
 Download:
Download:




-
Introduction Climate change is intensifying extreme heat events, positioning heat-related illness as an escalating public health threat. However, multi-provincial, individual-level evidence quantifying the association between elevated temperatures and heat-related illness in China remains limited.
Methods This multi-provincial study employed a time-stratified case-crossover design. Individual heat-related illness case data (2013–2022) were obtained from the Heat-related Illness Report System, which collects reports from local healthcare facilities and CDCs across 11 provincial-level administrative divisions (PLADs). We evaluated associations between daily mean and maximum temperatures and heat-related illness risk across multiple lag periods (lag0 to lag07), with lag01 designated a priori as the primary exposure window. Effect estimates are presented as relative risks (RR) and percentage changes in RR per 1°C temperature increase. Subgroup analyses examined potential effect modification by sex, age, heat-related illness subtype, heat intensity, and geographic location.
Results Between 2013 and 2022, 53,061 heat-related illness cases were recorded across study areas, with annual counts rising throughout the decade and reaching a peak of 14,025 in 2022. Although mild cases predominated each year (maximum 83.0% in 2015), the proportion of severe cases exhibited a concerning gradual increase. Regarding temperature associations, each 1°C increase in daily mean temperature corresponded to a 21.03% (95% CI: 20.59, 21.47) elevation in the RR of heat-related illness. Daily maximum temperature demonstrated a comparable pattern, though risk estimates were marginally lower.
Conclusion This study demonstrates a clear upward trend in heat-related illness incidence linked to climate change and confirms that elevated temperatures significantly increase disease risk. The escalating health burden necessitates urgent development and implementation of targeted heat-health action plans to protect vulnerable populations.
-
Climate change is intensifying both the frequency and severity of heatwaves, thereby elevating risks across multiple adverse health outcomes (1), with heat-related illness emerging as a critical concern (2). Heat-related illnesses are defined as conditions resulting from prolonged exposure to high temperatures and/or strenuous physical activity in hot and humid environments, occurring when the body accumulates heat faster than its thermoregulatory capacity can dissipate it (3). These conditions have become a major public health concern during summer months. Heat-related illnesses range from mild to severe and can be categorized into heat cramps, heat exhaustion, and heat stroke based on clinical presentation. While several local studies have documented associations between temperature and heat-related illnesses (4–6), national-level evidence remains limited, particularly regarding specific illness subtypes. Therefore, this study aimed to analyze the epidemiological characteristics of heat-related illnesses across multiple provincial-level administrative divisions (PLADs) in China from 2013 to 2022 and to quantify the association between temperature and heat-related illness risk to inform public health policy development and guide future research priorities.
Heat-related illness data spanning 2013 to 2022 were obtained from the Heat-related Illness Report System, which compiles reports submitted by local medical institutions during patient diagnosis and treatment, as well as by CDCs during the management of heat-related illness incidents (7). We focused our analysis on 11 PLADs with continuous reporting throughout the study period: Anhui, Beijing, Guangdong, Hubei, Hunan, Jiangxi, Shandong, Shanxi, Shanghai, Zhejiang, and Chongqing. Cases with missing or inconsistent patient identification numbers or reporting addresses were excluded from the analysis. We restricted our investigation to incidents occurring between May and September, the primary heat season in China. The final analytical dataset comprised individual-level information on sex, age, reporting location, date of illness onset, and heat-related illness subtype. Meteorological data, including hourly temperature and dewpoint temperature measurements, were retrieved from the European Centre for Medium-Range Weather Forecasts (ECMWF) reanalysis database. These meteorological variables were extracted at a 0.25° spatial resolution and subsequently aggregated to generate daily county-level metrics, including both daily mean and daily maximum values.
We employed a time-stratified case-crossover study design coupled with conditional logistic regression models, stratified by individual cases, to quantify the linear association between temperature exposure and heat-related illness risk across different subtypes. Models were adjusted for potential confounders, including daily dewpoint temperature and holiday status (categorized as weekday, weekend, or public holiday). We examined multiple exposure windows from lag0 (same-day exposure) through lag07 (7-day cumulative exposure), with lag01 (cumulative exposure over the current and previous day) designated a priori as the primary exposure window. Effect estimates were expressed as the percentage change in relative risk (RR) per 1°C increase in both mean daily temperature and maximum daily temperature. Subgroup analyses were conducted to assess effect modification by sex (male, female), age (<65 years, ≥65 years), heat-related illness subtype (mild, severe, heat cramps, heat exhaustion, heat stroke), and temperature threshold (>30 °C versus ≤30 °C for mean daily temperature; >35 °C versus ≤35 °C for maximum daily temperature). Given that Zhejiang Province contributed over 50% of all reported cases, we performed separate analyses for Zhejiang and non-Zhejiang regions to evaluate potential geographic heterogeneity in temperature-illness associations. All statistical analyses were performed using R software (version 4.4.1, R Foundation for Statistical Computing, Vienna, Austria), with statistical significance defined as P<0.05.
Between 2013 and 2022, 53,061 heat-related illness cases were documented across the study sites, demonstrating a generally upward trajectory that peaked at 14,025 cases in 2022. Geographically, Zhejiang Province accounted for the largest proportion (54.2%) of cumulative cases, followed by Anhui (13.0%), Hubei (9.3%), Chongqing (7.7%), and Shandong (6.2%). Mild heat-related illness constituted the predominant subtype each year, reaching its highest proportion of 83.0% in 2015. Notably, severe cases exhibited a gradual proportional increase throughout the study period. Men comprised the majority of cases, with their proportion escalating to 79.5% by 2021. The age distribution remained relatively consistent, primarily affecting young and middle-aged adults, although the proportion of older individuals (≥65 years) peaked at approximately 30% in 2022 (Figure 1).
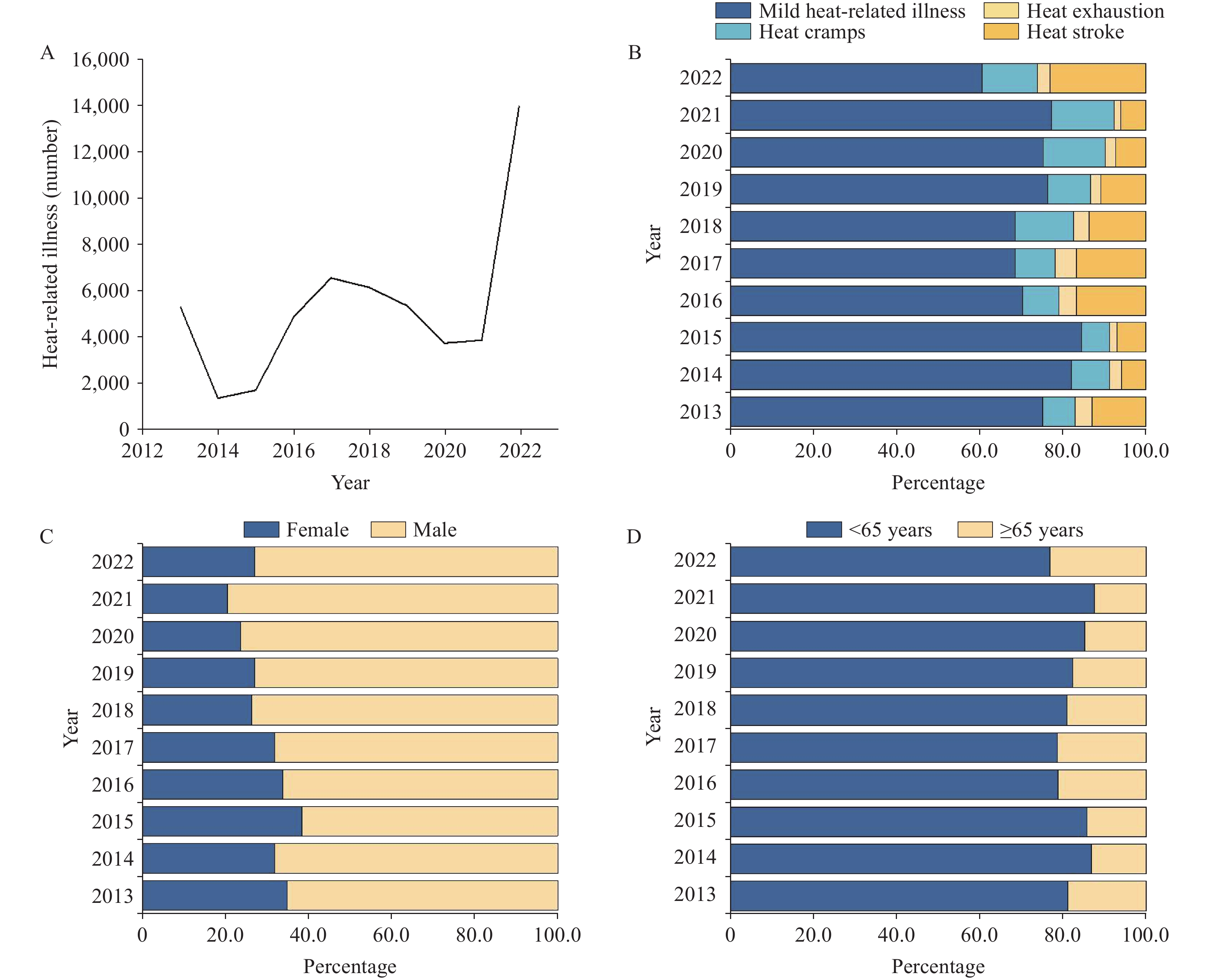 Figure 1.
Figure 1.Basic characteristics of heat-related illness cases from 2013 to 2022.(A) The annual number of heat-related illness cases; (B) The yearly distribution of heat-related illness subtypes (mild heat-related illness, severe heat-related illness, heat cramps and heat exhaustion, heat stroke); (C) The annual sex-based distribution (male, female) of heat-related illness; (D) The yearly age-based distribution (<65 years, ≥65 years) of heat-related illness.
Our analysis demonstrated that each 1°C increase in daily average temperature corresponded to a 21.03% elevation in the RR of heat-related illnesses [95% confidence interval (CI): 20.59%, 21.47%]. Stratified by population group, the RR increased by 22.03% (95% CI: 21.48%, 22.60%) for men, 26.62% (95% CI: 25.67%, 27.58%) for women, 35.67% (95% CI: 34.43%, 36.91%) for older adults, and 20.48% (95% CI: 19.96%, 21.00%) for younger individuals. All differences achieved statistical significance (P<0.05). When examining the effects of elevated temperatures, no substantial risk emerged below 30 °C. We further analyzed the relationship between temperature and specific subtypes of heat-related illness. Each 1°C increase in daily average temperature was associated with a 19.19% (95% CI: 18.66%, 19.72%) increase in mild heat-related illnesses, a 38.94% (95% CI: 37.77%, 40.13%) increase in severe heat-related illnesses, a 36.00% (95% CI: 33.90%, 38.14%) increase in heat cramps, an 86.87% (95% CI: 79.45%, 94.59%) increase in heat exhaustion, and a 62.48% (95% CI: 60.01%, 64.98%) increase in heat stroke. Daily maximum temperature exhibited a similar pattern, although the overall risk estimates were marginally lower (Figure 2). The robustness of these findings across different lag periods is presented in the Supplementary Material (
Supplementary Table S1 ). Additional comparative analysis between Zhejiang and non-Zhejiang regions revealed that results based on all study sites aligned closely with those from Zhejiang Province alone, whereas findings from non-Zhejiang regions generally showed slightly higher risk estimates than those observed in Zhejiang (Supplementary Table S2 ).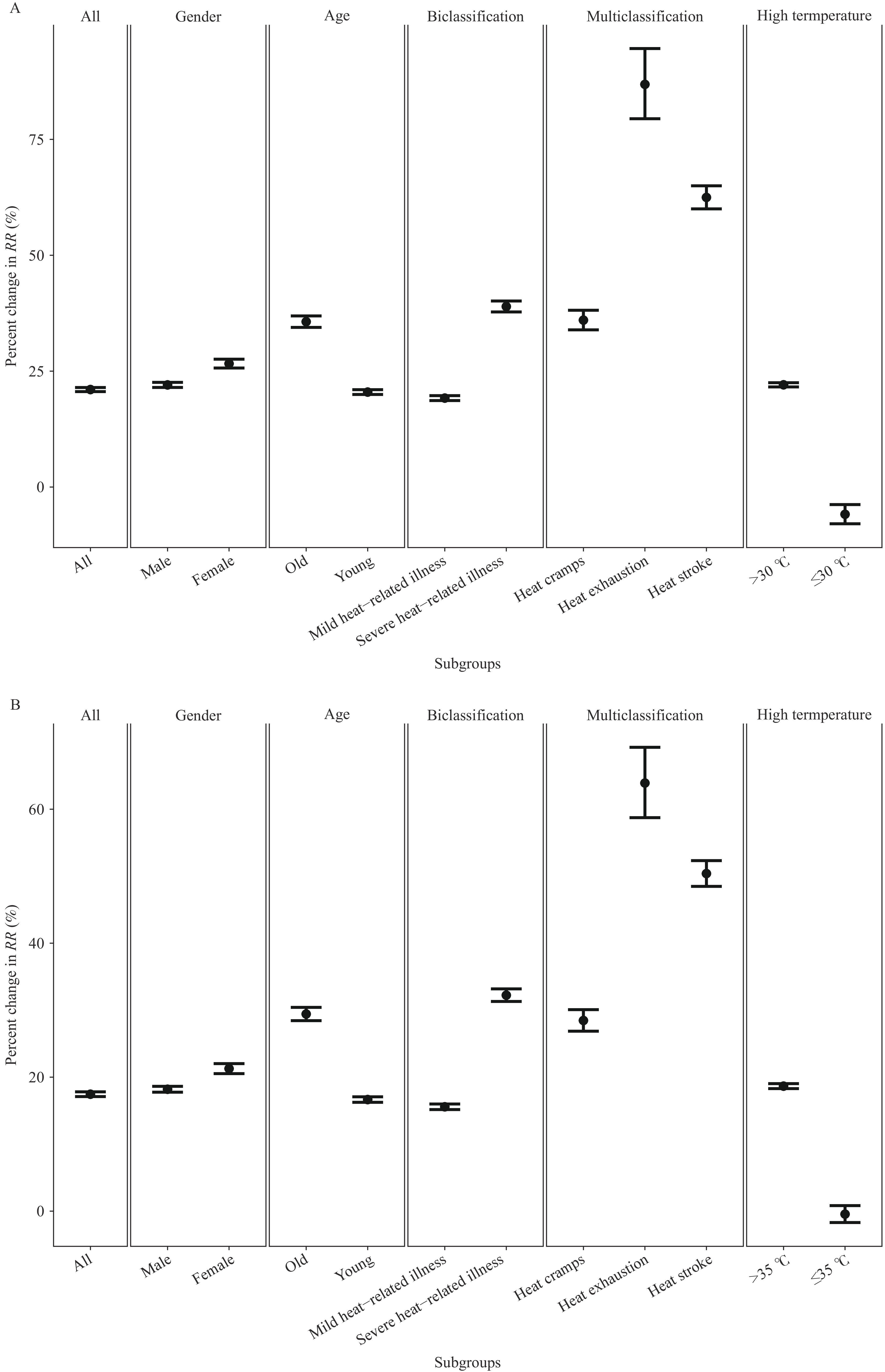 Figure 2.
Figure 2.Association between temperature and heat-related illness at lag01. (A) The relationship between daily mean temperature and heat-related illness at lag01. (B) The relationship between daily maximum temperature and heat-related illness at lag01.
Note: In each graph, panels from left to right correspond to overall results, gender-stratified results, age-stratified results, subtype-stratified results, and temperature-stratified results.
Abbreviation: RR=risk ratio.
-
This study utilized decade-long, cross-provincial data to characterize the spatial-temporal patterns of heat-related illness and quantify its association with temperature. Our findings reveal a generally increasing trend in heat-related illnesses over the past decade, with most cases occurring in men and individuals under 65 years of age, predominantly classified as mild heat-related illness. Notably, women and older individuals exhibited heightened sensitivity to elevated temperatures, with significant risks emerging when daily average temperatures exceeded 30°C and daily maximum temperatures surpassed 35°C. The risk of severe heat-related illness, including heat exhaustion and heat stroke, was highest under these conditions.
Our findings confirmed that high temperatures substantially increase the risk of heat-related illness, with effects persisting for several days following exposure. These results align with previous studies (4–6), underscoring the critical importance of implementing preventive measures during extreme heat events. Without prompt recognition and treatment, heat-related illness can progress to multi-organ dysfunction, failure, and death. Given the severity of these outcomes, prevention strategies are paramount. Evidence-based protective measures during extreme heat include maintaining access to air-conditioned environments, utilizing cooling devices, ensuring adequate hydration, and minimizing strenuous physical activity (8).
Our results indicate that while men and individuals under 65 years experience a higher incidence of heat-related illnesses, likely attributable to occupational exposures and activity patterns (9), women and older adults face disproportionately greater health risks from elevated temperatures. Current studies offer varying conclusions on sex differences in heat-related illness susceptibility, with explanations encompassing physiological factors, pathophysiological mechanisms, and differential exercise-heat exposure scenarios (10). Additionally, older adults demonstrate increased vulnerability to heat-related illnesses due to diminished thermoregulatory capacity and higher prevalence of chronic comorbidities (11–12). These findings highlight a critical distinction: although males and younger individuals (under 65 years) account for the majority of reported cases, females and older adults (≥65 years) exhibit greater physiological vulnerability when exposed to rising temperatures, warranting targeted protective interventions for these populations.
This study has several limitations that warrant consideration. First, the heat-related illness data relied on hospital-based reporting, meaning that not all cases were captured. Some individuals may not seek medical care, and reporting compliance varied across hospitals and local CDCs due to differences in awareness and interest in surveillance activities. Consequently, the current heat-related illness surveillance system may not accurately reflect the true disease burden in certain regions. Second, meteorological data were aggregated at the county level, which may introduce exposure misclassification at the individual level, potentially attenuating the observed temperature-health associations.
Despite these limitations, our findings carry important practical implications for public health policy and practice. It is essential to strengthen preventive measures, enhance public awareness campaigns, and improve emergency response capacity in high-risk PLADs such as Zhejiang, Jiangsu, and Anhui, with particular focus on vulnerable populations including women and older adults. Although most heat-related illnesses in our dataset were mild, likely reflecting prompt recognition and clinical intervention, the risk of severe outcomes such as heat exhaustion and heat stroke remains substantial during extreme heat events. Implementing comprehensive preventive strategies and ensuring timely access to medical care are critical for reducing morbidity and mortality. Furthermore, local health systems should enhance case reporting procedures to enable early detection of heat-related illness clusters and public health emergencies. Such improvements would facilitate rapid deployment of targeted interventions in affected regions and ultimately reduce the population-level health burden associated with extreme heat exposure.
HTML
| Citation: |

|