

 Download:
Download:




-
Introduction: On August 6, 2025, the Yiwu CDC received notification of a suspected mpox case. Subsequent laboratory testing confirmed mpox virus (MPXV, Clade Ib) infection, prompting the initiation of a comprehensive multi-level epidemiologic investigation.
Methods: Between August 6–10, 2025, provincial, municipal, and county expert teams conducted systematic case finding, interview-based exposure mapping, and linkage analysis of public security and border records to reconstruct contact trajectories. The investigation included comprehensive contact tracing, environmental sampling, and real-time PCR testing of lesion and oropharyngeal specimens for MPXV detection.
Results: Six laboratory-confirmed cases were identified with symptom onset dates spanning July 23 through August 6. Five patients received treatment in Yiwu, while one was managed in Changzhou. The cases were predominantly male (5/6), with ages ranging from 22–43 years (median 30 years). Four of the six cases were foreign nationals. Investigators identified and monitored 52 core close contacts and 38 general contacts under 21-day health surveillance protocols. Environmental sampling (n=43) conducted at five case residences and personal items yielded 27 positive results (62.8%) for MPXV.
Conclusions: This outbreak represents an imported mpox cluster with subsequent person-to-person transmission occurring primarily through intimate contact. We documented substantial household environmental contamination, emphasizing the critical importance of comprehensive decontamination measures. Rapid case detection, systematic contact management, and terminal disinfection protocols effectively contained further viral spread.
-
Mpox is an emerging zoonotic disease caused by the mpox virus (MPXV), a member of the Orthopoxvirus genus (1). MPXV Clade Ib was first identified in September 2023 in the Democratic Republic of Congo and, following its rapid global dissemination, was declared a Public Health Emergency of International Concern by the WHO in August 2024 (2). Prior to January 2025, all reported mpox cases in China were attributed to Clade IIb; however, five MPXV Clade Ib infections were detected that month, marking the strain’s initial documented entry into the country (3). This clade demonstrates sustained human-to-human transmission, occurring primarily through sexual contact networks (accounting for 72% of cases), household exposure, and community contact, with no evidence supporting airborne transmission (4). Unlike previous clades, MPXV Clade Ib exhibits enhanced virulence, with a case fatality ratio (CFR) of 5.3%. The strain disproportionately affects pediatric populations (67% of cases) and young adults in high-risk groups, including sex workers (5).
This report describes the first documented cluster of MPXV (Clade Ib) infections in Zhejiang Province, originating from an imported case that traveled from Tanzania to Yiwu City. We present the epidemiological, clinical, and virological characteristics of this outbreak and detail the coordinated public health interventions implemented to prevent secondary transmission.
-
On August 6, 2025, the fever clinic at Yiwu Central Hospital notified Yiwu CDC of a male patient (Case 1) presenting with fever and genital rash. Considering Yiwu’s substantial international population mobility and recent global mpox alerts, the attending physician suspected mpox and immediately implemented isolation protocols. Lesion and oropharyngeal swabs were collected and transported to Yiwu CDC, where same-day real-time PCR testing confirmed MPXV DNA positivity. Jinhua CDC verified these results on August 7, prompting immediate notification of the Zhejiang Provincial CDC. A joint investigation team comprising provincial, municipal, and county CDC experts was established that same day.
Epidemiologic interviews revealed that Case 1 had recent sexual contact with a foreign national (Case 2), who had arrived in Yiwu in late July from Tanzania via Guangzhou. Case 2 reported multiple sexual encounters with local individuals between July 23 and August 7. During the subsequent investigation, we defined a “high-risk sexual network” as individuals connected through recent anonymous or casual sexual relationships occurring within the 21-day MPXV incubation period. Network membership was traced through: 1) standardized epidemiological interviews with cases and contacts, including sexual-history modules; 2) verification of travel, residence, and activity patterns via immigration and public-security databases, supplemented with mobile-signaling data when available; and 3) venue-based tracing conducted with community health service centers and managers of high-risk venues (bars, clubs, guesthouses). These findings confirmed that the outbreak originated from an imported case and spread within a confined high-risk sexual network (Figures 1 and 2).
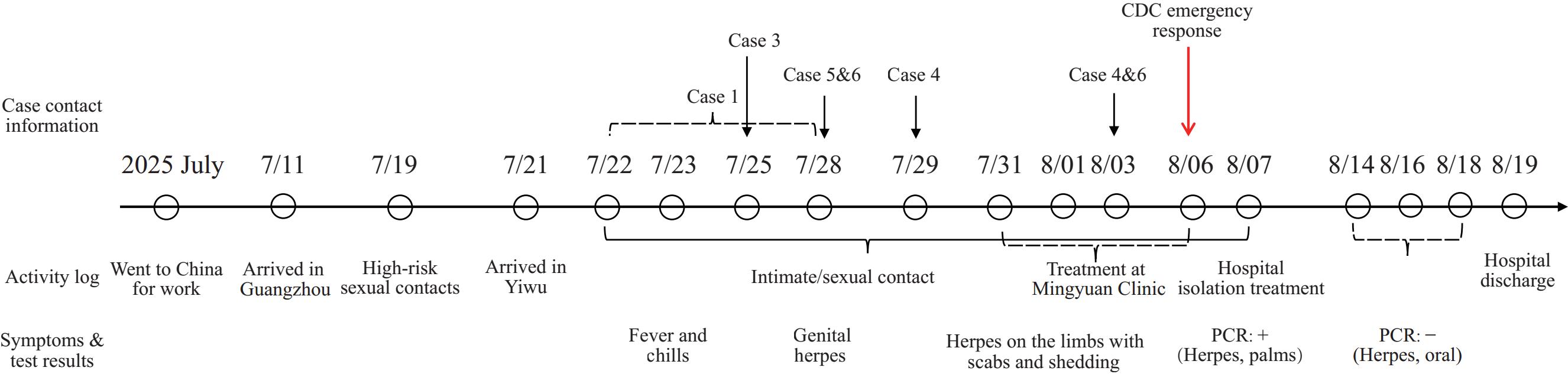 Figure 1.
Figure 1.Travel and movement patterns of Case 2 confirmed by public security and immigration data — Yiwu City, July–August, 2025.
Abbreviation: PCR=polymerase chain reaction. Figure 2.
Figure 2.Schematic diagram of the transmission chain and contact tracing for the mpox Clade Ib cluster — Yiwu City, July–August 2025.
Note: This figure illustrates the 6 laboratory-confirmed mpox cases and all 52 core CCs identified during the investigation. The 52 core contacts comprise 31 individuals with documented sexual contact (either with the imported source Case 2, which represents the cluster’s epidemiological origin, or with other confirmed cases) and 21 individuals with non-sexual prolonged close contact (including shared living spaces and repeated in-person interactions). All core close contacts tested negative for mpox throughout the 21-day health-monitoring period.
Abbreviation: CC=close contact.
We established a working case definition as any individual presenting with acute rash, fever, or lymphadenopathy, with documented epidemiologic linkage to a confirmed or probable case in Yiwu since July 21, and laboratory confirmation of MPXV via PCR from lesion, oropharyngeal, or other clinical samples. Active case finding encompassed reviewing outpatient and inpatient records in dermatology, infectious disease, and fever clinics; systematically interviewing identified contacts; and collaborating with community health stations.
Supplementary Table S1 presents a detailed chronology of case detection, reporting, laboratory confirmation, and public health intervention implementation, demonstrating the response’s timeliness and effectiveness.Between August 6 and 10, six laboratory-confirmed cases (Cases 1–6) were identified. The transmission network, illustrated in
Supplementary Figure S1 , demonstrates that Cases 1 and 3–6 acquired MPXV infection through direct sexual contact with the imported source case (Case 2). Case 2, a female foreign national from Tanzania, was epidemiologically confirmed as the sole source of viral introduction into the network. Table 1 summarizes the demographic and clinical characteristics of all cases. Among the five cases with documented sexual exposure histories, the median interval from last sexual contact to symptom onset was 6 days (range: 5–10 days), consistent with established MPXV incubation periods. Cases were predominantly male (5/6) and aged 22–43 years (median 30 years); four were foreign nationals (from Tanzania, Azerbaijan, and Burkina Faso) and two were Chinese nationals. Clinically, all patients developed cutaneous rash lesions — predominantly affecting genital, perianal, and facial areas — accompanied by fever (100% of cases) and lymphadenopathy (67% of cases). Lesion counts ranged from fewer than 10 to more than 50. No severe complications or fatalities occurred.Transmission branch Case number & name Gender Age
(years)Nationality/
regionYiwu status Sexual contact period
with index caseOnset of
illnessTested
positiveTop node (index) Case 2 Female 27 Tanzanian Entered Guangdong (July 11 2025);
Arrived in Yiwu (July 20 2025)N/A (Index Case) July 23 August 7 Branch 1 Case 1 Male 37 Azerbaijani Arrived in Yiwu (July 8 2025) July 22–July 28 August 1 August 6 Branch 2 Case 3 Male 31 Xinjiang, China Permanent resident in Yiwu July 25 July 31 August 7 Branch 3 Case 4 Male 22 Burkinabe Arrived in Yiwu (May 9 2025) July 29, August 3 August 6 August 8 Branch 4 Case 5 Male 42 Xinjiang, China Traveled between Jiangsu and Yiwu July 28 August 2 August 8 Branch 5 Case 6 Male 38 Tanzanian Permanent resident in Yiwu July 28, August 3 August 3 August 8 Table 1. Demographic and epidemiological characteristics of mpox (Clade Ib) cases in the transmission chain — Yiwu City, July–August 2025.
All patients received treatment at designated hospitals — five in Yiwu and one in Changzhou — where they received symptomatic supportive care, including antipyretics and topical treatments. Isolation was maintained until complete lesion crusting occurred and PCR testing of lesion and oropharyngeal samples returned negative results.
In total, 52 core close contacts and 38 general contacts were identified and placed under 21-day health monitoring. The 52 core close contacts included sexual partners of confirmed cases, household members, and individuals with prolonged close-range exposure; the 38 general contacts comprised primarily healthcare workers from clinics and hospitals where confirmed cases sought medical care. All contacts remaining in Yiwu underwent daily temperature and symptom monitoring for 21 days, with no mpox-compatible symptoms reported during the surveillance period.
-
Laboratory confirmation for all cases relied on PCR testing of lesion and oropharyngeal specimens. Lesion samples consistently demonstrated higher viral loads than oropharyngeal swabs, as evidenced by lower Ct values (27.10±4.48 vs. 30.74±4.00). Notably, Case 6 exhibited positive oropharyngeal PCR results prior to rash onset, with a Ct value of 25.29, confirming that oropharyngeal viral shedding can occur before cutaneous lesion development.
Environmental investigations were conducted from August 7 to 9 in the residences of five cases and on selected personal items. Forty-three environmental surface swabs were collected from bedding, towels, bathroom fixtures, door handles, and electronic devices. The detection results of MPXV nucleic acid in different surface samples are presented in
Supplementary Table S2 . Twenty-seven samples (62.8%) tested positive for MPXV DNA by PCR, with the highest positivity rates observed on bedding and bathroom surfaces. These findings revealed substantial and heterogeneous MPXV contamination throughout home environments, emphasizing the critical importance of comprehensive disinfection protocols.The comprehensive investigation, supported by epidemiological and laboratory evidence, confirmed that this Yiwu cluster originated from an imported mpox case and subsequently spread within a defined high-risk network primarily through intimate and sexual contact.
-
Local health authorities and CDC teams implemented a comprehensive, multi-agency coordinated response to contain the mpox outbreak. Key interventions included: 1) Immediate isolation of confirmed cases in designated hospitals with strict infection prevention and control protocols, coupled with timely clinical management; 2) Systematic environmental disinfection of case residences and personal belongings using chlorine-based disinfectants, followed by verification testing to confirm decontamination effectiveness; 3) Enhanced active surveillance for rash and vesicular illnesses across key healthcare settings, including fever clinics, dermatology departments, and community health centers; and 4) Targeted risk communication and health education delivered in both Chinese and relevant foreign languages, with proactive outreach to high-risk social and sexual networks to promote early care-seeking behaviors and prevention practices.
These coordinated measures successfully interrupted further transmission. No additional cases were detected beyond the identified cluster, and all contacts completed the 21-day medical observation period without developing mpox-compatible symptoms, ultimately leading to formal closure of the outbreak investigation.
-
This investigation documented a cluster of six laboratory-confirmed mpox cases (Clade Ib) in Yiwu City, Zhejiang Province, with one imported source case and five epidemiologically linked secondary cases. This represents the first documented Clade Ib MPXV transmission cluster in Yiwu, China, driven primarily by sexual contact within high-risk networks. The importation pathway is confirmed by the travel history of the source case (Case 2), who arrived from Tanzania — a country with documented endemic circulation of Clade Ib MPXV (6). The outbreak occurred in an international trade hub characterized by substantial cross-border mobility, diverse sexual networks, and dense population settings, creating optimal conditions for rapid person-to-person transmission. Notably, four of the six cases were foreign nationals, highlighting the critical role of global travel in introducing mpox into non-endemic regions.
The epidemiologic pattern reflects recent global outbreaks where close skin-to-skin and sexual contact serve as the primary transmission routes (7). However, the involvement of heterosexual commercial sex in this cluster expands the recognized transmission contexts in China. The attack rate within this defined sexual network was high, consistent with reports documenting efficient Clade Ib transmission within sexual networks from other regions (7-8). Unlike scenarios involving household transmission, particularly to children in endemic areas (7-8), we observed no secondary transmission to household contacts despite extensive environmental contamination. This suggests that while highly transmissible through intimate contact, the effective reproduction number (R-eff) in non-intimate household settings may be lower, potentially influenced by viral load, contact type, and timely decontamination efforts. This contrast emphasizes the importance of context-specific transmission risk assessment. Notably, one case (Case 6) yielded a positive oropharyngeal real-time PCR result before rash onset, suggesting potential pre-symptomatic viral shedding. While this single observation is intriguing, it cannot confirm pre-symptomatic transmission. However, it aligns with clinical guidelines indicating that some cases may be infectious 1–4 days before symptom onset (9). This finding warrants further investigation and underscores the need to re-examine current contact tracing and isolation protocols to account for potential pre-symptomatic transmission (10).
Extensive environmental contamination — identified through PCR positivity on bedding, household surfaces, and personal hygiene items — demonstrates widespread viral DNA distribution and highlights the potential for indirect transmission via contaminated objects (8). This finding reinforces the critical importance of comprehensive environmental decontamination in outbreak response protocols (11). However, it is essential to recognize that PCR detection of viral DNA does not necessarily indicate the presence of viable, infectious virus, which requires confirmation through cell culture methods. The rapid containment achieved through coordinated interventions — including timely case isolation, systematic contact tracing, targeted health education, and thorough environmental disinfection — demonstrates the effectiveness of multi-agency public health responses.
This investigation has several important limitations. First, the small outbreak size limits our statistical power to draw definitive conclusions, particularly regarding the significance of pre-symptomatic oropharyngeal viral shedding observed in one case. Second, the inherently clandestine and anonymous nature of high-risk sexual networks likely resulted in incomplete case detection and underreporting, suggesting our investigation may not have captured the full transmission network. Third, without viral culture performed on environmental samples, we cannot confirm whether the detected viral DNA represented infectious virus, potentially leading to overestimation of fomite transmission risk. Future investigations with larger sample sizes and systematic viral culture integration are needed to validate these preliminary findings.
Despite these limitations, this outbreak underscores the necessity of proactive surveillance within high-risk sexual and social networks, culturally appropriate risk communication strategies, and the integration of environmental and genomic data into comprehensive outbreak management. Additionally, the observed pre-symptomatic oropharyngeal viral shedding warrants further investigation to refine diagnostic protocols and optimize prevention strategies. Sustained vigilance, rapid detection capabilities, and cross-sectoral collaboration remain essential for preventing future introductions and limiting the spread of MPXV (Clade Ib) in China’s high-mobility urban centers.
-
Approval from the Ethics Committee of Jinhua Center for Disease Control and Prevention, China (approval number: 2025-22).
HTML
Case Report
Laboratory Testing
| Citation: |

|