
 Download:
Download:




-
Introduction: This study aimed to quantify potentially inappropriate medication (PIM) use for primary cardiovascular disease (CVD) prevention in China and its attributable mortality and morbidity.
Methods: Data from the 2015, 2018, and 2023 China Chronic Disease and Risk Factor Surveillance were analyzed for adults aged ≥30 years without diagnosed CVD. PIM use was defined according to guideline adherence for aspirin, statins, antihypertensives, and glucose-lowering agents. Population attributable fractions (PAFs) were calculated using weighted prevalence and relative risks, and CVD outcomes were derived from the Global Burden of Disease 2023.
Results: From 2015 to 2023, PIM prevalence for primary CVD prevention declined by half, with larger relative reductions observed among women and older adults. The number of PIM-attributable CVD deaths decreased by 39%, and its rank among CVD risk factors dropped from 17th to 21st after 2018. Before 2018, 15 provinces showed increases in PIM-attributable CVD mortality and morbidity, but subsequent declines occurred in 30 provinces for mortality and 28 for morbidity, with Inner Mongolia and Tianjin showing the largest improvements.
Conclusion: Despite marked progress, disparities persist across regions and populations. Establishing population-based PIM surveillance and implementing targeted interventions in high-burden areas are essential to further reduce preventable CVD morbidity and mortality.
-
In 2017, the World Health Organization launched the Medication Without Harm initiative, aiming to reduce severe avoidable medication-related harm by 50% within five years (1). However, China’s progress toward this target remains unclear. As cardiovascular diseases (CVD) remain the leading cause of death in China, improving primary prevention is essential for reducing CVD morbidity and mortality (2–3). This study quantified potentially inappropriate medication (PIM) use for primary CVD prevention, its population attributable fractions (PAFs), and the corresponding CVD mortality and morbidity.
The China Chronic Disease and Risk Factor Surveillance (CCDRFS) was conducted in 2015, 2018, and 2023 across 302 surveillance points in 31 provinces using a multistage stratified cluster sampling method to obtain nationally representative data. Residents aged ≥18 years were invited to participate, with response rates exceeding 97% in all surveys. Detailed methods have been reported elsewhere (4).
PIMs for CVD prevention were defined among participants without a history of CVD as follows: 1) aspirin use inconsistent with guideline recommendations (2019 Chinese Expert Consensus on the Use of Aspirin for the Primary Prevention of Cardiovascular Diseases; 2020 Chinese Guideline for the Primary Prevention of Cardiovascular Diseases); 2) statin use inconsistent with guideline recommendations (2020 Chinese Guideline for the Primary Prevention of Cardiovascular Diseases; 2023 Chinese Guideline for Lipid Management in Adults); 3) absence of antihypertensive therapy among individuals aware of having hypertension with uncontrolled blood pressure (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg), without contraindications to therapy and without intention to modify lifestyle; or 4) absence of oral glucose-lowering drugs or insulin among individuals with diagnosed diabetes and uncontrolled glycemia (fasting blood glucose ≥7.0 mmol/L or hemoglobin A1c ≥6.5%), without contraindications to therapy and without intention to modify lifestyle.
All calculations were weighted according to the sampling scheme, with post-stratification adjustments based on Chinese population estimates from the National Bureau of Statistics. Relative risks associated with PIM use were estimated using Cox proportional hazards models. Mortality and morbidity data for CVDs were obtained from the Global Burden of Disease 2023 study. Statistical analyses were conducted using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA), and data visualization was performed with Python software (version 3.11; Python Software Foundation, Wilmington, DE, USA).
This study included 473,324 community-dwelling adults aged ≥30 years without diagnosed CVDs or related hospitalizations (157,565 in 2015, 155,245 in 2018, and 160,514 in 2023). Among the 157,565 participants enrolled in 2015 and linked to hospitalization and mortality records through 2020, 2,097 deaths and 17,037 CVD events occurred over five years. In each survey, the proportion of men (42.8%–47.0%) was lower than that of women. The proportions of older adults (mean age increased from 53.8 to 58.5 years), urban residents (39.8% to 45.7%), and individuals with hypertension (40.4% to 51.9%), diabetes (9.1% to 25.6%), and dyslipidemia (36.8% to 41.7%) all increased over the study period. The distributions of participants by region and education remained relatively stable across survey years.
PIM prevalence for primary CVD prevention declined by nearly half (47.7%), from 4.4% in 2015 to 2.3% in 2023. Men and women showed similar declines, with slightly lower levels in women by 2023. PIM prevalence rose with age — especially ≥50 years — but decreased across all age groups. Initially, urban prevalence exceeded rural levels, but by 2023 the rates converged, with rural slightly higher. Regionally, the North and Northeast consistently had the highest PIM levels, and the South and Southwest the lowest, though all regions showed declines (Table 1).
Characteristics 2015 2018 2023 P* (95% CI) PAF (95% CI) † P* (95% CI) PAF (95% CI) † P* (95% CI) PAF (95% CI) † Mortality Morbidity Mortality Morbidity Mortality Morbidity Total 4.4 (3.9–4.8) 3.0 (2.3–3.6) 3.2 (3.0–3.4) 3.7 (3.4–4.0) 2.5 (2.0–3.0) 2.7 (2.6–2.9) 2.3 (2.1–2.4) 1.6 (1.2–1.9) 1.7 (1.6–1.8) Sex Male 4.3 (3.7–4.8) 3.7 (3.1–4.3) 3.2 (2.9–3.5) 3.7 (3.4–4.0) 3.2 (2.7–3.8) 2.8 (2.5–3.0) 2.4 (2.2–2.6) 2.1 (1.8–2.5) 1.8 (1.7–2.0) Female 4.4 (4.1–4.8) 1.7 (0.7–2.8) 3.3 (3.0–3.6) 3.7 (3.3–4.0) 1.4 (0.6–2.3) 2.8 (2.5–3.0) 2.1 (1.9–2.3) 0.8 (0.3–1.3) 1.6 (1.5–1.7) Age group (years) 30–34 0.8 (0.6–1.1) 0.6 (0.4–0.7) 0.1 (0.0–1.2) 0.9 (0.5–1.2) 0.6 (0.5–0.7) 0.1 (0.0–1.3) 0.6 (0.4–0.9) 0.4 (0.4–0.5) 0.1 (0.0–1.0) 35–39 1.6 (1.2–2.0) 1.1 (0.9–1.3) 1.9 (1.1–2.7) 1.3 (1.0–1.6) 0.9 (0.7–1.1) 1.6 (0.9–2.2) 0.3 (0.2–0.5) 0.2 (0.2–0.3) 0.4 (0.2–0.6) 40–44 2.1 (1.7–2.5) 1.5 (1.2–1.8) 2.0 (1.3–2.7) 2.0 (1.7–2.4) 1.4 (1.1–1.7) 1.9 (1.3–2.6) 0.9 (0.6–1.2) 0.6 (0.5–0.8) 0.9 (0.6–1.2) 45–49 3.4 (2.8–3.9) 2.3 (1.8–2.8) 2.5 (1.9–3.2) 3.2 (2.7–3.6) 2.2 (1.7–2.6) 2.4 (1.7–3.0) 1.5 (1.2–1.8) 1.0 (0.8–1.3) 1.2 (0.8–1.5) 50–54 4.8 (4.3–5.3) 3.2 (2.6–3.9) 3.6 (3.0–4.3) 4.8 (4.1–5.4) 3.2 (2.6–3.9) 3.6 (2.9–4.3) 2.5 (2.1–2.8) 1.7 (1.4–2.1) 1.9 (1.6–2.3) 55–59 6.3 (5.4–7.2) 4.2 (3.4–5.1) 2.9 (2.1–3.8) 5.6 (4.9–6.2) 3.8 (3.0–4.5) 2.6 (1.9–3.3) 3.5 (3.1–3.9) 2.4 (1.9–2.9) 1.7 (1.2–2.1) 60–64 7.6 (6.8–8.5) 5.1 (4.0–6.1) 3.0 (2.2–3.8) 6.9 (6.3–7.6) 4.6 (3.7–5.6) 2.8 (2.0–3.5) 4.5 (4.1–5.0) 3.1 (2.4–3.7) 1.8 (1.3–2.3) 65–69 8.8 (7.6–9.9) 5.8 (4.6–6.9) 3.1 (2.2–4.0) 8.4 (7.4–9.4) 5.5 (4.4–6.7) 3.0 (2.1–3.8) 5.2 (4.7–5.7) 3.5 (2.8–4.3) 1.9 (1.3–2.4) ≥70 10.1 (8.0–12.3) 6.6 (5.3–7.9) 2.2 (1.4–3.1) 8.1 (7.2–9.1) 5.4 (4.3–6.5) 1.8 (1.1–2.5) 6.9 (6.1–7.6) 4.6 (3.7–5.5) 1.5 (0.9–2.1) Residency Urban 4.9 (4.2–5.6) 3.3 (2.6–4.0) 3.6 (3.4–3.8) 3.8 (3.4–4.2) 2.6 (2.1–3.1) 2.8 (2.7–3.0) 2.2 (2.0–2.4) 1.5 (1.2–1.8) 1.6 (1.5–1.7) Rural 3.7 (3.4–4.0) 2.5 (2.0–3.0) 2.7 (2.6–2.9) 3.5 (3.2–3.9) 2.4 (1.9–2.9) 2.6 (2.5–2.8) 2.3 (2.1–2.5) 1.6 (1.3–1.9) 1.8 (1.6–1.9) Subnational region§ Central 4.0 (3.0–5.0) 2.7 (2.2–3.3) 3.0 (2.8–3.1) 3.7 (3.0–4.4) 2.5 (2.0–3.0) 2.7 (2.6–2.9) 2.5 (2.1–2.8) 1.7 (1.3–2.1) 1.9 (1.7–2.0) East 4.6 (3.7–5.4) 3.1 (2.5–3.7) 3.4 (3.2–3.6) 3.4 (2.9–3.8) 2.3 (1.8–2.8) 2.5 (2.4–2.7) 1.8 (1.6–2.0) 1.2 (1.0–1.5) 1.3 (1.2–1.4) North 6.5 (5.8–7.2) 4.3 (3.5–5.2) 4.7 (4.5–5.0) 6.2 (5.3–7.1) 4.2 (3.3–5.0) 4.5 (4.3–4.8) 3.9 (3.3–4.5) 2.7 (2.1–3.2) 2.9 (2.7–3.1) Northeast 5.7 (4.3–7.2) 3.9 (3.1–4.6) 4.2 (4.0–4.5) 5.5 (4.2–6.7) 3.7 (2.9–4.4) 4.0 (3.8–4.3) 2.7 (2.0–3.4) 1.8 (1.5–2.2) 2.0 (1.9–2.1) Northwest 5.0 (4.0–5.9) 3.4 (2.7–4.1) 3.7 (3.5–3.9) 4.2 (3.2–5.1) 2.8 (2.3–3.4) 3.1 (2.9–3.3) 3.2 (2.5–3.9) 2.2 (1.7–2.6) 2.4 (2.2–2.5) South 2.5 (1.4–3.5) 1.7 (1.3–2.0) 1.8 (1.7–2.0) 1.7 (1.3–2.1) 1.2 (0.9–1.4) 1.3 (1.2–1.4) 1.5 (1.1–1.8) 1.0 (0.8–1.2) 1.1 (1.0–1.2) Southwest 2.9 (2.3–3.4) 2.0 (1.6–2.4) 2.2 (2.0–2.3) 2.4 (1.8–3.1) 1.7 (1.3–2.0) 1.8 (1.7–2.0) 1.6 (1.3–1.9) 1.1 (0.9–1.4) 1.2 (1.1–1.3) * P indicates the prevalence of potentially inappropriate medication use among the Chinese population aged ≥30 years. Prevalence values were weighted to represent the overall national population.
† PAF =population attributable fraction; CI=confidence interval.
§ Subnational regions were classified as follows: East (Shanghai, Jiangsu, Zhejiang, Anhui, Fujian, Jiangxi, Shandong); Central (Henan, Hubei, Hunan); Southwest (Sichuan, Guizhou, Yunnan, Chongqing, Xizang); North (Beijing, Tianjin, Hebei, Shanxi, Inner Mongolia); South (Guangdong, Guangxi, Hainan); Northeast (Liaoning, Jilin, Heilongjiang); Northwest (Shaanxi, Gansu, Qinghai, Ningxia, Xinjiang).Table 1. Prevalence and population attributable fractions of mortality and morbidity due to potentially inappropriate medication use among adults receiving primary prevention for cardiovascular disease, China, 2015–2023.
Overall, PAFs for CVD morbidity attributable to PIM use exceeded those for mortality. Mortality PAFs increased with age, while morbidity PAFs peaked at ages 50–69 years. Mortality PAFs were consistently higher in men, whereas morbidity PAFs were similar between sexes. Both declined by about half from 2015 to 2023. Urban PAFs initially exceeded rural values but converged by 2023. Relative reductions were greater in women, and absolute declines were largest among older adults. Regionally, PAFs were highest in the North and Northeast and lowest in the South and Southwest (Table 1).
PIM use showed a clear downward trend in its contribution to CVD-related deaths. Its rank among causes of CVD deaths was 17th in both 2015 and 2018, declining to 21st in 2023, indicating a relative reduction compared with other risk exposures. The absolute burden also decreased substantially — by approximately 39%, from 1.0 million deaths in 2015 to 0.6 million in 2023 — with a more pronounced decline after 2018 (Figure 1).
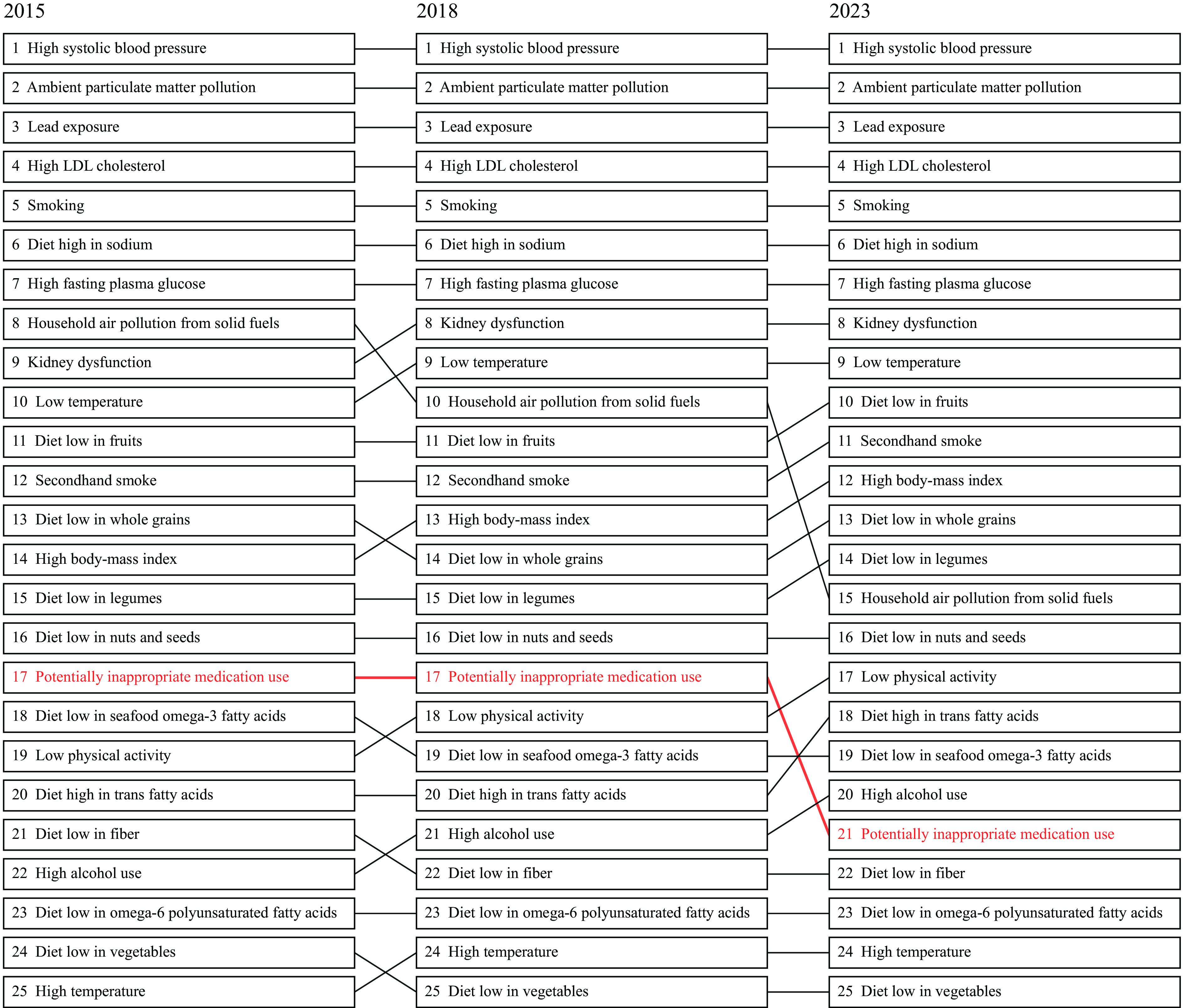 Figure 1.
Figure 1.Ranking of the top 25 risk factors by attributable cardiovascular disease deaths in China, 2015, 2018, and 2023 (both sexes).
Note: Estimates for risk factors other than potentially inappropriate medication use were derived from the Global Burden of Disease 2023. The estimates of cardiovascular disease (CVD) deaths attributable to the potentially inappropriate medication use were derived from population attributable fractions and the death counts due to CVD estimates from the Global Burden of Disease 2023.The study examined provincial disparities in trends of PIM–attributable CVD deaths and incidence between 2015–2018 and 2018–2023. From 2015 to 2018, 15 provinces exhibited increasing trends in PIM-attributable CVD deaths and incidence. After 2018, however, most provinces experienced declines, except Gansu for deaths and Gansu, Guangdong, and Yunnan for incidence. The most substantial reductions in CVD mortality and incidence were observed in Inner Mongolia and Tianjin during 2018–2023 (Figure 2).
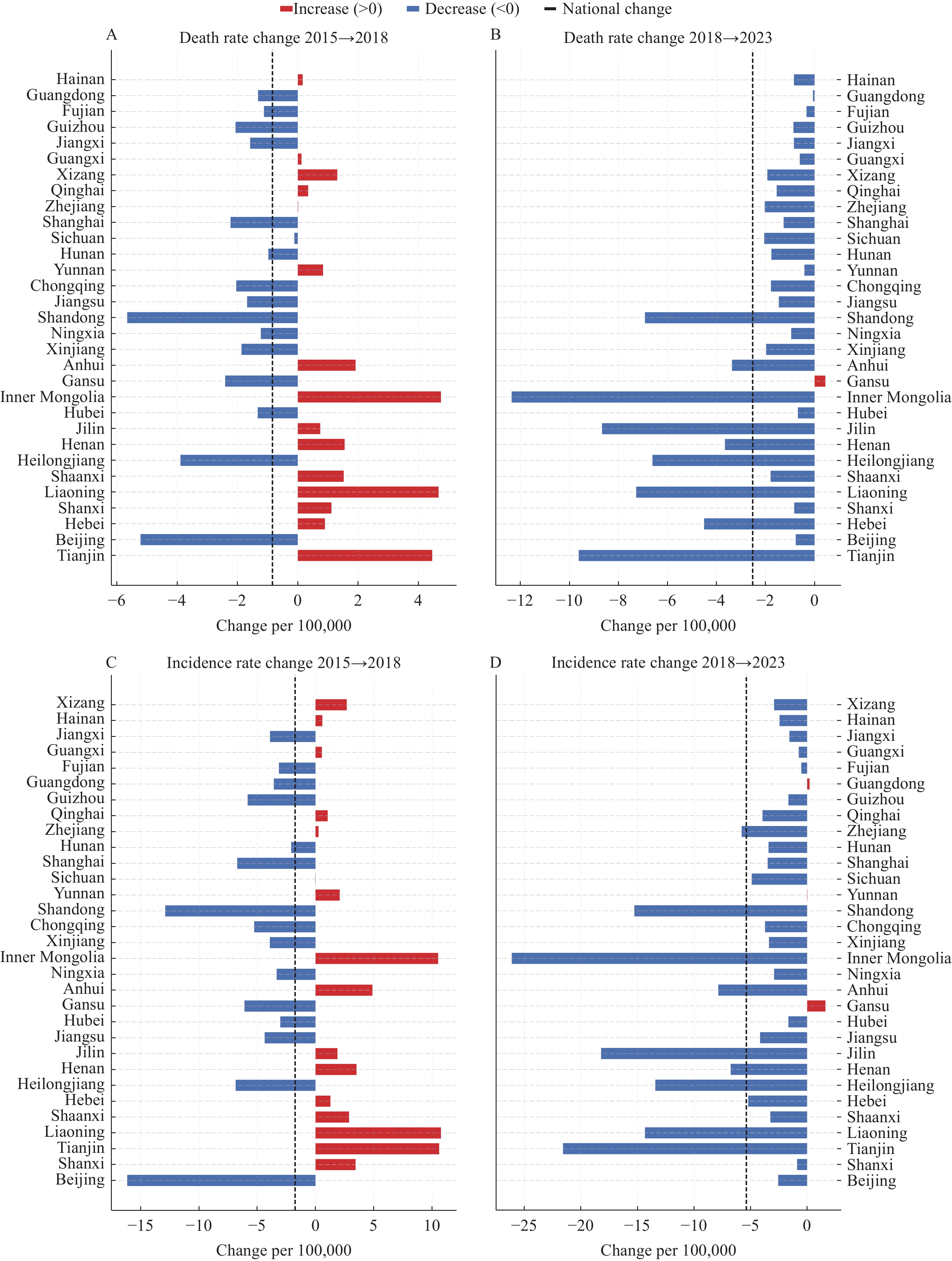 Figure 2.
Figure 2.Province-level changes in CVD mortality and morbidity attributable to potentially inappropriate preventive medication use, China, 2015–2018 and 2018–2023. (A) Death rate change 2015−2018; (B) Death rate change 2018−2023; (C) Incidence rate change 2015−2018; (D) Incidence rate change 2018−2023.
Note: Estimates were derived from province-specific population attributable fractions applied to provincial mortality and morbidity data. -
To our knowledge, this is the first study to reveal national trends and provincial variations in PIM use attributable to CVD deaths and incidence in China, which yielded four main findings. First, we observed substantial improvement in medication management alongside persistent challenges in optimizing rational medication use for cardiovascular prevention across demographic and geographic subgroups. Despite a sustained decline in PIM use, approximately 2.3% of the primary prevention population in 2023 still received inappropriate medications, which represents a considerable burden given China’s large population base.
Second, the parallel 50% reductions in mortality and morbidity PAFs indicate major progress in medication stewardship and CVD prevention. Morbidity PAFs remained higher than mortality PAFs, suggesting that PIM mainly contributes to new CVD events, while the narrowing gap reflects improved acute care and secondary prevention. By 2023, rural PAFs slightly exceeded urban values, highlighting uneven progress and the need to strengthen prescribing quality and follow-up in rural areas. Persistently higher mortality PAFs in men indicate greater fatal risk, calling for focused medication review, risk-factor control, and emergency preparedness. Marked age and north–south gradients further support targeted interventions for older adults and high-burden northern regions, reinforced by ongoing surveillance.
Third, the rank of PIM–attributable CVD deaths declined significantly from 17th to 21st after 2018 among all CVD risk factors, marking a pivotal turning point. Three major developments between 2017 and 2019 may explain this shift. First, three landmark clinical trials — ARRIVE, ASPREE, and ASCEND — fundamentally questioned the role of aspirin in primary prevention, leading to widespread revisions in international clinical guidelines (5–6). Second, China’s centralized medicine procurement policy, launched in 2019, substantially improved the cost-effectiveness of pharmacotherapies for CVD prevention (7). Third, in 2018, China introduced explicit criteria for PIM use in older adults to enhance prescribing oversight and rational medication management (8). Collectively, these evidence- and policy-driven reforms may explain the downward trend in PIM-attributable CVD deaths observed after 2018.
Fourth, regional policy initiatives in Inner Mongolia (since 2019) and Tianjin (since 2020) likely contributed to the observed declines in PIM-attributable CVD deaths and incidence. In December 2019, Inner Mongolia issued a reform plan mandating stricter supervision of drug and consumable use (9). By March 2020, all medical institutions across the region were required to establish and publicly disclose key drug monitoring lists, followed by the implementation of a province-wide surveillance system integrating clinical monitoring with performance assessment. In 2020, the Tianjin government introduced digital health community platforms at the primary care level across four districts — Hebei, Jinnan, Dongli, and Xiqing (10). PIM use was restricted through an online, AI-enabled prescription review system. These coordinated policy actions likely played a key role in reducing PIM-attributable CVD deaths and incidence after 2018.
Several limitations of this study should be acknowledged. First, untreated individuals who were unaware of having hypertension but met diagnostic thresholds, and those unaware of having diabetes despite elevated fasting blood glucose (≥7.0 mmol/L) or hemoglobin A1c (≥6.5%), were not classified as receiving PIM. Consequently, our estimates may underestimate the burden among individuals who should have received pharmacotherapy but did not. Second, we used International Classification of Diseases, 10th Revision (I00–I99) codes to identify CVDs in real-world settings; however, this approach may obscure differences among specific CVD subtypes. Third, we analyzed mortality and morbidity but not disability-adjusted life years. Fourth, causal inferences regarding policy interventions require further validation. Lastly, while sensitivity analyses were not conducted, the robustness of our findings is supported by the large sample size, high response rates, and consistent patterns across demographic strata and survey years.
In conclusion, although progress in rational medication use for CVD prevention is evident, gaps persist across regions and populations. Establishing population-based medication surveillance and integrating rational-use training and public education into basic public health services — particularly in northern and northeastern provinces — are essential for further reduce the CVD burden attributable to PIM.
-
The authors express their sincere appreciation to all staff members who contributed to data collection and participated in this study.
-
Approved by the Institutional Review Board of the National Center for Chronic and Non-Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention (Approval Nos. 201519-A, 201819, and 202305), and written informed consent wasobtained from all participants.
HTML
| Citation: |

|