
 Download:
Download:




-
Introduction: In 2025, a patient with leukemia in Haizhu District, Guangdong Province, China, tested positive for dengue virus. The local Center for Disease Control and Prevention immediately initiated an investigation and response.
Methods: This investigation included epidemiological surveys, vector mosquito surveillance, case findings, and blood sample collection for laboratory testing. The laboratory analyses comprised dengue virus nucleic acid detection, antigen detection, specific antibody detection, viral isolation, and genetic sequencing.
Results: The patient was diagnosed with dengue virus serotype 1 (DENV-1) infection 6 months prior to undergoing chemotherapy and targeted therapy for leukemia. Six months later, during high-intensity immunosuppressive therapy following allogeneic hematopoietic stem cell transplantation, the patient tested positive again for DENV-1. Genetic sequencing revealed 99.99% identity between the viral sequences obtained during initial infection and subsequent detection. Viral culture confirmed the presence of a replication-competent live virus.
Conclusions: This is the first documented case of persistent dengue virus infection lasting six months in a patient with leukemia in China. This highlights that for patients undergoing hematopoietic stem cell transplantation and immunosuppressive therapy, particularly in dengue-endemic regions, there should be heightened vigilance regarding the possibility of persistent dengue infection. Implementation of continuous serological monitoring is warranted in high-risk populations.
-
Dengue is primarily endemic to tropical and subtropical regions. The dengue virus (DENV) comprises four serotypes (DENV-1–4) and is predominantly transmitted through mosquito vectors (1). DENV is traditionally considered to cause only acute infection in humans, with efficient clearance by the host immune system post-infection. Reinfection typically occurs only upon exposure to different DENV serotypes. In immunocompetent individuals, dengue fever usually presents as an acute self-limiting disease. The viremic phase lasts approximately 2–7 days; the virus is typically cleared within 2–3 weeks post-infection, conferring lifelong homotypic immunity — mediated by DENV-specific memory T and B cells — which provides rapid protection against reinfection with the same serotype (2). Long-term dengue infections are rare. Herein, we report the first documented case of homologous DENV persistence following allogeneic hematopoietic stem cell transplantation (allo-HSCT), confirmed using whole-genome sequencing (WGS).
-
The patient was a 19-year-old male individual diagnosed with Philadelphia chromosome-positive acute B-lymphoblastic leukemia on August 3, 2024, presenting with fever, arthralgia, and severe thrombocytopenia (platelet count, 15×109/L). He subsequently received intensive chemotherapy combined with targeted therapy (hyper-CVAD regimen A plus orelabrutinib). On October 21, 2024, he developed fever, rash, and calf pain during chemotherapy. On day 5 of febrile illness, laboratory testing revealed positive dengue NS1 antigen with negative immunoglobulin (Ig)M and IgG antibodies and stable platelet counts. Reverse transcription polymerase chain reaction (RT-PCR) confirmed primary DENV-1 infection [cycle threshold (CT), 11.61]. Symptoms resolved within one week of supportive treatment. Chemotherapy was suspended for 2 months owing to persistent thrombocytopenia and reinitiated on January 17, 2025, with high-dose methotrexate, vincristine, prednisone, and orelabrutinib. No further dengue virus tests were performed during this interval.
On March 5, 2025, the patient underwent a myeloablative conditioning regimen consisting of total-body irradiation combined with fludarabine/cyclophosphamide, followed by paternal donor-derived allogeneic hematopoietic stem cell transplantation (allo-HSCT) on March 14, 2025. Neutrophil engraftment (absolute neutrophil count, ≥0.5×109/L) and platelet engraftment (platelets, ≥20×109/L) were achieved on post-transplantation days +11 and +12, respectively. On day +26 (April 9, 2025), a scattered pruritic erythematous rash (nonpainful) appeared on the palms and face, consistent with grade 3 acute cutaneous graft-versus-host disease (GVHD) by the National Institutes of Health (NIH) criteria. By day +30 (April 13, 2025), he developed unexplained diarrhea with abdominal pain progressing to hematochezia. Gastrointestinal endoscopy revealed diffuse mucosal erosion with hemorrhage. Concurrent refractory thrombocytopenia (<20×109/L) persisted despite platelet transfusions. The patient received multiagent immunosuppressive therapy (methylprednisolone, cyclosporine, ruxolitinib) with suboptimal response, indicating therapy-refractory acute gastrointestinal GVHD. Biomarker profiling demonstrated high-risk features: sST2, 412,173 pg/mL; REG3α, 10,416 pg/mL; sTNFR1, 3,108 pg/mL. The final diagnosis was concurrent grade 3 cutaneous and grade 4 gastrointestinal GVHD (NIH grading) complicated by refractory hematochezia and transfusion dependence.
The patient underwent screening for infectious sources owing to persistent diarrhea, hematochezia, and progressive thrombocytopenia with poor response to treatment. Plasma metagenomic next-generation sequencing detected the nucleic acid sequence of DENV-1 on May 20, 2025. Subsequent dynamic monitoring during May 16–29 demonstrated persistent positivity for viral RNA (CT, 19.51–20.56), positive NS1 antigen, positive IgM, and negative IgG. On June 4, 2025, WGS revealed a high degree of homology (>99.99%), with a single nucleotide difference of 10,635 nucleotides) between the DENV-1 sequence in this blood sample and the sequence obtained during the initial infection. Viable DENV was isolated from blood samples using Aedes albopictus C6/36 cell culture, with the isolate serotyped as DENV-1 by quantitative RT-PCR. The complete disease course and dengue testing timeline are shown in Figure 1.
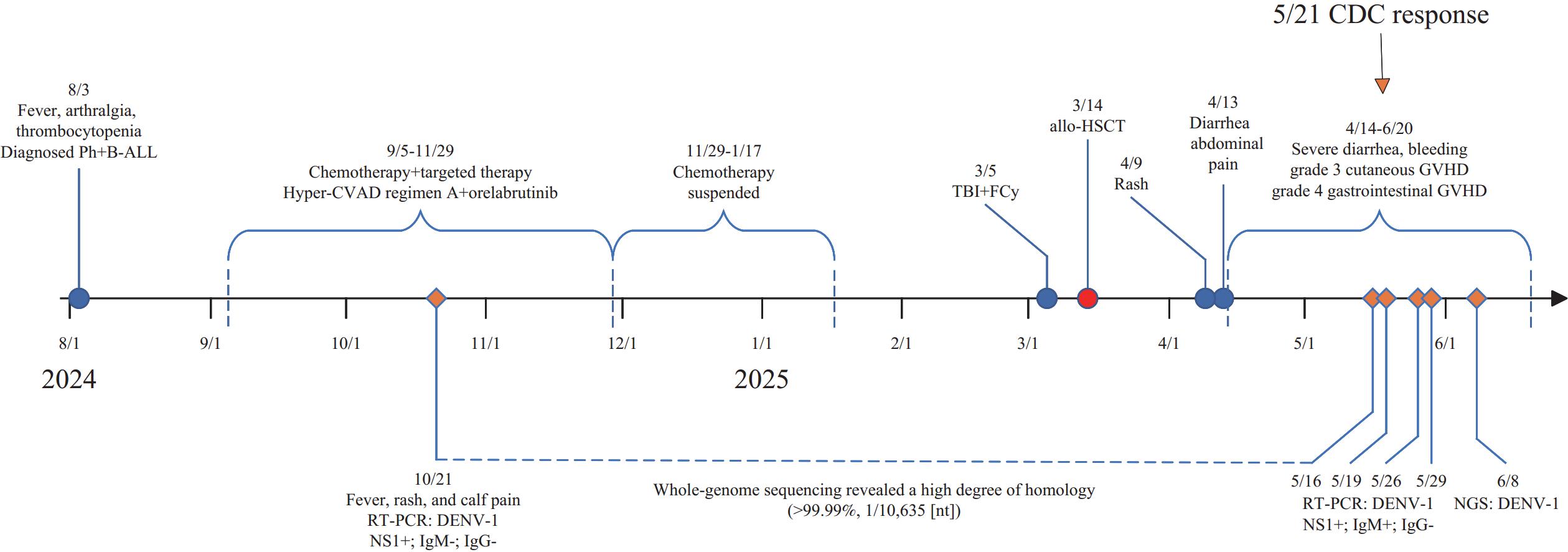 Figure 1.
Figure 1.The complete disease course and dengue testing timeline of the case.
Note: “−” means negative; “+” means positive.
Abbreviation: B-ALL=B-lymphoblastic leukemia; allo-HSCT=allogeneic hematopoietic stem cell transplantation; GVHD=graft-versus-host disease; RT-PCR=reverse transcription polymerase chain reaction; NGS=next-generation sequencing; DENV=dengue virus.
Throughout nearly 1 month of isolation and treatment, the patient was continuously protected using a laminar airflow bed, effectively eliminating potential exposure to mosquito vectors. Surveillance data indicated no reported dengue cases (imported or local) in the patient’s residential area within the 30 days preceding diagnosis. Mosquito surveillance data confirmed that the vector density within the patient's community remained below the safe threshold, meeting the national health authorities' criteria for no transmission risk (3). Furthermore, case-finding activities conducted among nearby residents and hospital facilities identified no suspected cases. The stem cell transplant donor (the patient’s father) had no recent history of dengue infection. Written informed consent was obtained from the patient.
-
DENV is classically considered a non-persistent pathogen in human hosts that typically causes self-limiting acute infections that are effectively cleared by the host immune response (2). The reinfection of individuals is believed to occur only through distinct serotypes. However, we report a rare case of a patient having leukemia with confirmed DENV-1 infection during chemotherapy who subsequently tested persistently positive for DENV-1 RNA 6 months after undergoing allo-HSCT and intensive immunosuppression therapy for graft rejection. This suggests that DENV infection may persist in immunocompromised or immunosuppressed populations with temporary immune impairment due to medical treatment or medication use, rather than repeated exogenous exposure.
Although dengue is primarily transmitted through mosquito vectors, cases of transfusion-related and organ transplantation-associated transmission have been documented (4). In the present case, we excluded cases of reinfection via mosquito vectors, blood transfusion, and bone marrow transplantation. Despite the occurrence of this case in Guangdong Province, China (a dengue-endemic region), the current epidemic pattern is driven primarily by imported cases without evidence of sustained local transmission chains (5). Surveillance data from the local Centers for Disease Control and Prevention indicated a Breteau Index of <5 (suggesting low mosquito density), and no locally acquired cases were reported for 3 consecutive months, thereby ruling out the possibility of community mosquito-borne transmission. Furthermore, the allo-HSCT donor showed no evidence of dengue infection. The likelihood of transmission related to allo-HSCT or blood transfusion is considered extremely low. Comparative genomic analysis of DENV-1 WGS during the initial infection and 6 months later revealed >99.99% sequence identity, confirming the occurrence of autologous persistent infection.
Persistent DENV infection remains exceptionally rare. In immunocompetent hosts, the canonical immunological response involves dengue-specific IgM seroconversion detectable 3–5 days post-infection (lasting 2–3 months), followed by IgG emergence around day 14, which confers lifelong serotype-specific immunity (6). Crucially, while pre-existing humoral immunity generally wanes after allo-HSCT, studies indicate that most patients with hematological malignancies retain high-titer measles/mumps/rubella IgG at 12 months post-transplantation (7). Notably, our patient remained dengue-IgG seronegative 6 months after the initial detection, suggesting failed protective antibody induction — potentially enabling viral persistence. Impaired immune surveillance in leukemia likely compromised both cellular and humoral antiviral clearance mechanisms (8). Collectively, such multifactorial immunosuppression provides the most parsimonious explanation for the observed DENV-1 detection at the 6-month follow-up.
In immunocompetent hosts, DENV infection activates T- and B-cell-mediated adaptive immunity, establishing lifelong serotype-specific immunological memory. Homologous reinfection triggers rapid memory responses (6). Paradoxically, impaired T/B-cell function disrupts viral clearance, memory formation, and immune activation. Literature documents viremia persisting ≤80 days post-HSCT in patients with hematological malignancies (9). Ng et al. reported a 4-month DENV-3 RNAemia (non-cultivable) with concomitant 9-month infectious virus shedding in the urine of a renal transplant recipient (10). Thaivanich et al. detected DENV genomic RNA in granulocyte colony-stimulating factor-mobilized peripheral blood stem cells from an asymptomatic patient with myeloma in remission without recent symptoms or serological evidence (11). In this case, we observed a significant increase in GVHD biomarkers, which may be related to immunosuppression and DENV infection. Immune abnormalities in the patient could not effectively clear the DENV virus, thereby promoting persistent DENV infection.
Collectively, immunosuppressed hosts fail to achieve rapid viral clearance or establish sterilizing immunity, in stark contrast to immunocompetent individuals.
Because sustained virological monitoring was not performed post-initial infection, the exact viral state remains undefined. We recommend longitudinal monitoring of viral RNA, NS1 antigen, and serological profiles in immunocompromised patients (e.g., leukemia) post-dengue infection to elucidate persistence dynamics and clinical implications. Owing to the risk of infection, we recommend close virological follow-up after the acute phase, including weekly quantitative RT-PCR or NS1 testing within 4–6 weeks of symptom onset to track viral clearance, and prolonged monitoring of patients with low platelets, unknown causes, or signs of inflammation.
Clinically, dengue exhibits a significant symptomatic overlap with hematological disorders (12). Despite definitive laboratory evidence of acute dengue infection, the present patient lacked the classic dengue symptoms (fever, myalgia/arthralgia, and hepatic/renal impairment). The rash was attributed to acute GVHD, and diarrhea, hemorrhage, and thrombocytopenia were deemed disease-related. Given that immunocompromised patients may present with atypical manifestations and that active dengue infection can exacerbate underlying conditions, clinicians must include dengue in the differential diagnosis when managing hematological patients with unexplained clinical deterioration and implement comprehensive virological/serological assessments.
In summary, we documented persistent DENV-1 viremia over 6 months during chemotherapy and allogeneic HSCT in a patient with hematological malignancy. This underscores the need for vigilance against persistent dengue in immunosuppressed populations and highlights the critical role of sustained serological surveillance in clinical management.
HTML
| Citation: |

|