
 Download:
Download:




-
Introduction: Rabies vaccination compliance and safety are critical for post-exposure prophylaxis. This study compared the freeze-dried human rabies vaccine (Vero cell) under 4-dose (Zagreb) and 5-dose (Essen) regimens in real-world settings.
Methods: In this open-label, randomized trial across Jiangsu Province, China between 2023 and 2024, 2,000 participants received Zagreb (n=999) or Essen (n=1,001) regimens. Active mobile-app surveillance monitored adverse reactions for 28 days post-vaccination. Compliance was assessed through dropout (discontinuation) and out-of-window administration (delayed dosing). Safety and compliance differences were analyzed using the chi-squared or Fisher’s exact tests.
Results: Overall adverse reaction rates were comparable (Zagreb: 2.10%; Essen: 2.70%; P=0.385). Solicited local adverse reactions (pain, induration, swelling, and itching) occurred at rates of 1.50% for Zagreb and 2.10% for Essen. Solicited systemic adverse reactions (fever, diarrhea, and vomiting) were 0.60% for both. Dropout rates were statistically similar (8.51% vs. 8.69%; P=0.884), but Zagreb had significantly fewer out-of-window administrations (8.41% vs. 16.38%; P<0.001). Compliance factors differed: Zagreb was associated with age/marital status/exposure level; Essen additionally involved education and perceived convenience.
Conclusion: Both regimens demonstrated comparable safety profiles. The Zagreb regimen showed significantly superior schedule adherence through reduced out-of-window administrations while maintaining similar dropout rates to the Essen regimen.
-
Rabies remains a serious public health threat, characterized by high fatality rates after clinical onset and a substantial burden on healthcare systems worldwide (1). Vaccination is the most effective prevention method, but compliance varies widely (2). Completing the recommended vaccination schedule is crucial for developing immunity (3). Delayed doses require adjustments to subsequent doses while maintaining proper intervals (4). Currently, China has approved two post-exposure prophylaxis regimens: the Essen 5-dose (1-1-1-1-1) regimen (vaccination on days 0, 3, 7, 14, 28) and the abbreviated Zagreb 4-dose (2–1–1) regimen (vaccination on days 0, 7, 21) (5). Reducing the number of doses decreases the number of clinic visits, which is believed to improve compliance.
This open-label, randomized trial (China Drug Trials: CTR20222797) comprised 2,000 participants with rabies exposure across five Jiangsu counties: Gaogang, Guannan, Huaiyin, Siyang, and Yixing (400 per site). Participants were randomly assigned to the Essen or Zagreb regimens. Both groups received the freeze-dried human rabies vaccine (Vero cell) manufactured by Changchun Institute of Biological Products Co., Ltd. (batch No. 20210911 and 20211016).
Safety monitoring included 30-min onsite observation after each vaccination by trained investigators, who recorded local/systemic reactions via mobile application. Participants or guardians subsequently reported solicited adverse reactions within 7 days, and unsolicited/serious adverse reactions within 28 days post-vaccination. Investigators assessed all reports for causality and severity using National Medical Products Administration criteria (2019 edition), which defined four severity grades ranging from asymptomatic (Grade 1) to life-threatening (Grade 4) (6). Exposure levels were categorized into three distinct classifications: Level I (animal contact or intact skin exposure), II (minor abrasions without bleeding), and III (penetrating wounds or mucosal contamination).
Compliance was evaluated through a questionnaire assessing reasons for non-compliance following vaccination, with non-compliance defined through two distinct metrics: dropout (discontinuation post-randomization) and out-of-window administration (receiving a dose later than the maximum permitted delay). As per protocol, the Zagreb out-of-window thresholds were defined as: ≥1 day (dose 1–2), ≥2 days (dose 3), or ≥3 days (dose 4); the Essen out-of-window thresholds were defined as: ≥1 day (dose 1–2), ≥2 days (dose 3–4), or ≥3 days (dose 5).
Safety comparisons and compliance comparisons between groups were conducted using the chi-squared or Fisher’s exact test. All hypothesis testing was two-sided, with a P-value <0.05 considered statistically significant. All statistical analyses were performed using SAS (version 9.4, SAS Institute Inc., Cary, NC, USA).
A total of 2,000 participants were enrolled in the study between January 17, 2023 and May 21, 2024, with 999 receiving the Zagreb regimen and 1,001 receiving the Essen regimen. None received rabies immunoglobulin (RIG) or anti-rabies virus monoclonal antibody (mAb) as part of their post-exposure prophylaxis. All participants received the first injection and were included in the safety analysis set (SS) for adverse reaction monitoring. Among these, 172 participants (85 Zagreb, 87 Essen) did not complete the full vaccination schedule (Figure 1). No significant demographic differences were observed between groups at enrollment (
Supplementary Table S1 ).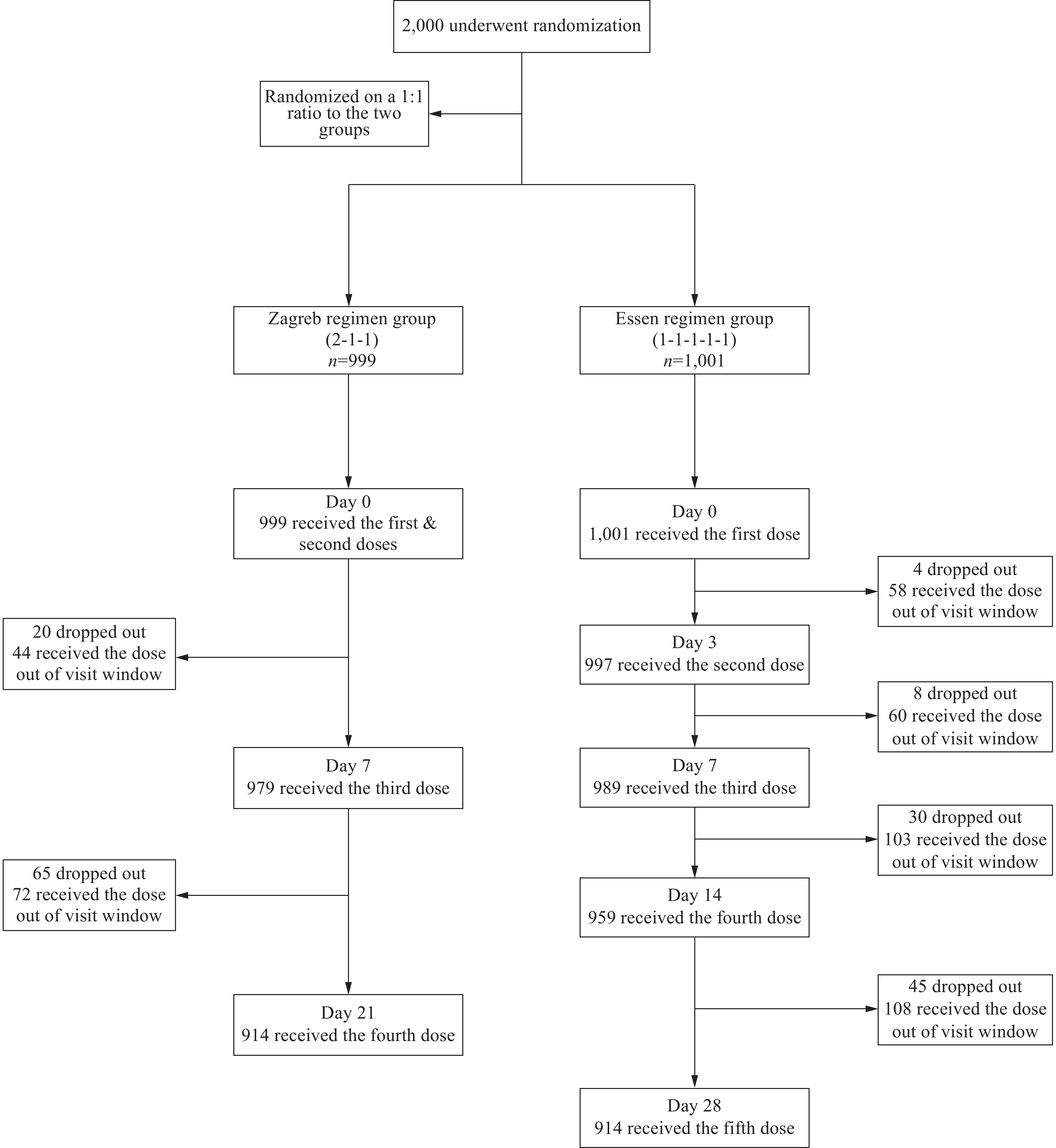 Figure 1.
Figure 1.Inclusion and follow-up in analyses of safety and compliance in two groups.
From the first dose to 28 days after the last dose, the overall incidence of adverse reactions was 2.10% in the Zagreb group and 2.70% in the Essen group, with no significant difference between groups. The most common solicited local adverse reactions in the Zagreb regimen group were pain (1.10%) (grade 1: 1.00%, grade 2: 0.10%), swelling (0.10%) (grade 2: 0.10%), and itching (0.30%) (grade 1: 0.30%). In the Essen regimen group, the most common solicited local adverse reactions were pain (1.80%) (grade 1: 1.30%, grade 2: 0.50%) and induration (0.30%) (grade 1: 0.20%, grade 2: 0.10%). The most common solicited systemic adverse reactions in the Zagreb group were fever (0.60%) (grade 1: 0.10%, grade 2: 0.30%, grade 3: 0.30%), diarrhea (0.10%) (grade 1: 0.10%), and vomiting (0.20%) (grade 1: 0.20%), while in the Essen group, they were fever (0.50%) (grade 1: 0.30%, grade 3: 0.20%) and vomiting (0.10%) (grade 1: 0.10%) (Figure 2). No significant differences in these symptoms were observed between groups. No serious adverse reactions or events were reported in either group.
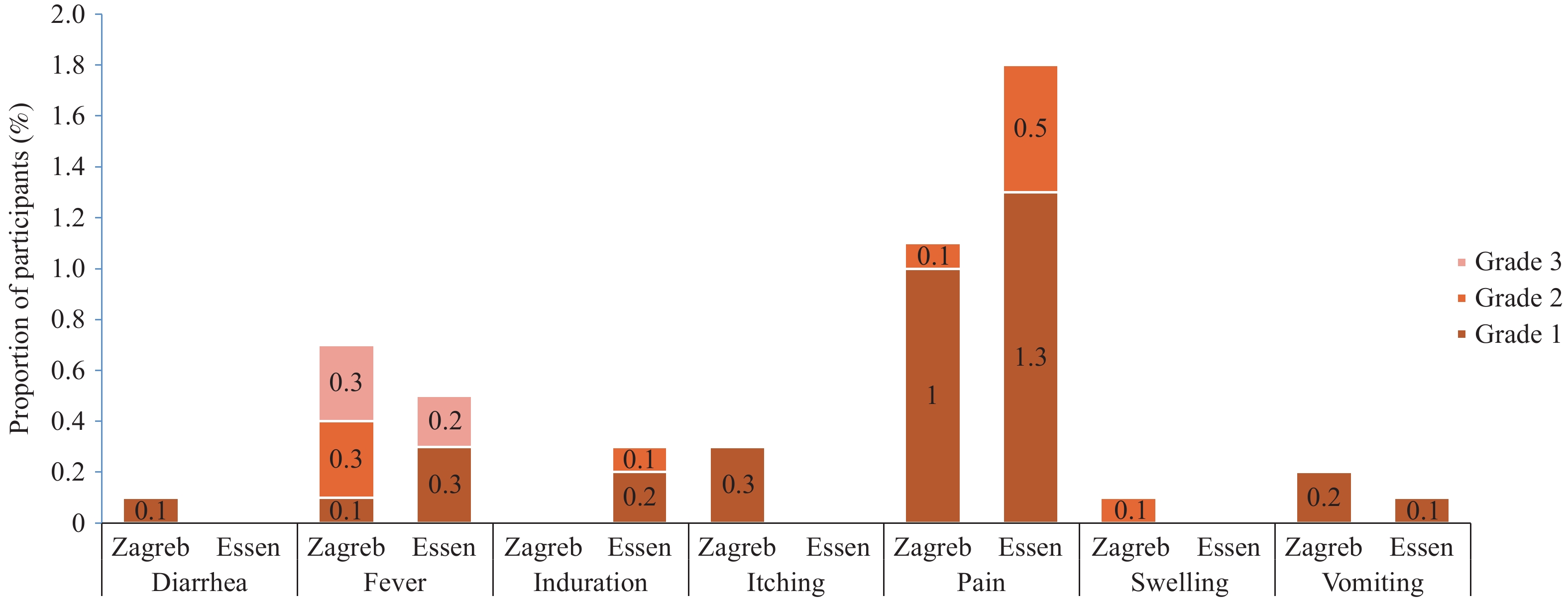 Figure 2.
Figure 2.Solicited local and systemic adverse reactions between two groups.
Among the 2,000 participants, dropout rates for the second dose were 2.00% in the Zagreb regimen group compared to 0.40% in the Essen regimen group. The rates of administering the second dose outside the visit window were 4.40% and 5.79%, respectively. For the third dose, dropout rates were 6.64% in the Zagreb group and 0.80% in the Essen group, with rates of administration outside the visit window at 7.35% and 6.02%, respectively. The overall dropout rates were 8.51% for the Zagreb regimen and 8.69% for the Essen regimen, while rates of out-of-window administration were 8.41% and 16.38%, respectively. The differences in dropout rates for the second and third doses, as well as the rates of completing the vaccination series outside the visit window, were statistically significant between the two groups. However, the differences in rates of administering the second and third doses outside the visit window were not statistically significant (Table 1).
Follow-up Status Zagreb Essen Total P Eligible participants for the first visit 999 1,001 2,000 − Dropout, n (%) 0 (0) 0 (0) 0 (0) − Out of window, n (%) 0 (0) 0 (0) 0 (0) − Eligible participants for the second visit 999 1,001 2,000 − Dropout, n (%) 20 (2.00) 4 (0.40) 24 (1.20) 0.001† Out of window, n (%) 44 (4.40) 58 (5.79) 102 (5.10) 0.158 Eligible participants for the third visit 979 997 1,976 Dropout, n (%) 65 (6.64) 8 (0.80) 73 (3.69) <0.001† Out of window, n (%) 72 (7.35) 60 (6.02) 132 (6.68) 0.234 Eligible participants for the fourth visit 989 989 Dropout, n (%) − 30 (3.03) 30 (3.03) − Out of window, n (%) − 103 (10.41) 103 (10.41) − Eligible participants for the fifth visit 959 959 Dropout, n (%) − 45 (4.69) 45 (4.69) − Out of window, n (%) − 108 (11.26) 108 (11.26) − Dropout total, n (%) 85 (8.51) 87 (8.69) 172 (8.60) 0.884 Out-of-window total, n (%) 84 (8.41) 164 (16.38) 248 (12.40) <0.001† * The non-compliant category includes participants meeting either dropout or out-of-window administration criteria as defined in the Methods.
† Statistically significant (P<0.05).Table 1. Analysis of non-compliance* in two groups.
In the Zagreb group, significant differences emerged between compliant and non-compliant participants based on age (P<0.001), marital status (P=0.001), and exposure level (P<0.001). Compliant participants in the Zagreb regimen had a higher mean age (38.81±21.35 vs. 28.18±17.62 years), higher marriage rate (63.93% vs. 51.19%), and a greater proportion of individuals with level III exposure (46.99% vs. 35.71%) (
Supplementary Table S2 ).In the Essen group, significant differences were observed between compliant and non-compliant participants based on age (P<0.001), marital status (P=0.014), highest education level (P=0.027), exposure level (P=0.005), and perception that the Zagreb regimen is more convenient (P=0.006). The compliant group under the Essen regimen demonstrated a higher mean age (39.54±22.47 vs. 30.51±20.61 years), higher marriage rate (65.23% vs. 53.66%), lower proportion of individuals with higher education (bachelor’s degree: 12.66% vs. 17.68%), and a greater proportion of individuals with level III exposure (47.55% vs. 40.85%) (
Supplementary Table S2 ). -
Both regimens showed comparable safety, consistent with prior clinical trials (7–8). The Zagreb regimen demonstrated significantly lower rates of out-of-window administrations (8.41% vs. 16.38%, P<0.001), indicating better schedule adherence despite similar overall dropout rates.
Previous studies suggest that reduced dosing schedules improve compliance by lowering participant burden (9). Our findings confirm this benefit for schedule adherence, with fewer out-of-window doses in the Zagreb regimen (8.41% vs. 16.38%, P<0.001), but similar dropout rates between regimens (8.51% vs. 8.69%, P=0.884) indicate that factors beyond visit frequency affect completion. While fewer doses ease logistical challenges (10), dropout is influenced by demographics and socioeconomic status (2). Identifying these factors allows tailored interventions to improve adherence. Although abbreviated regimens may boost initial participation, addressing barriers after initiation is essential for full-course completion.
Active mobile surveillance detected fewer adverse reactions than phase III trials (7) but more than some post-marketing studies (8), likely due to methodological differences. Phase III trials typically employ active and structured solicitation of a predefined list of adverse events by investigators at each visit, which may capture more minor and transient reactions. In contrast, our active surveillance relied on participant-initiated reporting via the mobile application after training, potentially leading to underreporting of milder, non-bothersome symptoms.
Several limitations warrant consideration. First, the open-label design may introduce observer and reporting biases, despite using standardized digital symptom lists. Second, operational variability arose from using two vaccine batches (both quality controlled) and non-standardized syringes across sites. Third, recruitment was limited to Jiangsu Province, restricting generalizability. Although all batches met national regulatory quality control standards, the absence of batch-tracking data prevents assessment of batch-to-batch safety variations. Despite these limitations, this study provides robust real-world evidence from prospective, app-based active surveillance of 2,000 participants across five districts. It demonstrates comparable safety between regimens while innovatively quantifying differences in schedule adherence. Participant adherence may have been enhanced by awareness of monitoring, but this approach accurately captured adverse reactions and dose-specific compliance patterns often missed by passive surveillance.
In conclusion, both the Zagreb and Essen regimens demonstrated comparable safety profiles. The Zagreb regimen showed significantly better schedule adherence through lower out-of-window administration rates while maintaining comparable dropout rates to the Essen regimen. Future studies should validate strategies addressing non-compliance drivers identified in this trial, while exploring mobile-based surveillance for broader safety monitoring.
-
Approved by the Ethics Committee of the Jiangsu Provincial Center for Disease Control and Prevention (JSJK2022-A038-02) and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice. Written informed consent was obtained from all participants before enrollment.
HTML
| Citation: |

|