
 Download:
Download:




-
Introduction: The 13-valent pneumococcal conjugate vaccine (PCV13) has reduced vaccine-type carriage rates, though regarding serotype replacement remain.
Methods: This study conducted a 2-year prospective cohort study (February 2023–February 2025) in Suqian, Jiangsu Province, enrolling 2-month-old infants and monitoring for acute respiratory infections (ARIs). Pharyngeal swabs collected during ARIs were analyzed using targeted next-generation sequencing (tNGS) to identify respiratory pathogens, and Streptococcus pneumoniae (S. pneumoniae)-positive samples were serotyped using multiplex PCR. Risk ratios (RRs) for S. pneumoniae detection were estimated using Poisson regression, with sensitivity analysis performed using inverse probability of treatment weighting (IPTW).
Results: Among 579 children, 1,527 swabs were collected, yielding an overall S. pneumoniae detection incidence of 35.2%. Vaccinated children receiving 3–4 PCV13 doses demonstrated significantly lower detection rates than unvaccinated children [23.1% vs. 40.2%; adjusted RR=0.70; 95% confidence interval (CI): 0.50, 0.98; P=0.036]. IPTW analysis confirmed these findings. Non-vaccine serotypes predominated, particularly the 10A and 15A/15F strains.
Conclusion: PCV13 vaccination was associated with reduced S. pneumoniae detection among children with ARIs, despite dominance of non-vaccine serotypes. Our findings emphasize the importance of ongoing surveillance for S. pneumoniae and highlight the need to expand the serotype coverage of pneumococcal vaccines.
-
Streptococcus pneumoniae (S. pneumoniae) represents a major bacterial pathogen responsible for significant infections and mortality among children under five years of age. Nasopharyngeal colonization serves not only as the primary reservoir for horizontal transmission within communities but also as an essential prerequisite for invasive disease development (1). Young children serve as the principal reservoir, with point prevalence estimates of nasopharyngeal colonization ranging from 27% to 85% (2). The introduction of pneumococcal conjugate vaccines (PCVs) has substantially reduced the incidence of vaccine-type carriage and pneumococcal disease among young children. However, the selective pressure exerted by vaccination has fundamentally altered the microbial landscape, resulting in an increased prevalence of non-vaccine serotypes, with a growing proportion of infections now attributed to replacement serotypes, such as 8, 10A, 12F, 15A, and 24F (3). In recent years, global interest has intensified regarding the protective effects of PCVs and the associated changes in pneumococcal serotype distribution across diverse populations. Therefore, based on a prospective acute respiratory infection (ARI) surveillance cohort in eastern China, the present study aimed to evaluate the impact of PCV13 vaccination on the risk of S. pneumoniae detection and characterize the current distribution of predominant pneumococcal serotypes among young children.
This study was based on a prospective cohort of healthy infants established in February 2023 in Suqian, Jiangsu Province, Eastern China, as previously reported (4). Briefly, infants aged 2 months at recruitment were enrolled and actively monitored for ARI episodes over 24 months. Demographic data and baseline pharyngeal swabs were collected at enrollment. During the surveillance, the researchers contacted caregivers biweekly via telephone to monitor their health status. When a child exhibited ARI symptoms such as cough, nasal congestion, tachypnea, or throat redness and swelling, researchers conducted home visits within 48 hours to collect pharyngeal swabs. Trained healthcare personnel collected pharyngeal swabs. With the child’s head tilted slightly backward, a disposable flocked swab was inserted into the posterior pharyngeal wall and tonsillar areas, rotated 3–5 times, and immediately placed in a tube containing the viral transport medium. All specimens were transported on dry ice and stored at −80 °C prior to laboratory testing.
Pharyngeal swab specimens were analyzed using the Respiratory Pathogen Detection Kit (KS608-100HXD96, KingCreate, Guangzhou, China) for targeted next-generation sequencing (tNGS), which can identify 107 respiratory pathogens, including S. pneumoniae, Mycoplasma pneumoniae, and influenza A and B viruses. Detailed tNGS procedures are provided in the
Supplementary Material . Serotyping was performed using multiplex PCR for specimens that tested positive for S. pneumoniae. DNA extraction and analysis of the amplified products from earlier surveys have been described previously (4). PCV13 vaccination status during the follow-up period was obtained from the National Immunization Information System.All statistical analyses were conducted using the R Software (version 4.4.1; The R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics, including medians, interquartile ranges (IQRs), and percentages, were calculated to summarize the baseline characteristics of the study population. Categorical variables were compared using the Chi-square test, and continuous variables were compared using the Mann-Whitney U test. We compared the overall incidence of S. pneumoniae detection in PCV13-vaccinated and unvaccinated children. Risk ratios (RRs) were estimated using Poisson regression with robust standard errors by PCV13 doses, and adjusted RRs were obtained after controlling for sex, disease history, mode of delivery, maternal age at delivery, maternal education level, maternal monthly income, number of household members, presence of children under 18 years of age in the household, monthly household income, and baseline S. pneumoniae carriage. We employed inverse probability of treatment weighting (IPTW) using propensity scores to reconstruct comparable cohorts of PCV13-vaccinated and unvaccinated individuals for sensitivity analysis to examine the impact of PCV13 on the detection of S. pneumoniae. The reduction in pneumococcal occurrence attributable to vaccination was calculated as (1−adjusted RR)×100%. For samples with failed serotyping, multiple imputations were applied using chained equations. Missing serotype values were imputed using classification and regression tree methods to generate 20 imputed datasets. The results from all the imputed datasets were subsequently combined using Rubin’s rules. A two-sided P value of <0.05 was considered statistically significant.
Of the 796 children enrolled in the longitudinal ARI surveillance cohort study, 579 (72.7%) provided at least one valid pharyngeal swab sample during an ARI episode and were included in the present analysis. The baseline demographic characteristics of the 579 participants did not differ significantly from those of the overall cohort (
Supplementary Table S1 ). Among the included children, 310 (53.5%) were boys, 21 (3.6%) carried S. pneumoniae at enrollment, and 54 (9.3%) received one dose of PCV13 before enrollment (Table 1).Characteristics Participants included in the analysis Infant sex, n (%) Female 269 (46.5) Male 310 (53.5) Infant age, median (IQR), days 71.0 (66.0, 78.0) Infant height, median (IQR), cm 60.0 (59.0, 62.0) Infant weight, median (IQR), kg 6.3 (5.8, 6.8) Infant birth length, median (IQR), cm 50.0 (50.0, 50.0) Infant birth weight, median (IQR), kg 3.4 (3.2, 3.7) Infant disease history*, n (%) Yes 18 (3.1) No 561 (96.9) Maternal mode of delivery, n (%) Full-term vaginal delivery 291 (50.3) Cesarean delivery 288 (49.7) Maternal feeding pattern, n (%) Breastfeeding 523 (90.3) Not breastfeeding after birth 47 (8.1) Mixed feeding 9 (1.6) Maternal age, n (%), years <35 503 (86.9) ≥35 76 (13.1) Maternal education, n (%) Middle school or below 162 (28.0) High school or vocational school 100 (17.3) Junior college 152 (26.3) Bachelor's degree or above 165 (28.5) Maternal monthly income, n (%), CNY <1,000 245 (42.3) 1,000–6,999 270 (46.6) ≥7,000 64 (11.1) No. of household members, n (%) ≤4 421 (72.7) >4 158 (27.3) With household members <18 years of age, n (%) Yes 329 (56.8) No 250 (43.2) Monthly household income, n (%), CNY <10,000 175 (30.2) ≥10,000 404 (69.8) Baseline S. pneumoniae carriage Yes 21 (3.6) No 553 (95.5) Missing 5 (0.9) Received first dose of PCV13 before enrollment, n (%) Yes 54 (9.3) No 525 (90.7) Abbreviation: PCV13=13-valent pneumococcal conjugate vaccine; CNY=Chinese Yuan; COVID-19=coronavirus disease 2019.
* Infant disease history includes pneumonia, jaundice, COVID-19, and lactose intolerance.Table 1. Baseline demographic characteristics of 579 participants analyzed in this study.
During the study period, 2,996 ARI episodes were recorded, yielding an incidence rate of 196.6 episodes per 100 person-years (95% CI: 189.5, 203.6). A total of 1,527 pharyngeal swab samples were collected from 579 participants. Among them, 204 tested positive for S. pneumoniae at least once, with an overall detection rate of 35.2% (95% CI: 31.3%, 39.1%). Overall, 181 (31.3%) children received 1–4 doses of PCV13, whereas 398 (68.7%) remained unvaccinated. Notably, PCV13 vaccination was not associated with a reduction in the overall ARI incidence (Table 2).
PCV13 vaccination status Person years No. of events Rate (95% CI) Incidence rate ratio (95% CI) P Unvaccinated 819 1,676 204.6 (194.8, 214.4) Reference − 1–2 doses 78 150 191.9 (161.2, 222.6) 0.94 (0.79, 1.10) 0.448 3–4 doses 294 591 201.0 (184.8, 217.2) 0.98 (0.89, 1.08) 0.695 Note: The incidence rate ratio and 95% CI were estimated using Poisson regression models with log (person-years) as the offset.
Abbreviation: PCV13=13-valent pneumococcal conjugate vaccine; CI=confidence interval.Table 2. Incidence of acute respiratory infection episodes per 100 person-years by PCV13 vaccination status.
For each of the 204 children with S. pneumoniae, one positive sample was randomly selected for serotyping analysis. Of these, 137 (67.2%) were successfully serotyped. Among the 137 successfully serotyped samples, 105 (76.6%) contained a single serotype, 26 (19.0%) contained two serotypes, and 6 (4.4%) contained three serotypes. The most frequently detected non-vaccine serotypes were 10A (30.3%) and 15A/15F (22.3%), with 23F (3.4%) being the most common (Figure 1). For samples for which serotyping failed, we additionally applied multiple imputations that showed a consistent serotype distribution. The detection rates of most non-vaccine serotypes were higher in unvaccinated children than in vaccinated children. Statistically significant differences were observed for serotypes 10A (P=0.041) and 15A/15F (P=0.003) based on the Pearson’s Chi-square test, whereas no significant differences were detected for the other serotypes (Figure 2).
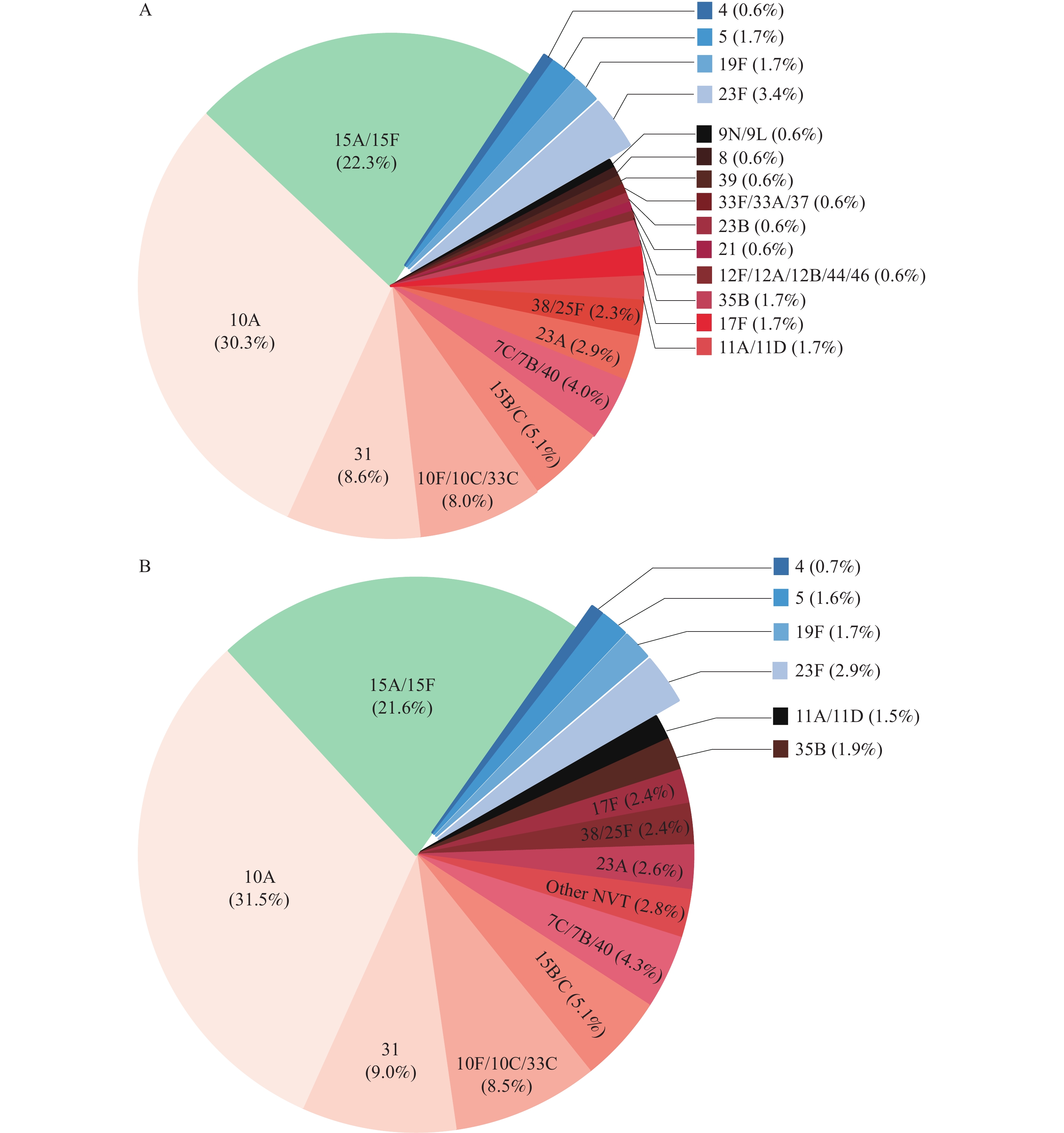 Figure 1.
Figure 1.Distribution of pneumococcal serotypes during ARI episodes among children. (A) Serotype distribution of Streptococcus pneumoniae detected during ARI episodes; (B) Serotype distribution of Streptococcus pneumoniae after multiple imputation.
Note: In panels A and B, the vaccine serotypes are highlighted in blue. Other NVT included 12F/12A/12B/44/46, 21, 23B, 33F/33A/37, 39, 8, and 9N/9L.
Abbreviation: NVT=non-vaccine serotypes; ARI=acute respiratory infection.
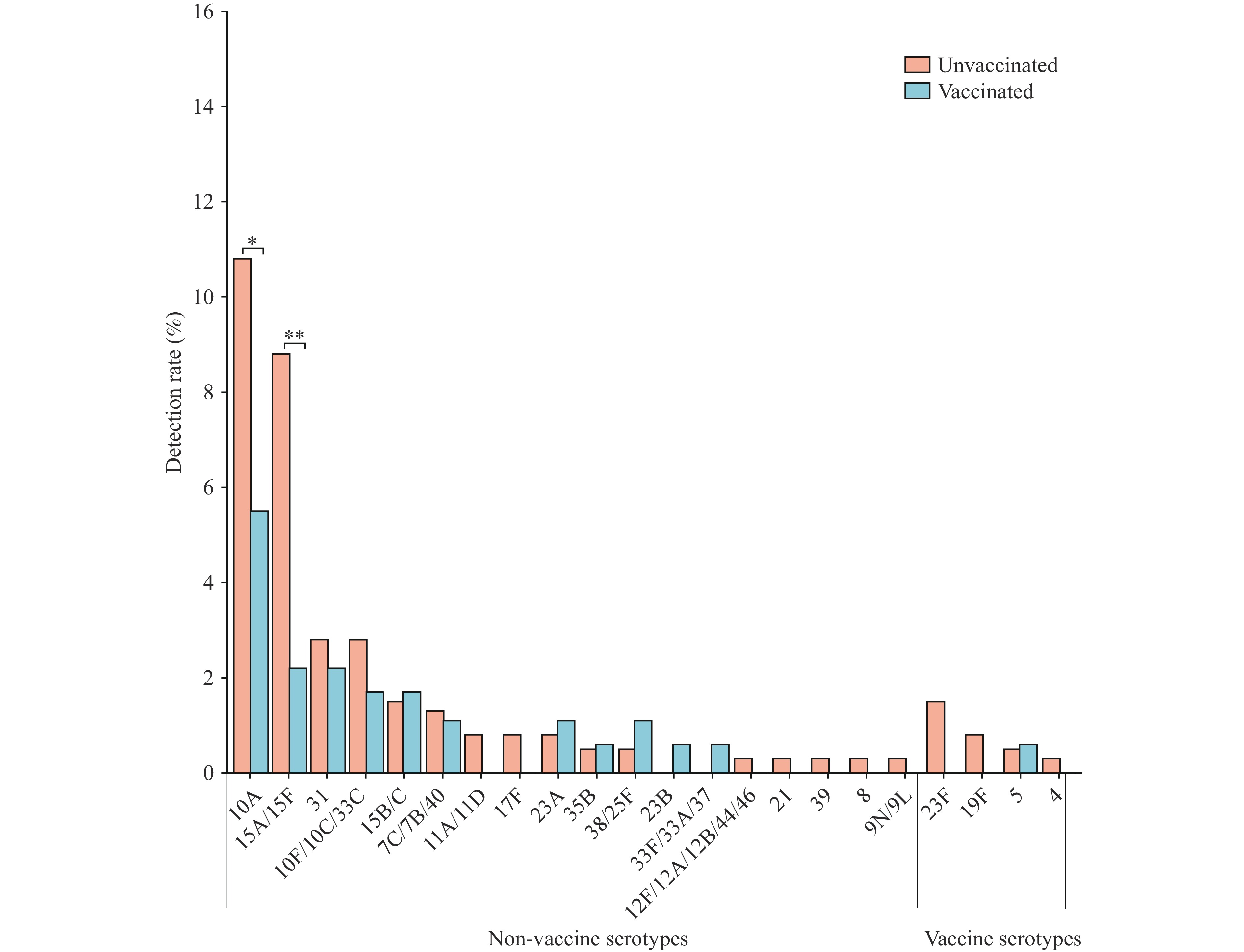 Figure 2.
Figure 2.Detection rates of vaccine-type and non-vaccine serotypes during ARI episodes.
Abbreviation: ARI=acute respiratory infection.Among children in the overall pneumococcal group, those who received 1–2 doses of PCV13 demonstrated an incidence of S. pneumoniae detection of 28.9% (95% CI: 15.4%, 45.9%), compared to 40.2% (95% CI: 35.3%, 45.2%) in unvaccinated children, with an adjusted RR of 0.80 (95% CI: 0.49, 1.32; P=0.392) (Table 3). In contrast, children who received 3–4 doses exhibited a 30.2% reduction in S. pneumoniae detection (adjusted RR=0.70; 95% CI: 0.50, 0.98; P=0.036). A significant 39.0% reduction in non-vaccine-type S. pneumoniae detection was also observed in this group (adjusted RR=0.61; 95% CI: 0.38, 0.97; P=0.037) (Table 3). Owing to the limited sample size, no significant effect of PCV13 was observed on vaccine-type S. pneumoniae detection, although point estimates suggested some differences. Sensitivity analyses using IPTW yielded consistent results, demonstrating a 61.9% reduction in non-vaccine-type S. pneumoniae detection (RR=0.38; 95% CI: 0.23, 0.64; P<0.001) (Table 3).
Pneumococcal
typePCV13 vaccination
statusn/N (%) Cumulative incidence
(%, 95% CI)Unadjusted RR
(95% CI)P
(unadjusted)Adjusted RR
(95% CI)*P
(adjusted)Original cohort All pneumococci Unvaccinated 160/398 (40.2) 40.2 (35.3, 45.2) Reference − Reference − 1–2 doses 11/38 (28.9) 28.9 (15.4, 45.9) 0.74 (0.44, 1.23) 0.260 0.80 (0.49, 1.32) 0.392 3–4 doses 33/143 (23.1) 23.1 (16.4, 30.9) 0.57 (0.41, 0.78) 0.001 0.70 (0.50, 0.98) 0.036 Vaccine serotypes Unvaccinated 12/398 (3.0) 3.0 (1.6, 5.2) Reference − Reference − ≥1 dose 1/181 (0.6) 0.6 (0.0, 3.0) 0.18 (0.02, 1.36) 0.096 0.29 (0.04, 2.39) 0.251 Non-vaccine serotypes Unvaccinated 99/398 (24.9) 24.9 (20.7, 29.4) Reference − Reference − 1–2 doses 7/38 (18.4) 18.4 (7.7, 34.3) 0.75 (0.38, 1.48) 0.408 0.78 (0.41, 1.49) 0.454 3–4 doses 18/143 (12.6) 12.6 (7.6, 19.2) 0.50 (0.31, 0.79) 0.003 0.61 (0.38, 0.97) 0.037 IPTW cohort† All pneumococci Unvaccinated 222/578 (38.4) 38.4 (33.5, 43.3) Reference − − − 1–2 doses 152/530 (28.7) 28.7 (13.3, 44.0) 0.75 (0.43, 1.30) 0.299 − − 3–4 doses 124/573 (21.6) 21.6 (13.9, 29.2) 0.56 (0.39, 0.82) 0.003 − − Non-vaccine serotypes Unvaccinated 138/578 (23.9) 23.9 (19.7, 28.2) Reference − − − 1–2 doses 82/530 (15.5) 15.5 (4.4, 26.6) 0.65 (0.31, 1.35) 0.247 − − 3–4 doses 52/573 (9.3) 9.1 (4.8, 13.5) 0.38 (0.23, 0.64) <0.001 − − Note: Data are presented as n/N (%) unless otherwise specified.
Abbreviation: ARI=acute respiratory infection; PCV13=13-valent pneumococcal conjugate vaccine; RR=risk ratio; CI=confidence interval; IPTW=inverse probability of treatment weighting.
* Adjusted for sex, disease history, mode of delivery, maternal age at delivery, maternal education level, maternal monthly income, number of household members, presence of children under 18 years old in the household, monthly household income, and baseline S. pneumoniae carriage.
As there were no cases in the 1–2 dose group and only one case in the 3–4 dose group, the two groups were combined for analysis.
† Weighted analysis was performed using IPTW estimated from multinomial logistic regression. The weighted results for vaccine serotypes were not estimated because of the small number of events. For the IPTW cohort, n/N values represent the sum of the IPTW weights and not the actual sample size.Table 3. Cumulative incidence and risk ratios of pneumococcal detection during ARI episodes by PCV13 vaccination status in the original and IPTW cohorts.
-
This study evaluated the impact of PCV13 vaccination on the detection of S. pneumoniae among children with ARI through a comprehensive 24-month active surveillance program. During the follow-up period, the overall incidence of S. pneumoniae detection was 35.2%. Children who received 3–4 doses of PCV13 demonstrated a significantly reduced risk of S. pneumoniae detection compared with their unvaccinated counterparts, with particularly pronounced reductions observed for non-vaccine serotypes 10A and 15A/15F.
The detection rate of S. pneumoniae observed in our cohort was 35.2%, exceeding that reported in previous studies of healthy children under 5 years of age (30.4%) (5) and the pooled prevalence estimate from a recent meta-analysis of Chinese children (21.4%) (6). This elevated detection rate can be attributed to our prospective cohort design, which enabled the comprehensive identification of ARI episodes and the implementation of tNGS, a highly sensitive molecular technique that achieves superior detection rates compared with traditional culture-based methods.
Our findings demonstrated that PCV13 vaccination significantly reduced the risk of pneumococcal detection during childhood, particularly among children who completed the 3–4 dose immunization series, reflecting the direct protective effect of the vaccine on vaccinated individuals. However, no significant effect was observed on the overall incidence of ARI. Unlike previous studies that primarily focused on vaccine serotypes, our results suggest that PCV13 vaccination may also be associated with a reduced detection of non-vaccine serotypes. Following the introduction of PCVs, vaccine-type serotypes are markedly suppressed, whereas non-vaccine serotypes may not colonize efficiently, and therefore may not fully occupy the niche vacated by vaccine types, leaving ecological space for competing colonizers (7). In a randomized controlled trial on PCV7, a negative association in co-colonization between S. pneumoniae (both vaccine-type and non-vaccine serotypes) and Staphylococcus aureus was observed (8).
Our results also revealed that non-vaccine serotypes of S. pneumoniae were predominant over vaccine serotypes, with serotypes 10A and 15A/15F being the most prevalent, whereas vaccine serotypes accounted for only 7.4%. These findings are consistent with previously reported patterns. In Ulaanbaatar, Mongolia, a 44% reduction in vaccine-type carriage was observed following PCV13 vaccination, with serotypes 15A and 10A being the dominant serotypes (9). In Hong Kong, serogroup 15 has been reported to be the most frequently detected (10). Furthermore, a meta-analysis conducted between 2017 and 2024 identified 15A as the major non-vaccine serotype in Chinese children (11). Notably, the study reported 19F as the most prevalent serotype, which differed from our findings. This discrepancy may reflect differences in specimen types; the analysis included sterile site specimens and bronchoalveolar lavage fluid, which better represent serotypes causing clinical disease, whereas our study focused on ARI cases with mild symptoms, likely reflecting serotypes circulating within the community.
PCV immunization reduces the individual carriage of vaccine-type S. pneumoniae, thereby diminishing the transmission of these serotypes within the community (12). Although serotype replacement occurs frequently, these emerging serotypes generally exhibit a lower invasive potential, resulting in a net benefit from vaccination with important public health implications. Long-term monitoring remains essential to determine whether vaccine-driven reductions in invasive pneumococcal persist and whether the invasive potential of non-vaccine serotypes remains stable or evolves as vaccine coverage expands.
The study had some limitations. First, although we evaluated the overall impact of PCV13 on pneumococcal detection, the small number of vaccine-type cases limited comprehensive subgroup analyses. Second, a substantial proportion of samples (32.8%) could not be serotyped, likely because of methodological factors. Multiplex PCR requires adequate template DNA, which makes low-load samples identified by tNGS more prone to serotyping failure. Moreover, some untypeable samples may have resulted from the limited serotype coverage of the PCR primers. Finally, our study was conducted exclusively in Eastern China, and given the regional variations in epidemiological patterns and transmission dynamics, our findings may not be fully generalizable to ARI populations in other geographic regions.
In conclusion, PCV13 vaccination reduced pneumococcal detection in children with ARI, highlighting the importance of complete early immunization. As serotype shifts occur, continuous surveillance is essential for guiding strategic adjustments and evidence-based control policies.
-
The Scientific Review Committee of Jiangsu Provincial Center for Disease Control and Prevention approved the study protocol (approval number: JSJK2022-B014-02).
HTML
| Citation: |

|