplicate in six independent assay runs by two qualified analysts.
-
The WHO-3 SRIG was serially diluted 23- to 212-fold to obtain concentrations from 20.5 to 0.0400 IU/mL. These dilutions were spiked into undiluted RVNA-negative serum samples to produce six concentrations: ULOQ 20.5 IU/mL, high quality control (HQC) 10.25 IU/mL, medium quality control (MQC) 2.5625 IU/mL, low quality control (LQC) 0.6406 IU/mL, LLOQ 0.0801 IU/mL, and LLD 0.0400 IU/mL. Each level was tested individually across six independent runs by two qualified analysts in triplicate for each run.
-
Specificity was evaluated using antigen competition and matrix effect studies. For competition studies, 7 RVNA-positive samples (4 at 5.125 IU/mL and 3 at 2.5625 IU/mL) were pre-incubated separately with 5 serial 2-fold dilutions of homologous inactivated rabies virus (PV2061, Speeda, Chenda Bio, Liaoning, China), inactivated heterologous viruses (Hepatitis A virus, H1N1 influenza virus, and Enterovirus 71), and assay medium (baseline control).
For the matrix effect studies, 10 RVNA-positive samples (2 at 10.25 IU/mL, 4 at 5.125 IU/mL, 4 at 2.5625 IU/mL) were spiked in a 1:1 ratio with hemolytic, lipemic, and icteric matrices, and RVNA-negative serum (baseline).
-
Robustness was assessed by varying the assay conditions for the RVNA titers. The impact of the BSR cells was evaluated by the percentage difference in the RVNA titer (5.125 IU/mL) from different BSR passages (P20, P30, P40, P60, P70, and P80). Additionally, BSR cells were inoculated and passaged every 2 or 3 days, and RFFIT tests were performed using 10 RVNA positive samples (4 of 5.125 IU/mL, 4 of 2.5625 IU/mL and 2 of 1.2813 IU/mL).
Further robustness testing was conducted using different batches and suppliers of the anti-rabies N-FITC conjugates and DMEM. The impact of reagent variation was assessed by comparing the RVNA titers (5.125 IU/mL) obtained from each batch/supplier. The assay was evaluated under various critical conditions.
-
The short-term stability of rabies virus, serum samples, and WHO-3 SRIG was assessed under various conditions. Serum samples (5.125 IU/mL) were assessed following 5 freeze–thaw cycles, and after 24 h, 1 w, and 4 w of storage at 4 °C, and after 4 h at room temperature (20–25 ℃). The WHO-3 SRIG was assessed following 5 freeze–thaw cycles. The rabies virus stability was evaluated after 15 min at room temperature before use.
Serum Samples
Cells and Rabies Virus
Heterologous Virus Antigens
Pooled Human Sera
Matrix Sera
Standard for Anti-Rabies Immunoglobulin
RFFIT Protocol
RFFIT Validation
Precision and dilutability.
Accuracy, linearity, and range.
Specificity.
Robustness.
Stability.
-
Samples were grouped by theoretical titer and the GCV% was calculated from the mean of triplicate replicates per run. All individual-precision GCV values were <30%, with most values from 5%–20% (Figure 1A, B). All ten negative samples tested negative in all runs.
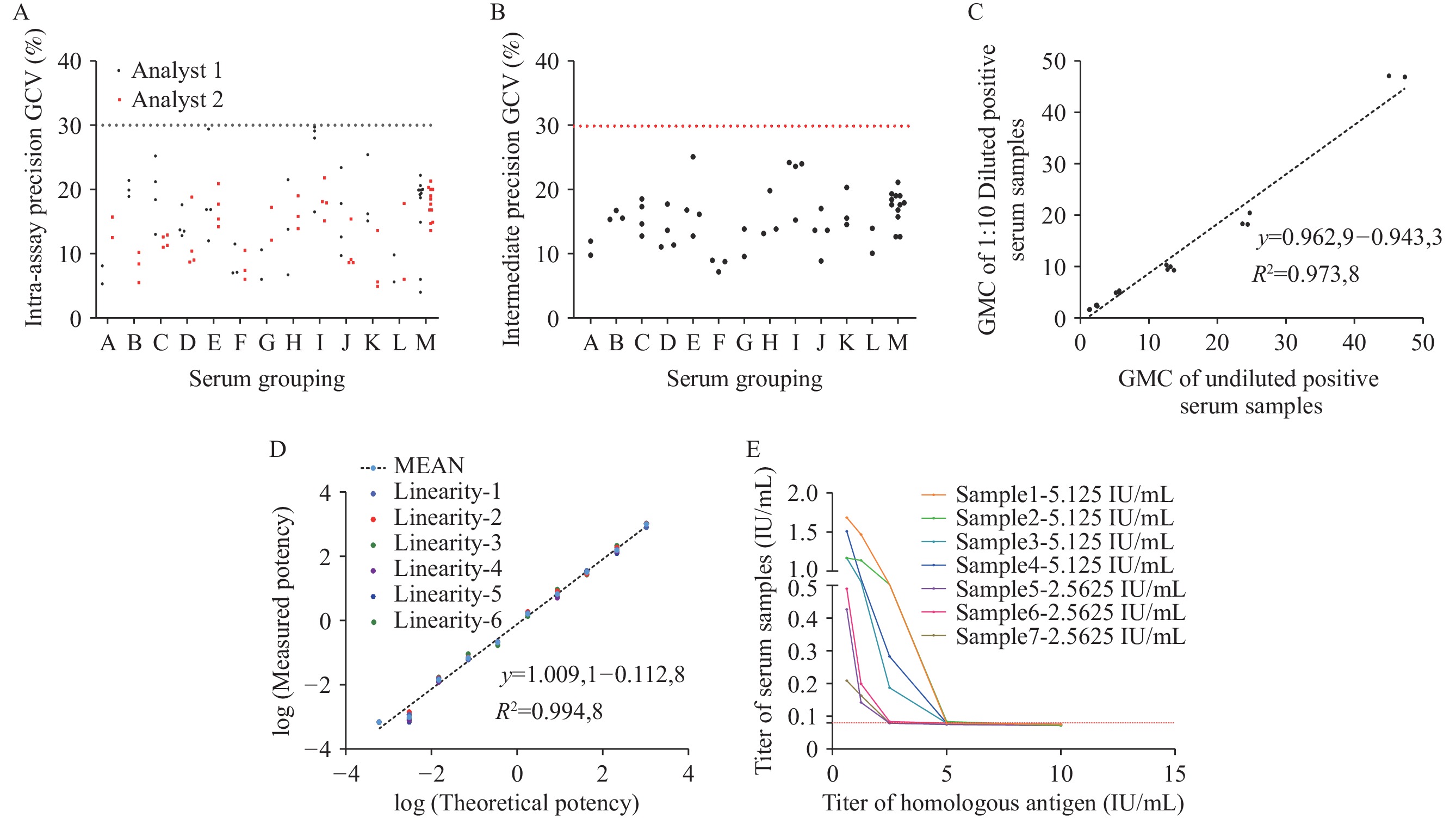 Figure 1.
Figure 1.The results of RFFIT validation. (A) Summary of profile of the RFFIT intra-assay precision; (B) Summary of profile of the RFFIT intermediate precision; (C) Dilutability regression plot for the RFFIT using 20 paired RVNA positive samples; (D) Linearity of WHO-3 SRIG; (E) RFFIT specificity: dose-dependent inhibition with inactivated homologous competitor.
Note: In A and B, serum grouping: A, 44 IU/mL; B, 20.5 IU/mL; C, 10.25 IU/mL; D, 5.125 IU/mL; E, 2.5625 IU/mL; F, 1.2813 IU/mL; G, 4.4 IU/mL; H, 2.05 IU/mL; I, 1.025 IU/mL; J, 0.5125 IU/mL; K, 0.25625 IU/mL; L, 0.12813 IU/mL; M, RVNA negative samples. Each scatter point represents the repeated test geometric coefficient of variation values of the individual samples. In (D), MEAN represents the average of six results; In (E), red horizontal lines denote lower limit of quantification values.
Abbreviation: RFFIT=rapid fluorescent focus inhibition test; RVNA=rabies virus neutralizing antibodies; WHO-3 SRIG=third World Health Organization international standard for anti-rabies immunoglobulin.
Using 20 undiluted and 1∶10 diluted, paired RVNA positive samples, 95% (19/20) of the samples tested had an absolute value of the percentage difference ≤30% between the value for each 1∶10 diluted and undiluted serum sample. Linear regression of the GMCs for these pairs showed an R2=0.9738 and a slope=0.9629, within acceptable limits indicating good dilution linearity (Figure 1C).
-
Of the tested concentrations of WHO-3 SRIG-spiked samples, 95.56% (86/90) of those with results ≥LLOQ exhibited percentage recoveries within the acceptable range of 70%–130%. The GCV% of the LLOQ was <30%. Linear regression demonstrated strong correlation and acceptable linearity (slope=1.0091, R2=0.9948), confirming that the accuracy and linearity acceptance criteria were met (Figure 1D).
-
For homologous inactivated rabies virus antigen analysis, all samples showed dose-dependent inhibition (Figure 1E). At the highest competitor concentration, RVNA titers were reduced by ≥97% in high-titer samples, whereas low-titer samples fell below the LLOQ. In the heterologous antigen analysis, titer change in all samples was within assay variability (≤30%). Matrix effect evaluation showed that RVNA titers in hemolytic, icteric, and lipemic samples differed by ≤30% from normal serum. These results confirm the specificity of RFFIT.
-
The RVNA titers (IU/mL) obtained from BSR cells at different passages exhibited differences within ±30%, with most variations being considerably smaller (e.g., −4.3% to 0.5%). Similarly, for cells tested on both day 2 and day 3 post-inoculation, the titer differences remained within an acceptable range, with the majority falling within ±25% (Table 2). Changes in experimental conditions resulted in percentage differences which were well within the ±30% range acceptable for cell-based assays (Table 3). These findings indicate that the assay was robust under various experimental conditions.
Condition RVNA titer
(IU/mL)Difference
(%)BSR passages Different days P20 2 5.1512 0.5 P30 5.1512 0.5 P40 4.9058 −4.3 P60 4.9272 −3.9 P70 4.9272 −3.9 P80 5.0578 −1.3 P81 2 5.7645 12.5 5.7645 12.5 5.5427 8.2 6.0741 18.5 2.1195 −17.3 2.1195 −17.3 2.2876 −10.7 2.2876 −10.7 1.0097 −21.2 1.0097 −21.2 P81 3 6.0741 18.5 5.8404 14.0 5.8404 14.0 6.4003 24.9 2.4104 −5.9 2.2334 −12.8 2.2334 −12.8 2.4104 −5.9 1.0639 −17.0 0.9921 −22.6 Note: The first section (rows 1–6) investigates the effect of cell passage number. The second section (rows 7–26) examines the impact of the cells on different days, which are specified for each group.
Abbreviation: RVNA=rabies virus neutralizing antibodies.Table 2. Impact of BSR cells and experimental conditions on robustness of RFFIT.
Incubation time Critical reagents (Supplier/ Cat. No.) RVNA titer
(IU/mL)Difference
(%)HI + SVN + PI + FITC DMEM FITC 30 min + 50 min + 23 h + 50 min Gibco/3023261 FUJIREBIO/311520 5.6156 9.6 30 min + 70 min + 25 h + 70 min Gibco/3023261 FUJIREBIO/311520 5.5066 7.4 60 min + 60 min + 24 h + 60 min Gibco/3023261 FUJIREBIO/311520 5.4707 6.7 30 min + 60 min + 24 h + 60 min Sigma/RNBN1157 FUJIREBIO/311520 5.7269 11.7 30 min + 60 min + 24 h + 60 min Gibco/3023261 FUJIREBIO/311624 5.7144 11.5 30 min + 60 min + 24 h + 60 min Gibco/3023261 FUJIREBIO/311520 5.7144 11.5 30 min + 60 min + 24 h + 60 min Gibco/3023261 Sigma/4206160 5.6156 9.6 30 min + 60 min + 24 h + 60 min Gibco/3023261 FUJIREBIO/311520 5.0578 −1.3 Note: The section examines the impact of alterations in incubation time and critical reagents, which are specified for each group.
Abbreviation: DMEM=Dulbecco’s modified Eagle’s medium; HI=heat inactivation; SVN=serum virus neutralization; PI=post-infection; FITC=fluorescein isothiocyanate; RFFIT=rapid fluorescent focus inhibition test; RVNA=rabies virus neutralizing antibodies.Table 3. Impact of experimental conditions on robustness of RFFIT.
-
The titers measured for samples and standards under freeze–thaw and different storage temperature conditions were all within ±30% of the baseline value (Table 4).
Condition RVNA titer (IU/mL) Difference (%) WHO-3 SRIG — 1 freeze–thaw cycle 39.2490 −28.2 WHO-3 SRIG — 2 freeze–thaw cycles 39.2490 −28.2 WHO-3 SRIG — 3 freeze–thaw cycles 39.2490 −28.2 WHO-3 SRIG — 4 freeze–thaw cycles 39.2490 −28.2 WHO-3 SRIG — 5 freeze–thaw cycles 44.1519 −19.2 Sample (5.125 IU/mL) — 1 freeze–thaw cycle 4.9058 −4.3 Sample (5.125 IU/mL) — 2 freeze–thaw cycles 4.9058 −4.3 Sample (5.125 IU/mL) — 3 freeze–thaw cycles 4.9058 −4.3 Sample (5.125 IU/mL) — 4 freeze–thaw cycles 4.9058 −4.3 Sample (5.125 IU/mL) — 5 freeze–thaw cycles 4.9058 −4.3 Sample (5.125 IU/mL): 4 ℃ 4 w 4.9058 −4.3 Sample (5.125 IU/mL): 4 ℃ 1 w 4.9058 −4.3 Sample (5.125 IU/mL): 4 ℃ 24 h 4.9058 −4.3 Sample (5.125 IU/mL): room temperature, 4 h 4.3610 −14.9 Rabies virus: room temperature, 15 min 4.9058 −4.3 Note: The baseline value of WHO-3 SRIG: 54.6667 IU/mL; room temperature: 20–25 ℃.
Abbreviation: RFFIT=rapid fluorescent focus inhibition test; RVNA=rabies virus neutralizing antibodies; WHO-3 SRIG=third World Health Organization international standard for anti-rabies immunoglobulin.Table 4. Stability evaluation of the RFFIT.
Precision and Dilutability
Accuracy, Linearity and Range
Specificity
Robustness
Stability
-
Various methods quantify RVNA. Commonly-used techniques include the mouse neutralization test (MNT), indirect immunofluorescence assay, RFFIT, fluorescent antibody virus neutralization test (FAVN), and enzyme-linked immunosorbent assay (ELISA). RFFIT is the most widely-used cell-based assay for detecting and quantifying rabies virus neutralizing antibodies in serum (3). Its results can be used for RVNA testing for pre- or post-exposure prophylaxis in humans or animals, as well as for the clinical diagnosis of rabies, detection of neutralizing activity of monoclonal antibodies against the rabies virus, determination of potency of immunoglobulin preparations, evaluation of the efficacy of new vaccines, development of new vaccination schedules, and evaluation and calibration of new serological testing methods (10). This validation supports the implementation of robust quality control measures and confirms the reliability of RFFIT for quantifying RVNA in serum.
Rabies antibody testing determines immunity levels conferred by pre- and post-exposure vaccinations. Although the intermediate precision met the acceptance criterion of ≤30% GCV, higher GCV values were generally observed in samples with low antibody titers near the critical threshold of 0.5 IU/mL. The WHO Rabies Expert Advisory Committee considers antibody levels ≥0.5 IU/mL in serum to indicate effective protection. If the antibody titer falls below 0.5 IU/mL, multiple booster doses should be administered until sufficient antibodies are produced. Therefore, accurate measurements around this cutoff are essential for determining seroconversion and adequate immune protection in clinical practice. The increased variability observed near this threshold can be attributed to the inherent limitations of serological assays at low analyte concentrations, including reduced signal-to-noise ratios and the impact of biological variability. Nevertheless, the RFFIT method still conformed to the pre-specified validation criterion of ≤30% GCV across all samples, underscoring its overall reliability.
This study has several limitations. First, validation was performed using serum spiked with WHO-3 SRIG rather than clinical samples from vaccinated individuals. Second, the sample size was limited (n=50) and may not fully represent the diversity of immune responses across populations. Finally, precision was reduced near the critical threshold of 0.5 IU/mL.
In conclusion, this study demonstrated that the validated RFFIT method exhibited excellent analytical performance for quantifying RVNA in post-vaccination serum. The assay met all criteria for specificity, accuracy, precision, stability, linearity, and robustness, ensuring result integrity and reproducibility under varied conditions. These findings support the suitability of RFFIT for the reliable assessment of vaccine-induced immunity in both clinical and research settings (15). Its broader implementation for serological monitoring in rabies sero-surveillance and vaccine evaluation studies is recommended.
-
This study did not involve human or animal subjects; therefore, no ethical statements were required.
| Citation: |

|