
 Download:
Download:




-
Introduction: Effective detection methods to distinguish between transient human papillomavirus (HPV) infection and clinically relevant high-risk HPV (hrHPV)-induced diseases are lacking, leading to excessive referrals and overtreatment. This study evaluated the clinical performance of a host DNA six-methylation marker panel (ASTN1, DLX1, ITGA4, RXFP3, SOX17, and ZNF671) to triage Chinese women who were hrHPV-positive.
Methods: This prospective multicenter study enrolled women aged 21–65 years with positive hrHPV testing. hrHPV genotyping, cytology, colposcopy, and the six-methylation marker assay were performed. High-grade cervical lesions were defined as histologically confirmed CIN2+. Forest plots analyses were performed to assess the triage performance of the methylation assay.
Results: Of the 1,806 patients recruited from 4 hospitals in China, 1,659 were included. The methylation assay positivity rates were 7.5%, 73.9%, 88.9%, and 100% for CIN1, CIN2, CIN3, and cervical cancer, respectively. The six-methylation marker assay demonstrated sensitivities of 82.2% and 90.3% and specificities of 92.4% and 84.1% for CIN2+ and CIN3+, respectively, which were higher than those of HPV genotype testing and cytology (≥ASCUS) screening; the areas under the curve for CIN3+ detection were 0.87 (0.84–0.90), 0.68 (0.64–0.72), and 0.64 (0.60–0.69), respectively. The six-methylation marker assay showed the lowest colposcopy referral rate (24.2%) and required the fewest referrals for detection, with 1.32 and 2.39 referrals per CIN2+ and CIN3+ cases, respectively. In women aged <30 years, the six-methylation marker assay had the highest specificity for CIN2+ (95.7%) and a sensitivity and specificity for CIN3+ of 80.8% and 88.9%, respectively. It had the lowest referral rate (17.17%) and colposcopy referrals, with 1.24 and 2.43 per CIN2+ and CIN3+ cases, respectively.
Conclusions: The host DNA six-methylation marker assay is a reliable triage tool for women who are hrHPV-positive, providing evidence supporting the application of methylation markers in China.
-
Cervical cancer is the second most common gynecological malignancy that causes death among female patients, with approximately 529,800 new cases and 275,100 deaths annually worldwide. Notably, China accounts for 28% of global cases and 50% of new cases in Asia each year, representing 25%–33% of the annual deaths in Asia (1). Persistent infection with hrHPV is considered the primary cause of cervical cancer and its precancerous lesions. However, HPV genotype testing demonstrates a low specificity of only 31.8% for CIN3 and worse (2). This is because most HPV infections are transient and clear naturally, especially in women younger than 30 years, who have regression rates of 60% (3). Therefore, given China’s large population and the substantial number of women who test HPV-positive annually, a reliable triage tool for high-grade intraepithelial lesions (HSIL) is urgently needed.
Ideal triage strategies require a balance between safety, sensitivity, specificity, and screening-related burden; however, a consensus on the optimal triage test is lacking. Various triage methods have been proposed, including p16/Ki-67 cytological dual staining and methylation assays. While p16/Ki-67 staining demonstrates 90% sensitivity for CIN3+, its limited specificity (42%) fails to reduce colposcopy referral rates (4). A meta-analysis showed that the sensitivity and specificity of all methylation assays for CIN3+ were 0.708 and 0.780, respectively (5). Among these, a methylation panel comprising six markers (ASTN1, DLX1, ITGA4, RXFP3, SOX17, and ZNF671) is suitable for application in developing countries due to its superior specificity (88.7%–94.6%) for CIN3+ (3,6). However, data for this methylation panel come only from clinical trials conducted in Western countries, and the prevalence and distribution of HPV genotypes in China differ from those in Western countries, with significantly higher infection rates of HPV52 and HPV58. Furthermore, the applicability of the positive threshold of this methylation panel to Chinese women and differences in the expression of methylation markers are unclear.
Therefore, this study hypothesized that the methylation pattern in China might be distinct and conducted a prospective multicenter study to evaluate the clinical performance of a host DNA six-methylation marker panel in Chinese women who were hrHPV-positive. This was the first prospective multicenter study in China with a large sample size to evaluate the feasibility of the six-methylation marker assay as a triage tool for hrHPV-positive women.
Overall, 1,806 women from the colposcopy clinics of 4 hospitals across China underwent HPV genotype testing, cytological screening, methylation assays, and colposcopy between August 2018 and April 2021. The participating institutions included Peking University First Hospital, Nanjing Drum Tower Hospital, Hunan Provincial Maternal and Child Health Care Hospital, and The First Affiliated Hospital of Anhui Medical University, representing 4 different provinces. The inclusion criteria were as follows: 1) women aged 21–65 years with an intact cervix, 2) hrHPV-positive status with available cervical cytology results, and 3) cervical lesions confirmed through colposcopy biopsy. The exclusion criteria were as follows: 1) pregnant, maternal, or lactating women; 2) unwillingness to participate or inability to provide informed consent; and 3) a history of cervical cancer. This study received ethical approval from all 4 participating hospitals (ethics approval numbers: JNFL2020001, 2020-180-04, JNFL2018001, and PJ 2021-02-06).
Samples were obtained by experienced gynecologists using a cervical brush. Cytology screening employed the liquid-based cytology (LBC) method, and the diagnosis was classified into 5 levels according to the 2014 Bethesda System (TBS) criteria. HPV genotype testing was performed using fluorescence quantification PCR, and results were categorized into 2 groups: HPV16/18-positive and positive for the other 12 hrHPV genotypes, i.e., “other-hrHPV positive.” Host DNA from LBC samples was heavy sulfite-transformed for methylation analyses. The methylation panel comprised 6 gene markers: DLX1, ASTN1, ITGA4, RXFP3, SOX17, and ZNF671. All procedures were performed according to standardized instructions. ZNF671 was assigned a score of 3 points, while the other 5 methylation markers were assigned 1 point each. The six-methylation marker assay was considered positive if the cumulative score across all 6 markers was ≥3. All HPV genotyping and methylation assays were conducted in a central laboratory. All women underwent colposcopy, and cervical biopsies were performed based on colposcopic impressions. Cervical lesions were histologically classified as CIN1/2/3 or cervical cancer (CC), while those with normal biopsy results or colposcopic impressions were categorized as “normal.”
This study evaluated 5 triage strategies for detecting CIN2+ and CIN3+ in hrHPV-positive women using histopathology as the gold standard. The evaluated strategies were as follows: 1) HPV16/18 genotyping; 2) cytology (≥ASCUS); 3) six-methylation marker assay; 4) six-methylation marker assay and HPV16/18 co-screening; and 5) six-methylation marker assay and cytology (≥ASCUS) co-screening. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), area under the receiver operating characteristic curve (AUC), and forest plots were calculated for each method. Statistical analyses were performed using SPSS (version 26.0, IBM Corp., NY, USA) and R (version 4.1.2, R Core Team, Vienna, Austria). Independent-sample t-tests were used to compare normally distributed continuous data, whereas nonparametric continuous variables were analyzed using the Mann-Whitney test. Categorical variables were assessed using the chi-squared or Fisher’s exact test. To compare methylation marker scores among different CIN groups that followed a non-normal distribution, this study employed the Kruskal-Wallis test, followed by Dunn’s test for pairwise comparisons. Two-sided P<0.05 were considered significant.
Finally, 144 cases did not meet the inclusion criteria, and 3 cases were excluded due to unsuccessful methylation detection, resulting in 1,659 cases available for final analysis, as shown in Figure 1. Assessment using a mixed-effects model showed no significant center effect (P>0.05) on baseline characteristics or CIN2+/CIN3+ detection rates. Data from all centers were therefore pooled for final analysis. The study flowchart is presented in Figure 1.
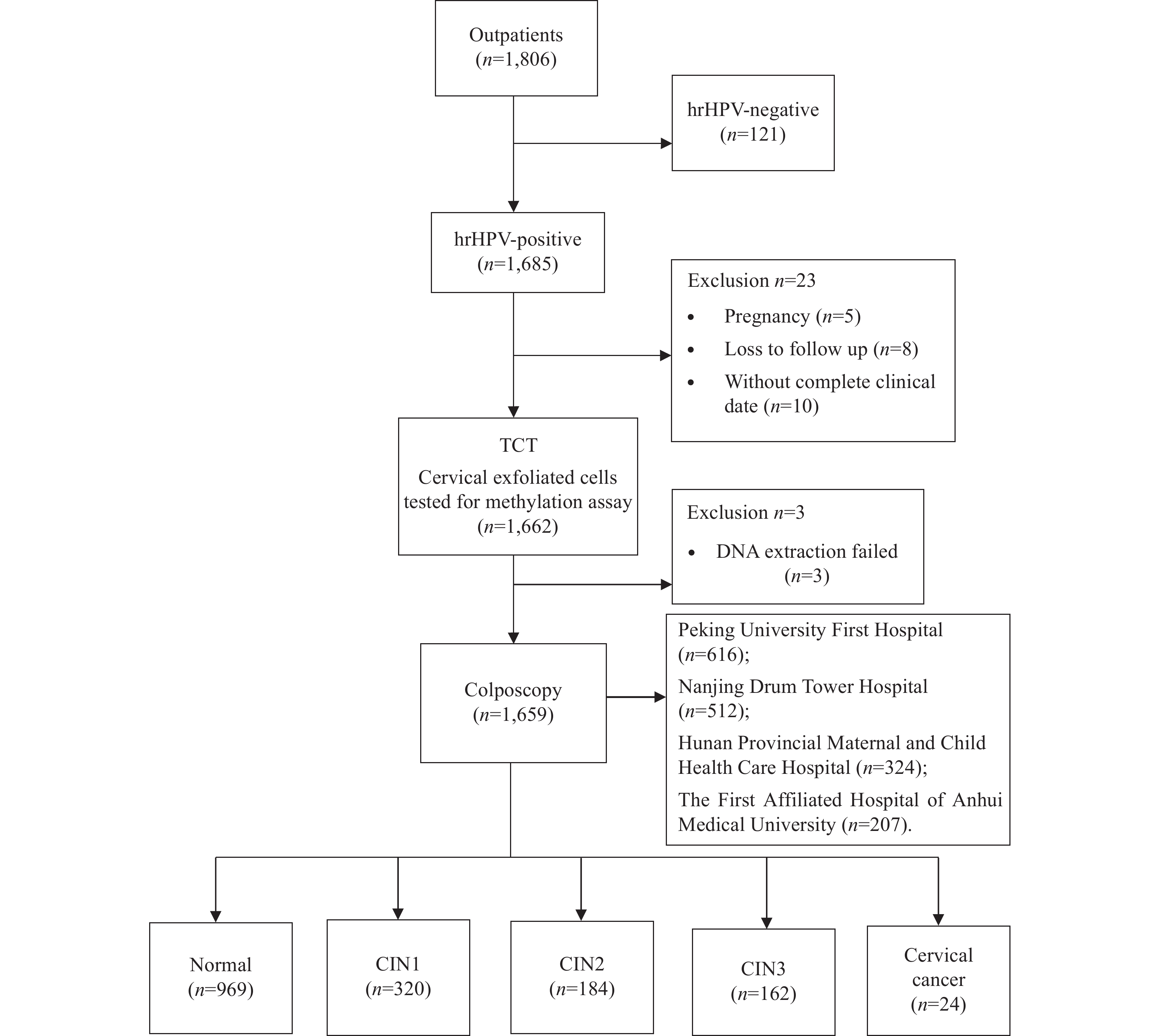 Figure 1.
Figure 1.Study flowchart of women who were hrHPV-positive.
Abbreviation: HPV=human papillomavirus; TCT=ThinPrep Cytologic Test; CIN=cervical intraepithelial neoplasia.The mean patient age was 41.3 years (range: 21–65). Histopathological findings included 320 (19.3%), 184 (11.1%), 162 (9.8%), and 24 (1.4%) cases of CIN1, CIN2, CIN3, and CC, respectively. Among all cases, 37.1% (259/690) were HPV16/18-positive. The methylation assay demonstrated positivity rates of 7.5% (24/320), 73.9% (136/184), 88.9% (144/162), and 100% (24/24) for CIN1, CIN2, CIN3, and CC, respectively. The methylation scores increased significantly with the severity of cervical lesions (P<0.05). Characteristics of the CC screening and methylation assays are presented in Table 1.
Items Normal CIN1 CIN2 CIN3 CC Total P Number (n, %) 969 (58.4) 320 (19.3) 184 (11.1) 162 (9.8) 24 (1.4) 1,659 − Age (years, mean±SD) 42.6±10.5 38.9±10.4 39.6±9.8 42.2±10.3 41.2±10.1 41.3±10.4 0.69 hrHPV results (n, %) HPV 16/18 291 (30.0) 70 (21.9) 77 (41.8) 89 (54.9) 20 (83.3) 547 (33.0) 0.01* Other-hrHPV 678 (70.0) 250 (78.1) 107 (58.2) 73 (45.1) 4 (16.7) 1,112 (67.0) Cytology results (n, %) Normal 576 (59.4) 118 (36.9) 36 (19.6) 23 (14.2) 2 (8.3) 755 (45.5) <0.001* ≥ASCUS 393 (40.6) 202 (63.1) 148 (80.4) 139 (85.8) 22 (91.7) 904 (54.5) Methylation (n, %) Positive 74 (7.6) 24 (7.5) 136 (73.9) 144 (88.9) 24 (100) 402 (24.2) <0.001* Negative 895 (92.4) 296 (92.5) 48 (26.1) 18 (11.1) 0 (0) 1,257 (75.8) Score (mean±SD) 0.6±1.3 0.60±1.4 3.6±2.5 4.6±2.2 5.7±2.4 1.5±2.3 <0.001* Methylation in women <30 years of age (n, %) Positive 4 (2.8) 6 (6.7) 20 (51.3) 16 (76.2) 5 (100.0) 51 (17.2) <0.01* Negative 138 (97.2) 84 (93.3) 19 (48.7) 5 (23.8) 0 (0) 246 (82.8) Score (mean±SD) 0.9±1.2 1.4±2.4 1.4±2.1 2.0±2.6 2.6±3.4 1.3±2.2 0.04* Note: “−” means "Not Applicable".
Abbreviation: HPV=human papillomavirus; CIN=cervical intraepithelial neoplasia; CC=cervical cancer; ASCUS=atypical squamous cells of undetermined significance; SD=standard deviation.
* P<0.05.Table 1. Cervical screening and six-methylation marker assay for cervical precancerous lesions and cervical cancer.
The 3 most frequently positive methylation markers in the CIN2+ and CIN3+ groups were ZNF671 (65.8% vs. 88.2%), DLX1 (43.5% vs. 68.3%), and ASTN1 (37% vs. 61.3%). In the CIN1 group, DLX1 showed the highest positivity rate (21.6%). However, as the cervical lesions progressed in severity from CIN1 to CIN2, the positive methylation rate of ZNF671 increased dramatically by 59.2%, which was substantially higher than that of the other markers (
Supplementary Table S1 ). The proportion of samples testing positive for all 6 markers increased from 2.3% in CIN1 to 11.4% in CIN2 and 24.1% in CIN3+. The mean numbers of positive markers in the CIN2, CIN3, and CC groups were 2.5, 3.5, and 4.6, respectively.The six-methylation marker assay as a single triage tool demonstrated a sensitivity of 82.2% for CIN2+ and a specificity of 92.4%. This sensitivity was significantly higher than that of HPV16/18 genotyping but comparable to that of cytology (≥ASCUS), while its specificity was the highest among all 3 methods. For CIN3+, the six-methylation marker assay achieved a sensitivity of 90.3% and a specificity of 84.1% (Table 2).
Triage algorithms Sensitivity (%) n/N
95% CISpecificity (%) n/N
95% CIPPV (%) n/N
95% CINPV (%) n/N
95% CICompared with HPV16/18 Compared with cytology Relative sensitivity (95% CI) Relative specificity (95% CI) Relative sensitivity (95% CI) Relative specificity (95% CI) For CIN2+ HPV16/18 50.3
(45.2–55.4)72.0
(69.5–74.4)34.0
(30.0–38.0)83.5
(81.3–85.6)1.00 1.00 0.60
(0.54–0.66)1.34
(1.29–1.38)Cytology
(≥ASCUS)83.5
(79.7–87.3)53.8
(51.1–56.6)34.2
(31.1–37.3)91.9
(90.0–93.9)1.66
(1.58–1.74)0.75
(0.71–0.79)1.00 1.00 Methylation 82.2
(78.3–86.1)92.4
(91.0–93.8)75.6
(71.4–79.8)94.7
(9.3.5–96.0)1.63
(1.56–1.71)1.28
(1.26–1.30)0.98
(0.94–1.03)1.72
(1.69–1.74)Methylation or HPV16/18 92.2
(89.4–94.9)67.5
(64.9–70.1)44.9
(41.3–48.4)96.8
(95.6–97.9)1.83
(1.78–1.89)0.94
(0.90–0.97)1.10
(1.07–1.14)1.25
(1.21–1.30)Methylation or cytology 94.6
(92.3–96.9)50.3
(47.6–53.1)35.4
(32.4–38.3)97.0
(95.7–98.3)1.88
(1.83–1.93)0.70
(0.66–0.74)1.13
(1.11–1.16)0.93
(0.88–0.99)For CIN3+ HPV16/18 58.6
(51.5–65.7)70.3
(67.9–72.6)19.9
(16.6–23.3)93.1
(91.6–94.6)1.00 1.00 0.68
(0.59–0.76)1.42
(1.37–1.46)Cytology
(≥ASCUS)86.6
(81.7–91.5)49.6
(47.0–52.1)17.8
(15.3–20.3)96.7
(95.4–98.0)1.48
(1.39–1.56)0.71
(0.67–0.74)1.00 1.00 Methylation 90.3
(86.1–94.6)84.1
(82.2–86.0)41.8
(37.0–46.6)98.6
(97.9–99.2)1.54
(1.47–1.61)1.20
(1.17–1.27)1.04
(0.99–1.09)1.70
(1.66–1.73)Methylation or HPV16/18 96.8
(94.2–99.3)60.6
(58.1–63.1)23.7
(20.7–26.7)99.3
(98.8–99.9)1.65
(1.61–1.69)0.86
(0.83–0.90)1.12
(1.09–1.15)1.22
(1.17–1.27)Methylation or cytology 96.8
(94.2–99.3)45.0
(42.5–47.6)18.2
(15.8–20.6)99.1
(98.4–99.8)1.65
(1.61–1.69)0.64
(0.60–0.68)1.12
(1.09–1.15)0.91
(0.86–0.96)Abbreviation: PPV=positive predictive value; NPV=negative predictive value; AUC=area under the receiver operating characteristic curve; HPV=human papillomavirus; ASCUS=atypical squamous cells of undetermined significance; CI=confidence interval. Table 2. Performance of different triage tools for the detection of CIN2+/CIN3+ among women who were hrHPV-positive.
The AUCs of HPV16/18 genotyping, cytology (≥ASCUS), and the six-methylation marker assay for CIN2+ and CIN3+ were 0.61 and 0.64, 0.69 and 0.68, and 0.87 and 0.87, respectively. Combining the six-methylation marker assay with HPV16/18 genotyping (≥ one positive) as a triage tool for CIN2+/3+ resulted in a higher sensitivity but a lower specificity compared to HPV16/18 genotyping alone. The relative sensitivity and specificity with HPV16/18 genotyping and cytology (≥ASCUS) as the reference strategy for CIN2+ and CIN3+ are shown in Figures 2 and 3.
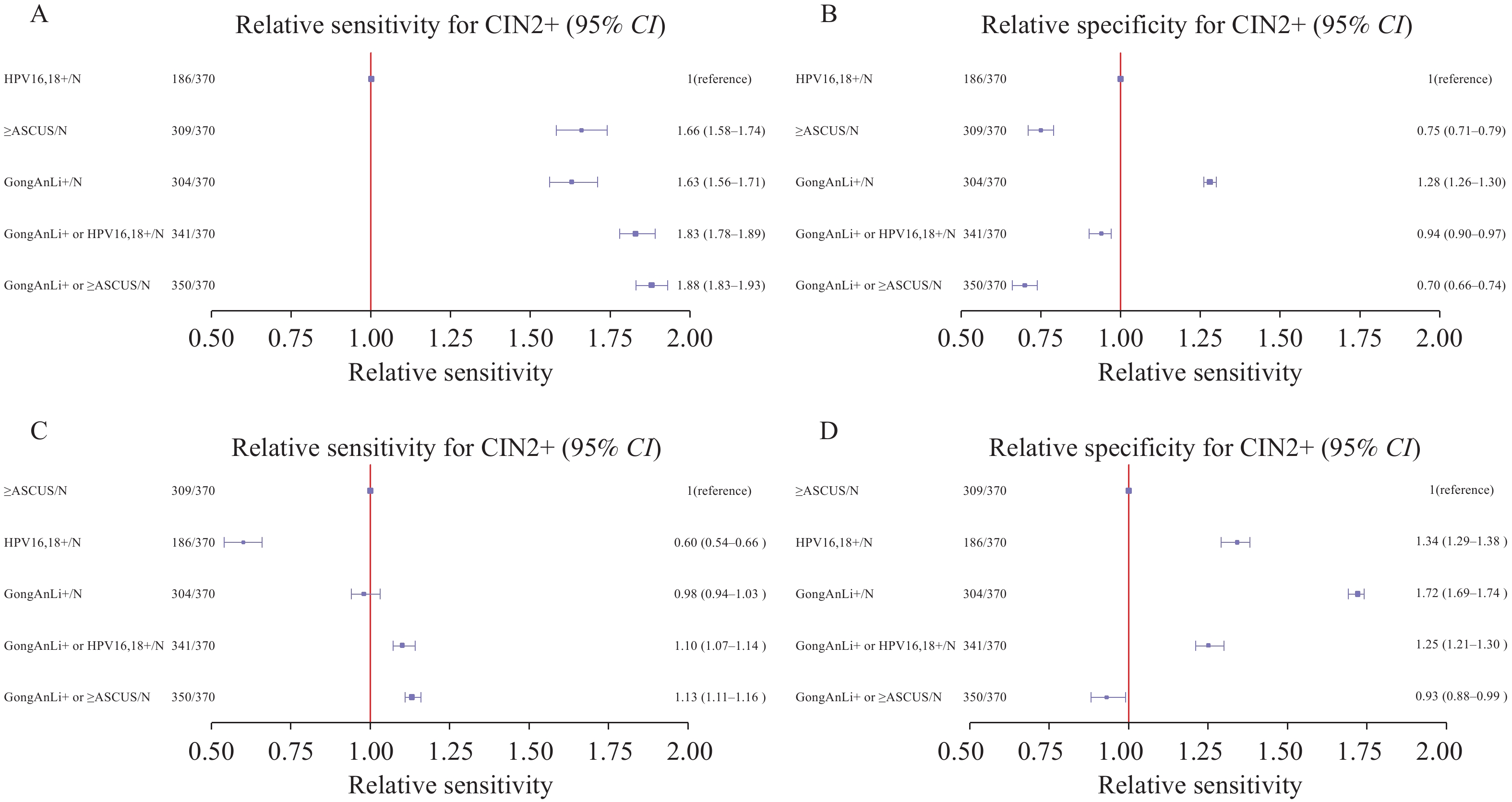 Figure 2.
Figure 2.Forest plots showing the relative sensitivity and specificity for CIN2+ detection of different triage tools compared with HPV16/18 genotyping and cytology (≥ASCUS). The relative (A) sensitivity and (B) specificity of different triage tools compared with HPV16/18 genotyping; The relative (C) sensitivity and (D) specificity of different triage tools compared with cytology (≥ASCUS).
Abbreviation: CIN2+=cervical intraepithelial neoplasia grade 2 or worse; HPV=human papillomavirus; ASCUS=atypical squamous cells of undetermined significance.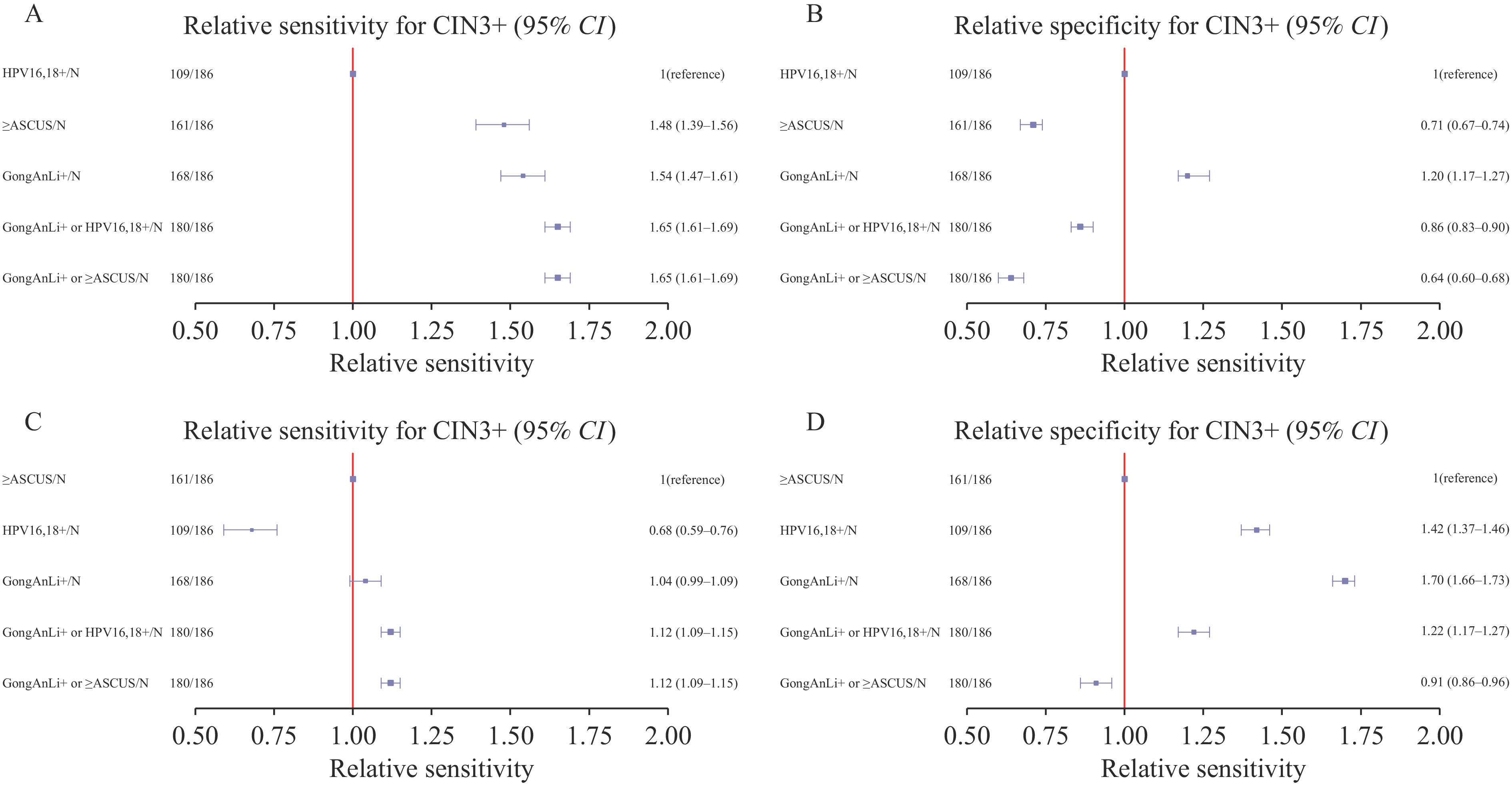 Figure 3.
Figure 3.Forest plots showing the relative sensitivity and specificity for CIN3+ detection of different triage tools compared with HPV 16/18 genotyping and cytology (≥ASCUS). (A) The relative sensitivity of different triage tools compared with HPV 16/18 genotyping; (B) The relative specificity of different triage tools compared with HPV 16/18 genotyping; (C) The relative sensitivity of different triage tools compared with cytology (≥ASCUS); (D) The relative specificity of different triage tools compared with cytology (≥ASCUS).
Abbreviation: CIN2+=cervical intraepithelial neoplasia grade 2 or worse; HPV=human papillomavirus; ASCUS=atypical squamous cells of undetermined significance.This study further analyzed the efficacy of different triage tools in women aged <30 years. The DNA methylation positivity rate among women who were <30 years of age and hrHPV-positive was 17.2% (51/297), which was lower than that among women >30 years of age (25.8%). The combination of the six-methylation marker assay and cytology had the highest sensitivity for CIN2+ (89.2%). However, the six-methylation marker assay showed the highest specificity (95.7%), with relative specificities of 1.34 and 1.8 compared to HPV genotyping and cytology (≥ASCUS), respectively. For CIN3+ detection, the six-methylation marker assay demonstrated relatively good sensitivity and specificity, with values of 80.8% and 88.9%, respectively (
Supplementary Table S2 ). Notably, it also demonstrated the highest specificity among the 5 triage strategies in the overall cohort for the detection of CIN2+ or CIN3+, particularly in the subgroup analysis of women <30 years of age for CIN2+ (Table 2 andSupplementary Table S2 ).In addition, the six-methylation marker assay demonstrated the lowest colposcopy referral rate (24.23%) and the fewest referrals required for detection, with 1.32 and 2.39 referrals per CIN2+ and CIN3+ cases, respectively. In contrast, HPV16/18 genotyping and cytology (≥ASCUS) required approximately 3 referrals each per CIN2+ case, and 5.02 and 5.61 referrals per CIN3+ case, respectively. In the subgroup analysis of women <30 years of age, the six-methylation marker assay also demonstrated the lowest colposcopy referral rates (17.17%) and colposcopy referrals (
Supplementary Table S3 ). -
Due to China’s large population, many women who are hrHPV-positive require annual colposcopy referrals. Currently, the main triage techniques used for women who are hrHPV-positive in China are cytology and hrHPV genotype testing. However, cytology has a relatively low sensitivity (50%–70%) for HSIL detection (7), and hrHPV genotype testing cannot distinguish between transient and persistent HPV infections, all resulting in clinical overtreatment.
Consequently, numerous DNA methylation genes have been reported as promising markers for HSIL detection. Sofia et al. conducted a meta-analysis of 23 studies examining DNA methylation-based biomarkers in women who are hrHPV-positive (8) and found that DNA methylation assays demonstrated a sensitivity of 0.78 (95% CI: 0.74–0.82) and specificity of 0.74 (95% CI: 0.69–0.78) for CIN3+. The previous methylation assay comprising 6 markers (ASTN1, DLX1, ITGA4, RXFP3, SOX17, and ZNF671) in Germany has been implemented clinically with a sensitivity of 67.7% (95% CI: 57.3%–77.1%) and specificity of 88.7% (95% CI: 83.7%–92.6%) for CIN3+ (3) and shows a much higher specificity than another assay that simultaneously detects p16 and Ki-67 via immunocytochemistry (6). However, it has not been recommended by WHO guidelines (9) and requires additional clinical research to verify its value. Furthermore, its applicability in Chinese women remains unknown.
To this study’s knowledge, this is the first prospective multicenter study, and is using the largest cohort, to evaluate a six-methylation marker panel in women who are hrHPV-positive. Although this study’s methylation panel shared the same 6 gene markers as a previous methylation panel from Germany, the scoring algorithms differed significantly. The positive threshold for the previous methylation panel was 0.5, with individual marker contributions as follows: DLX1 (0.1), ASTN1 (0.2), ITGA4 (0.2), RXFP3 (0.2), SOX17 (0.2), and ZNF671 (0.5); the cutoff value of the six-methylation marker panel in this study was 3. This finding may correlate with the variations in HPV genotype prevalence and distribution between Chinese and Western women, suggesting that Chinese women may exhibit different DNA methylation patterns. Nevertheless, this study confirmed that this six-methylation marker panel demonstrated significantly higher sensitivity and specificity for CIN3+ compared to HPV genotyping and cytology (≥ASCUS), supporting its potential as a reliable triage tool.
Previous studies have predominantly focused on evaluating the triage efficacy of methylation assays for CIN3+, with limited attention given to CIN2. However, CIN2 has a higher regression rate in clinical practice, especially in young women (<30 years of age) (3). Dippmann et al. compared the performance of the six-methylation marker assay with that of the QIAsure Methylation Test using 195 cervical scrapes from Western countries (1) and found that the six-methylation marker assay exhibited significantly higher specificity for CIN2+ (87.6% vs. 67.4%; P<0.001). In another study involving 396 cervical lesions, the specificity of the six-methylation marker assay for CIN2+ was 51.6%, which was higher than those of both HPV genotype testing (21.5%) and cytology (≥ASCUS) (45.2%) (10). In contrast to prior small-sample studies, this large-scale, prospective, multicenter study further validated the reliable triage performance of the six-methylation marker assay for CIN2+, even in women <30 years of age, which had the highest specificity and provided critical evidence to guide the clinical management of women with CIN2+. These findings align with those reported by Vink et al., who found that the FAM19A4/miR124-2 Methylation Test provided superior specificity compared to HPV16/18 genotyping for CIN2/3 detection in women aged <30 years (11). This suggests that follow-up without immediate intervention may be safe for young women who are methylation-negative. However, these hypotheses warrant further investigation.
Furthermore, this study found that the positivity rate of the six-methylation marker assay was significantly lower in young women. This age-dependent detection rate was confirmed in another study using a six-methylation marker assay in Western countries, although in that study, only 30% of women <30 years of age with CIN2/3 were methylation-positive compared to 70% in the older group (P=0.004) (1). This may be related to the high prevalence of transient HPV infections and higher regression rates of CIN2 lesions in younger women. This study also analyzed the methylation levels of six methylation markers and found that ZNF671 had the highest positivity rate (81.6%) in patients who were with CIN3+. Another real-time methylation-specific PCR analysis of ZNF671 showed the highest detection rates for cervical scrapes with CIN3 (71%) and cancer (97.3%) (10), and the ZNF671 methylation test showed superior performance compared to PAX1 for CIN3+ detection (12). This finding suggests that ZNF671 plays a particularly important role in the positive determination of methylation assays for HSIL detection. Additionally, this study observed that the host DNA methylation positivity rates and methylation scores in women with CIN1 and without CIN were similar and significantly lower than those in women with CIN2+ and CIN3+. This indicates that the DNA methylation assay can effectively distinguish patients with HSIL from women without HSIL.
This study also assessed cost-effectiveness by comparing the colposcopy referral rates across five triage strategies. The six-methylation marker assay performed best in both the overall population and in younger women who were hrHPV-positive, suggesting its potential to reduce CC screening costs, minimize unnecessary colposcopies, and lower the national healthcare burden while decreasing patient discomfort and infection risks from repeated procedures.
In conclusion, the host DNA six-methylation marker assay demonstrated relatively superior triage performance for both overall and young (<30 years) women who were hrHPV-positive, significantly reducing colposcopy referrals and making it a cost-effective and reliable triage strategy. Based on this study’s findings, its authors hypothesize that the host DNA six-methylation marker assay may serve as an alternative to cytology, particularly for women who are hrHPV-positive and have ASCUS/LSIL (Low-grade Squamous Intraepithelial Lesion) cytology or non-16/18 HPV genotypes in regions with limited availability of cytologists or colposcopists. Its implementation may reduce reliance on cytology quality and minimize unnecessary colposcopies and overtreatment. Further prospective studies are required to validate the feasibility of these clinical applications.
The findings in this report are subject to at least four limitations. First, cervical lesions were not followed-up long term. Although the methylation assay serves as a crucial tool for investigating HPV integration into the host DNA, it cannot directly differentiate between persistent and transient HPV infections. Long-term follow-up is required to further elucidate the relationships among methylation, HPV infection, and persistent CIN lesion. Second, although methylation testing reduces false-positive costs, the technical complexity and infrastructure requirements pose challenges for implementation in resource-limited settings, necessitating standardized protocols and training programs. Third, to minimize analytical variability, HPV genotyping and methylation assays were conducted in a central laboratory; however, potential confounding factors include inter-center differences in cytology interpretation and colposcopy practices and sample selection bias. Finally, this study focused exclusively on women who were hrHPV-positive, and the findings may not be generalizable to women who are HPV-negative or populations without prior HPV screening, highlighting the need for larger cohort studies to refine these results.
-
All the participants in this study.
HTML
| Citation: |

|