
 Download:
Download:




-
Introduction: School-aged children are primary vectors for influenza transmission through their frequent close contact in educational settings and developing immune awareness. Since 2019, the Shenzhen municipal government has implemented annual, free, influenza vaccination programs targeting eligible primary and secondary school students. However, evidence-based strategies specifically tailored to this demographic remain insufficient.
Methods: This study analyzed weekly influenza-like illness (ILI) surveillance data and laboratory-confirmed positivity rates from Shenzhen during the 2023–2024 season. It developed an age-stratified Susceptible–Exposed–Symptomatic–Asymptomatic–Recovered–Hospitalized–Deceased–Vaccinated compartmental model integrated with the Ensemble Adjustment Kalman Filter (EAKF) algorithm to estimate historical transmission parameters and quantify vaccination impact. The Upper Confidence Bound applied to Trees (UCT) algorithm was used to optimize the vaccination schedule and evaluate multiple strategic scenarios comparatively.
Results: Compared to a no-vaccination scenario, the current government strategy prevented approximately 1,285,925 [95% confidence interval (CI): 1,240,671–1,331,180] symptomatic infections and 56,956 (95% CI: 55,118–58,793) hospitalizations. Under identical vaccine supply conditions, the optimized strategy recommends vaccinating 30%, 25%, and 5% of school-aged children in November, December, and January, respectively. This optimized approach would avert approximately 1,469,368 (95% CI: 1,392,734–1,546,002) symptomatic infections and 64,442 (95% CI: 61,269–67,615) hospitalizations — representing 14.3% and 13.1% improvements over the government strategy, respectively. Additionally, a generic strategy developed using 2017–2019 data performed well during 2023–2024, demonstrating cross-seasonal adaptability.
Conclusions: Concentrating influenza vaccination efforts among school-enrolled children during November and December significantly reduces disease burden and represents a critical strategy for controlling influenza transmission.
-
Influenza represents a significant acute respiratory infectious disease that poses substantial public health challenges worldwide. Educational institutions, characterized by dense student populations, limited mobility patterns, and frequent close interpersonal contact, constitute particularly high-risk environments for influenza transmission and outbreaks (1). School-aged children demonstrate heightened susceptibility to viral infection compared to adults and, once infected, typically exhibit prolonged viral shedding periods with higher viral loads (2). These epidemiological characteristics underscore the critical importance of implementing targeted, evidence-based countermeasures within school settings. Among available pharmaceutical interventions, vaccination remains the most effective strategy for preventing influenza-related infections (3).
Since 2019, Shenzhen’s vaccination program has provided free influenza vaccinations to school-aged children, typically implementing these programs during October and November each year. Despite extensive research on influenza vaccination optimization strategies (4-5), the evidence base supporting vaccination decisions for this specific population remains limited, creating a gap between theoretical recommendations and practical implementation for school-based programs.
To assess the epidemiological impact of school-based vaccination programs, this study analyzed influenza transmission patterns in Shenzhen during the 2023–2024 season and compared observed outcomes with simulated scenarios assuming no vaccination intervention. This study utilized weekly ILI+ proxy data spanning August 2023 to July 2024, along with vaccination coverage data provided by the Shenzhen Center for Disease Control and Prevention (CDC), to estimate reductions in infections and hospitalizations attributable to vaccination (
Supplementary Material andSupplementary Figure S1 ). The ILI+ proxy integrates influenza-like illness (ILI) rates with laboratory-confirmed positivity rates, providing a comprehensive measure of influenza activity that captures both clinical presentation and virological confirmation. To reconstruct historical influenza transmission dynamics, this study implemented an age-specific Susceptible – Exposed – Symptomatic – Asymptomatic – Recovered – Hospitalized – Deceased – Vaccinated (SEYARHDV) compartmental model, which effectively characterizes viral spread across different population segments (Supplementary Material ,Supplementary Figure S2 , andSupplementary Table S1 ). By coupling this transmission model with the Ensemble Adjustment Kalman Filter (EAKF) algorithm (6), this study estimated time-varying transmission rates and other epidemiological parameters to quantify the public health impact of vaccination programs, specifically measuring reductions in symptomatic infections and hospitalizations (Supplementary Material ).For the optimization process, this study employed the Upper Confidence Bound applied to Trees (UCT) algorithm to identify an optimal vaccination schedule for school-aged children (
Supplementary Material ) (7). To address implementation challenges such as dispersed vaccination timing and uneven distribution patterns, it introduced a smoothness constraint to ensure gradual policy rollout and prevent abrupt strategic shifts. The optimization framework begins each September — coinciding with the academic year commencement — and spans a 12-month period with monthly decision intervals, aiming to minimize annual influenza-related hospitalizations. Based on the vaccination strategy implemented by the Shenzhen government, as documented by the Shenzhen CDC for 2023–2024, this study established an annual vaccination rate of 60% for children aged 6–18 years. Each month offers 6 vaccination options: 0%, 5%, 10%, 25%, 30%, or 45%, permitting up to 45% of school-aged children to receive vaccination monthly. For other age groups (0–5 years, 19–59 years, and ≥60 years), monthly and annual vaccination rates align with actual vaccination data from 2023 to 2024. Under the baseline strategy — where annual vaccination rates are distributed evenly across months — school-aged children receive a consistent monthly vaccination rate of 5%, while other groups maintain their default settings. Vaccines are administered uniformly throughout each day. Additional experimental details are provided inSupplementary Material .For the 2023–2024 period, this study fitted the SEYARHDV model and found that the influenza season extended from September 2023 to May 2024, with a peak ILI+ proxy of 0.0665 (Figure 1A). In a simulated scenario without vaccination, the projected peak ILI+ proxy increased dramatically to 0.2728, demonstrating the critical importance of vaccination in epidemic control. The Shenzhen vaccination program prevented approximately 1,285,925 (95% CI: 1,240,671–1,331,180) symptomatic infections and 56,956 (95% CI: 55,118–58,793) hospitalizations in 2023–2024. By comparison, the baseline vaccination strategy prevented only 704,669 (95% CI: 669,089–740,249) symptomatic infections and 32,175 (95% CI: 30,641–33,709) hospitalizations, demonstrating substantially lower effectiveness than the government’s approach. Using the same vaccine supply, the optimized strategy recommended vaccinating 30%, 25%, and 5% of school-aged children in November, December, and January, respectively. This optimized approach could prevent 1,469,368 (95% CI: 1,392,734–1,546,002) symptomatic infections and 64,442 (95% CI: 61,269–67,615) hospitalizations. Compared to the government’s vaccination strategy, the optimized approach achieved a 14.3% greater reduction in symptomatic infections and a 13.1% greater reduction in hospitalizations, demonstrating superior effectiveness in controlling influenza transmission. Figure 1B illustrates the differences in ILI+ proxy trends across vaccination strategies. Similar analyses were conducted using 2017–2019 data, with results provided in
Supplementary Material andSupplementary Figure S3 .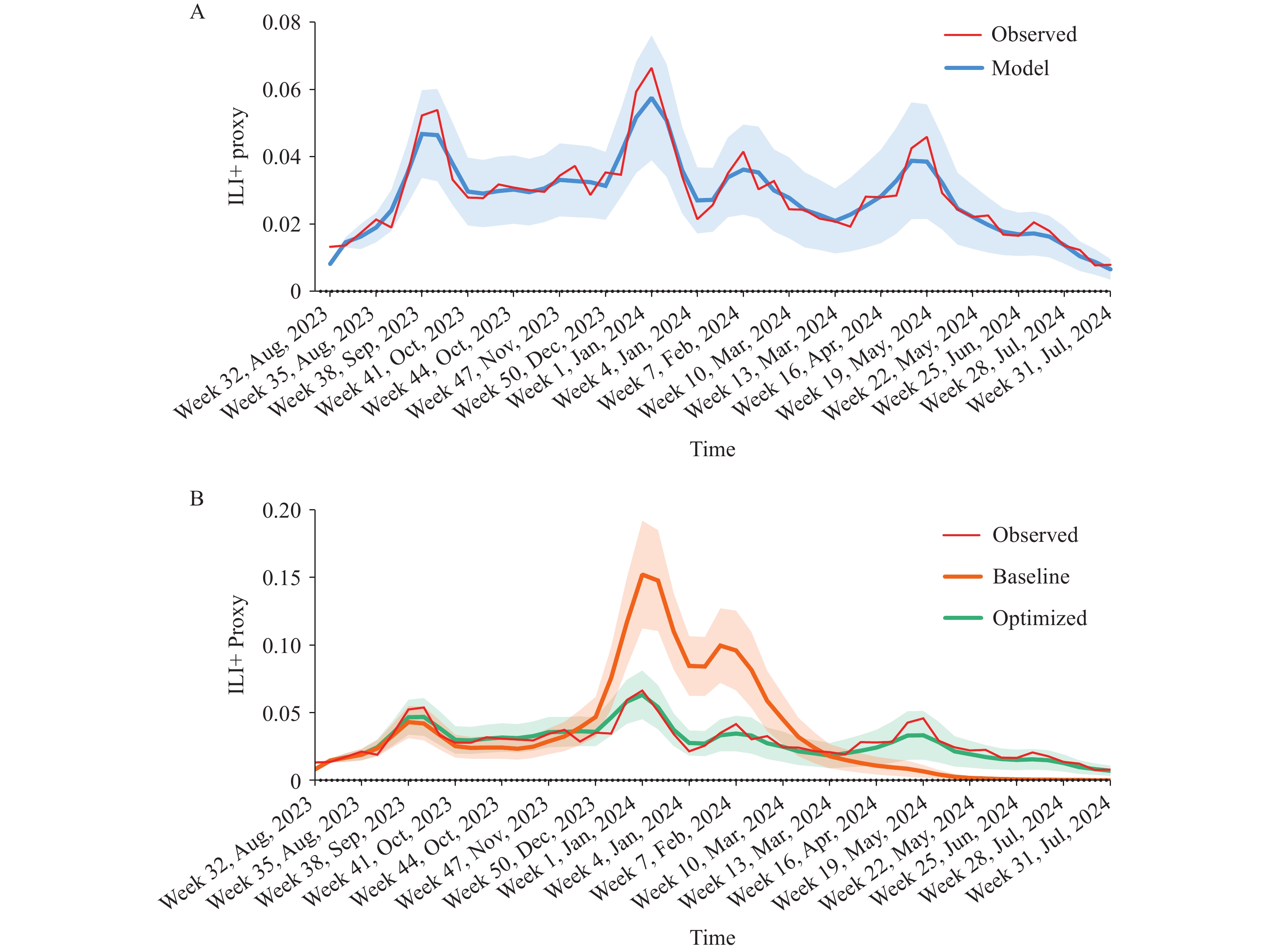 Figure 1.
Figure 1.Model fitting and simulation of influenza activity under different vaccination strategies, Shenzhen, 2023–2024. (A) Observed ILI+ proxy from surveillance data (red) and corresponding model fitting results (blue line with shaded 95% CI). (B) Comparison of observed ILI+ (red) with model-simulated outcomes under two strategies: baseline (orange) and optimized (green), shown as lines with shaded 95% CIs.
Note: All scenarios assume the same annual vaccine coverage. For school-aged children, only the monthly distribution differs; other age groups follow actual 2023–2024 rates.
Abbreviation: CI=confidence interval; ILI+=influenza-positive proportion.
To develop a vaccination strategy applicable to future influenza seasons, this study sought to derive an optimal approach using historical data that could be applied to prospective scenarios. It optimized vaccination strategies for the 2017–2018 and 2018–2019 influenza seasons using data from 2017 to 2019 (
Supplementary Material ). A comprehensive, universal strategy was obtained by calculating a weighted average of the optimization results from these two seasons, which recommended vaccinating 15% and 45% of school-aged children in October and November, respectively. When this strategy was applied to the 2023–2024 influenza season, it potentially reduced symptomatic infections by 1,187,407 (95% CI: 1,150,194–1,224,620) and hospitalizations by 52,924 (95% CI: 51,408–54,439). Although this strategy’s effectiveness was slightly lower than the government-enforced strategy, it demonstrated robust performance, making it suitable for vaccination policy recommendations. The difference in effectiveness can be attributed to significant variations in transmission patterns across different influenza seasons. For instance, the 2017–2018 influenza season was predominantly confined to the winter-spring period with relatively low case numbers, while the 2018–2019 season experienced significant outbreaks in both winter-spring and summer periods. In contrast, the 2023–2024 season extended from summer and autumn to the following spring and summer, with a higher overall peak. These findings suggest that future strategy optimization should incorporate more comprehensive historical data and predictions about influenza transmission levels. A universal strategy optimized using data from seasons with similar transmission patterns would likely prove more effective and better suited to adapting to the dynamic nature of influenza transmission.To better understand how different age groups contribute to the observed vaccination effectiveness, this study conducted additional simulations by sequentially removing vaccination coverage for each age group while maintaining coverage for all others. This approach allowed the quantification of the marginal impact of each age group on overall disease burden during the 2023–2024 season. The results demonstrated that removing vaccination for the 6–18 year group led to the most substantial increase in disease burden, resulting in an estimated 3,823,546 (95% CI: 3,513,522–4,133,570) symptomatic infections and 175,283 (95% CI: 162,422–188,143) hospitalizations — substantially higher than any other age group. In comparison, removing vaccination for the 0–5 year group resulted in 2,679,188 (95% CI: 2,406,184–2,952,192) symptomatic infections and 128,517 (95% CI: 116,848–140,186) hospitalizations. Removing vaccination for the 19–59 year group yielded 2,719,808 (95% CI: 2,444,489–2,995,128) symptomatic infections and 130,408 (95% CI: 118,631–142,185) hospitalizations. Finally, removing vaccination for the ≥60 year group led to 2,677,089 (95% CI: 2,404,110–2,950,069) symptomatic infections and 130,414 (95% CI: 118,546–142,282) hospitalizations. These findings highlight that while all age groups contribute to overall protection, the marginal impact of vaccinating school-aged children is notably greater in reducing population-level transmission and disease burden. This result aligns with both theoretical expectations and practical implementation, as the Shenzhen vaccination program has primarily targeted school-aged children and achieved the highest coverage in this demographic.
-
The spread of influenza has created severe health challenges among school-aged children. This demographic faces heightened susceptibility to cross-infection within school environments due to their limited self-protection awareness and frequent close peer interactions (8). Such intensive contact not only facilitates within-school transmission but also significantly amplifies community-level spread. Infected children often serve as vectors, carrying the virus into their households and triggering cascading consequences, including parental absenteeism and secondary infections among family members. Research demonstrates that for every 10 students absent from school due to influenza, approximately 8 household members subsequently become ill, with illness rates within 3 days of school absence being 2.2 times higher than expected during the influenza season (9). This evidence confirms that school-aged children frequently serve as primary introducers of influenza into households. Consequently, vaccinating school-aged children not only reduces their individual disease burden but also disrupts transmission pathways between schools and households, helping to curb broader community-level spread and thereby alleviating the overall public health and socioeconomic burden of seasonal influenza.
Although school-aged children are not traditionally considered the primary target of influenza vaccination, many countries now recommend including them in immunization programs as an extension of existing plans (10). This shift reflects growing recognition of their central role in influenza transmission. In Shenzhen, influenza vaccination is available to all individuals aged 6 months and older, with free vaccinations currently accessible only to school-aged children and elderly individuals aged 60 and above. Others who intend to receive vaccinations need to voluntarily visit clinics at their own expense for preventive immunization. It is worth noting that influenza vaccination for the elderly is also entirely voluntary. Hence, this study investigated the public health benefits of vaccination policies and examined optimal strategies for vaccinating school-aged children. Its findings underscore the importance of vaccination timing and coverage, highlighting the advantages of well-planned public health interventions.
This study has several limitations that should be acknowledged. First, its investigation of vaccination strategies did not consider other interventions such as social distancing measures. Second, this study utilized weekly ILI+ proxy data and healthcare-seeking rates to estimate symptomatic incidence in the general population from municipal-scale data, which may introduce biases in attack rate calculations. Third, this study considered only six possible vaccination actions to balance varying vaccination rates while minimizing computational complexity. It also assumed a maximum monthly vaccination rate of 45%, which constrained this study’s action space. Regions can adjust these actions and constraints based on their vaccination capacity and local conditions. Fourth, since unified mass influenza vaccination targets only school-aged children, this study assumed vaccination rates for other age groups remained fixed and focused solely on optimizing the vaccination schedule for school-aged children. However, this methodology can be similarly applied to other regions and age groups.
This study’s findings demonstrate that Shenzhen’s large-scale, targeted vaccination program for school-aged children substantially reduces influenza-related disease burden, including both infections and hospitalizations. The optimization algorithm that this study developed provides a valuable framework for refining vaccination strategies across different settings. While vaccination approaches may require adaptation to specific influenza transmission patterns, concentrating vaccination efforts during November and December consistently proves effective, establishing a robust foundation for future vaccination policies.
HTML
| Citation: |

|