
 Download:
Download:




-
Introduction: This study aimed to investigate the associations between training curriculum factors and the intention of laypersons to perform cardiopulmonary resuscitation (CPR).
Methods: We recruited laypersons participating in CPR training programs from nine public training institutes in Beijing, China, between February 15 and July 15, 2025. The exposure variable in this cohort study was trainee feedback on course content, and the primary outcome was a high intention to perform CPR following training. Robust Poisson regression models were used to calculate the incidence rate ratios (RRs) with 95% confidence intervals (CIs).
Results: Among 2,035 laypersons enrolled, 74.7% reported high CPR intention following training. This proportion was 42.4% and 96.4% for those with low and high CPR intentions, respectively, before training. Nine curriculum factors with RRs greater than 1.000 were identified. In 817 low-intention laypersons, the coexistence of five to seven factors and eight or nine factors increased the likelihood of high intention by 174.7% (RR=2.747; 95% CI: 0.964–7.826) and 283.6% (RR=3.836; 95% CI: 1.493–9.857), respectively, compared with exposure to zero to four factors. In 1,218 high-intention laypersons, a dose-response relationship emerged indirectly, as curriculum factors enhanced CPR intention by improving self-efficacy in cardiac arrest recognition and CPR performance.
Conclusions: Our study highlighted that key CPR curriculum content is associated with the post-training intention to perform CPR in the real world.
-
Bystander-initiated cardiopulmonary resuscitation (CPR) is the most effective intervention for out-of-hospital cardiac arrest (OHCA). However, only 4.8% of patients in China receive it, contributing to over one million massive sudden deaths annually (1-2). The American Heart Association (AHA) Utstein Formula for Survival states that public training is essential for translating scientific advancements into community-based lifesaving action (3). Standardized CPR courses provided by the Red Cross Society (RCS) and AHA are available to the public, and the average proportion of residents with first-aid certification in high-income countries is estimated at 10.2% (4). Within these frameworks, the effective transfer of knowledge and skills from the instructor to the trainee is regarded as a central driver in enhancing a layperson’s intention to initiate CPR, as conceptualized in the AHA’s intention-focused model (5–6).
However, no empirical studies have examined the relationship between the curriculum components of CPR training and laypersons’ post-training intentions to perform CPR. This study aimed to explore the relationship between CPR curriculum factors and laypersons’ intentions to perform CPR following real-world public training.
Between February 15 and July 15, 2025, we administered structured questionnaires to laypersons before and after the basic life support (BLS) training. The participating institutions included one emergency medicine center, two hospitals, and six social organizations that either voluntarily responded to the outreach efforts of the Chinese Center for Disease Control and Prevention (China CDC) or were recommended by the Beijing branch of the RCS. Participation in the survey was voluntary, and informed consent was obtained from each trainee prior to course initiation. The design of the questionnaire incorporated core content areas derived from standardized CPR curricula established by authoritative bodies, such as the RCS and AHA. To evaluate intention, respondents were asked to rate their willingness to perform CPR on a visual analog scale ranging from 0 (“not willing at all”) to 10 (“definitely willing”). To assess self-efficacy, participants responded to the statements “I can identify OHCA correctly” and “I can perform CPR correctly” using a five-point Likert scale (strongly disagree, disagree, neutral, agree, and strongly agree). The exposure variable was defined based on participant feedback regarding specific elements of course content, such as “Instructors mentioned the Civil Code of the People’s Republic of China” and “Instructors stated that chest–compression–only CPR is comparable to standard CPR that includes artificial respiration.” The primary outcome was defined as a high intention to perform CPR following training, operationalized as a self-reported score of 9 or higher on a 10-point visual analog scale. Secondary outcomes included post-training self-reported strong agreement with the statements “I can identify OHCA correctly” and “I can perform CPR correctly,” reflecting high self-efficacy in these domains.
The incidence rates of high intentions to perform CPR after BLS training were also calculated. To estimate the associations between curriculum factors and study outcomes, we employed robust Poisson regression models to calculate rate ratios (RRs) with 95% confidence intervals (CIs), adjusting for sex, age, public servant status, education level, previous CPR training experience, possession of a first-aid certificate, prior witnessing of an emergency, and high CPR intention before class. To account for the clustering effects associated with training institutions and instructors, the training class was modeled as a repeated-measures factor. The subgroup analysis were conducted based on the adjusted variables. All analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA). Statistical significance was defined as a two-sided P value of <0.05, except for tests of linear trends using the Chi-square method, in which a one-sided P value was applied.
A total of 2,035 participants from 148 training classes were analyzed. The sample comprised of a higher proportion of men, younger individuals, and those with college degrees or higher. The incidence of high CPR intention after training was 74.7%, whereas the rates were 42.4% and 96.4% for those with low and high intentions before training, respectively (Table 1). As shown in Table 2, the prevalence of the nine evaluated curriculum factors, each associated with an RR greater than 1.000, ranged from 79.7% to 96.4%. However, the proportion of participants exposed to all nine curriculum factors was only 57.7% (52.5% and 61.3% of those with low and high intentions, respectively), indicating a notable drop in comprehensive curriculum coverage. Each individual factor was associated with an increase in the incidence of reporting a high intention to perform CPR after training, which ranged from 6.3% to 15.0%. Compared with participants exposed to zero to four curriculum factors, those exposed to five to seven and eight to nine factors demonstrated a 15.6% increase (RR=1.156; 95% CI: 0.997–1.341) and 35.1% increase (RR=1.351; 95% CI: 1.174–1.555) in high intention rates, respectively, exhibiting a clear dose-response relationship (P for trend <0.001). This finding was consistent across the subgroups, except for CPR intention before training.
Population characteristics n (%) High intention to perform CPR (%) P Sex Male 1,117 (54.9) 74.8 0.863 Female 918 (45.1) 74.5 Age (years) 15–29 731 (35.9) 70.5 <0.001* 30–39 680 (33.4) 74.6 40–49 435 (21.4) 79.1 50–69 189 (9.3) 81.5 Public servant status Yes 377 (18.5) 78.0 0.878 No 1,658 (81.5) 73.9 Education level High school or less 96 (7.8) 76.0 <0.001* College 791 (64.0) 75.0 Graduate 349 (28.2) 65.3 Enthusiastic philanthropist Yes 645 (31.7) 78.6 0.006 No 1,390 (68.3) 72.9 Ever participated in CPR training Yes 745 (36.6) 75.7 0.425 No 1,290 (63.4) 74.1 Ever witnessed CPR performed by others Yes 482 (23.7) 82.0 <0.001 No 1,553 (76.3) 72.4 Intention to perform CPR before class Low 817 (40.2) 42.4 <0.001 High 1,218 (59.8) 96.4 Total 2,035 (100.0) 74.7 Abbreviation: CPR=cardiopulmonary resuscitation.
* P for trend.Table 1. Incidence of high intention to perform CPR after training by population characteristics.
Curriculum factors Person number
n (%)High intention to perform CPR following training (%) RRs
(95% CIs)Yes No Single curriculum factor Instructors mentioned the Civil Code of the People’s Republic of China 1,779 (87.4) 75.6 68.8 1.074 (1.013, 1.139) Instructors mentioned agonal breathing 1,951 (95.9) 75.1 64.3 1.084 (0.948, 1.239) Instructors mentioned telecommunicator CPR 1,932 (94.9) 75.2 65.1 1.063 (0.940, 1.201) Instructors stated that any CPR is better
than no CPR1,938 (95.2) 75.4 60.8 1.150 (1.031, 1.282) Instructors emphasized immediate CPR when cardiac arrest is uncertain 1,680 (82.6) 76.9 64.5 1.116 (1.046, 1.190) Instructors stated that chest-compression-only CPR is comparable to standard CPR that includes artificial respiration 1,639 (80.5) 77.3 63.9 1.140 (1.082, 1.202) Instructors preset an emergency scenario 1,622 (79.7) 77.9 62.2 1.143 (1.073, 1.218) Trainees practiced chest compressions
at least once1,962 (96.4) 75.0 65.8 1.137 (1.028, 1.258) Trainees practiced use of an automated external defibrillator at least once 1,906 (93.7) 75.2 66.7 1.075 (0.966, 1.196) Number of curriculum factors coexisting 0–4 73 52.1 – 1.000 5–7 415 66.5 – 1.156 (0.997, 1.341) 8–9 1,547 78.0 – 1.351 (1.174, 1.555) P for trend – <0.001 – – Note: Adjusted for sex, age, public servant status, education level, previous CPR training, possession of a first-aid certificate, prior witnessing of an emergency, high intention before training, and training class, if applicable;
–: not applicable.
Abbreviation: CPR=cardiopulmonary resuscitation; CI=confidence interval; RR=rate ratio.Table 2. Association between curriculum factors and high intention to perform CPR following training.
For all participants, in addition to the direct relationship above, curriculum exposure was also associated with enhanced self-efficacy, particularly, the ability to recognize OHCA and correctly perform CPR, which further mediated CPR intention. For the 817 participants with a low CPR intention before training, relative to the presence of zero to four factors, the coexistence of five to seven factors and eight or nine factors was associated with 174.7% (RR=2.747; 95% CI: 0.964–7.826) and 283.6% (RR=3.836; 95% CI: 1.493–9.857) increase in high intention incidence, respectively. Participants exposed to five to seven and eight to nine factors were 137.8% (RR=2.378; 95% CI: 1.280–4.418) and 250.1% (RR=3.501; 95% CI: 1.868–6.558) more likely, respectively, to strongly agree with the statement “I can correctly perform CPR,” than those exposed to zero to four factors. This showed a significant dose-response trend (P for trend <0.001). Furthermore, participants who agreed or strongly agreed with this statement were 73.0% (RR=1.730; 95% CI: 0.885–3.396) and 233.2% (RR=3.332; 95% CI: 1.674–6.632) more likely to report high CPR intention post-training, respectively (P for trend <0.001), than those responding “neutral” or lower. A similar pattern of association was observed for the intermediate variable “I can correctly identify cardiac arrest.” For 1,218 with a high CPR intention before training, a similar dose-response pattern was also found in the indirect pathway, although the RRs were obviously small. Detailed information is shown in Figure 1.
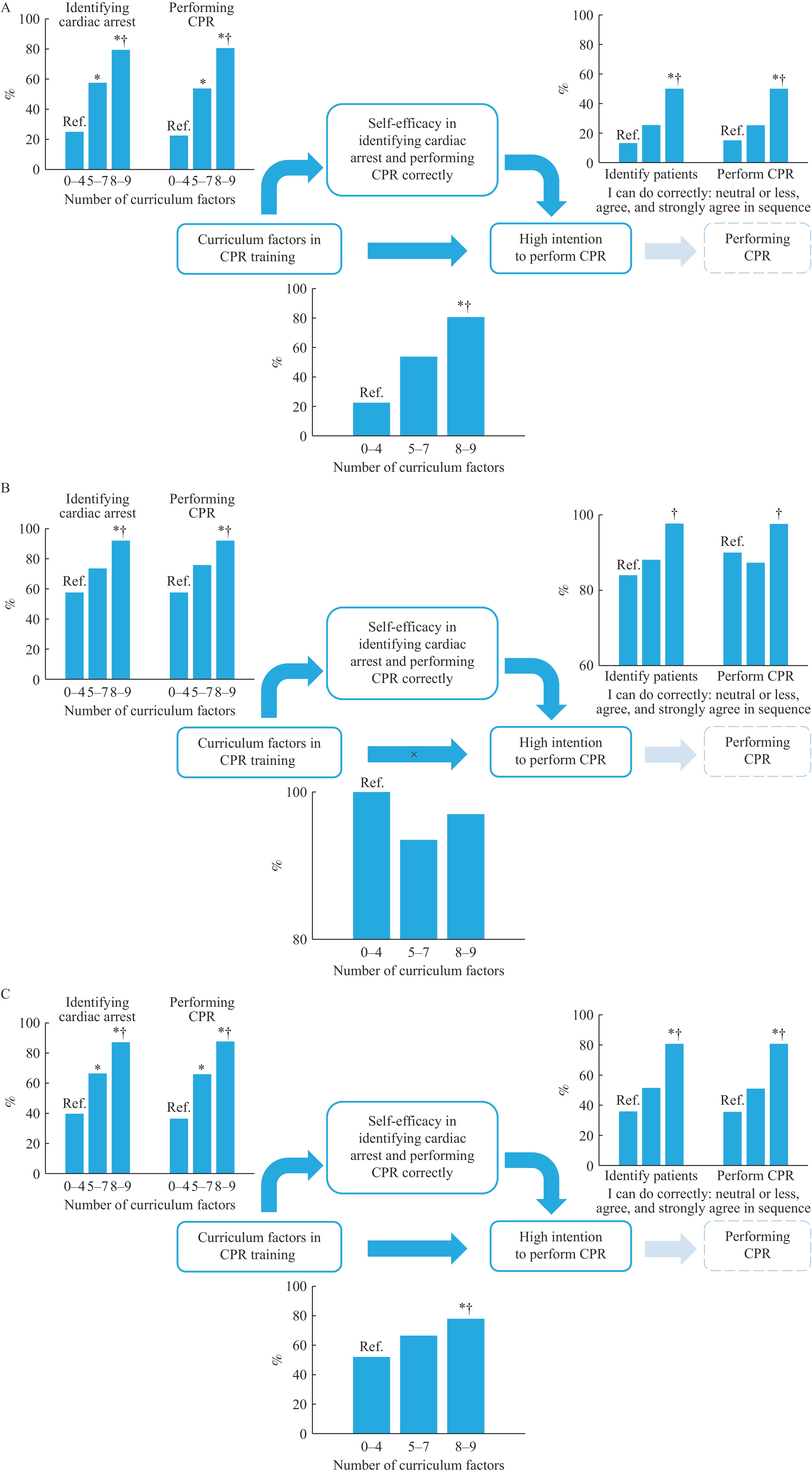 Figure 1.
Figure 1.Dose-response relationships in the direct and indirect pathways linking curriculum factors in CPR training scenarios with laypersons’ intention to perform CPR. (A) 814 participants with low CPR intention before training. (B) 1,218 participants with high CPR intention before training. (C) A total of 2,035 participants.
Note: Self-efficacy was assessed using the statements “I can correctly identify cardiac arrest” and “I can correctly perform CPR for patients with cardiac arrest.” A strong agreement with either statement was considered indicative of high self-efficacy. In the left of Figure 1A, 1B, and 1C, “%” represents percent of participants post-training self-reporting strong agreement with the statements “I can identify OHCA correctly” and “I can perform CPR correctly.” In the right and below of Figure 1A, 1B, and 1C, “%” represents percent of participants post-training self-reporting a high intention to perform CPR.
* P <0.05, compared with the reference.
† P for trend <0.001.
Abbreviation: CPR=cardiopulmonary resuscitation; OHCA=out-of-hospital cardiac arrest.
-
To our knowledge, this is the first study to systematically examine how specific CPR curriculum components influence laypersons’ intention to perform CPR following real-world public training. This study demonstrated a clear association between key curriculum factors within CPR training programs and the post-training intention to perform CPR, although the overall translation of training into high post-course intention remains suboptimal in China.
These curriculum components either promote intention directly or increase self-efficacy in recognizing OHCA and correctly executing CPR, both of which serve as mediators of intention. This dual-pathway effect reinforces the theoretical foundations including the AHA a “Utstein formula for survival” and intention-focused model (3,5). Particular emphasis should be placed on the different association patterns between participants with low and high CPR intentions before training; the former revealed both pathways, whereas the latter being an indirect pathway. However, no single factor was universally effective for all participants. Even among the trainees exposed to all nine identified elements, a considerable proportion failed to report high intention following training.
Persistent barriers to bystander CPR in China, including unwillingness, lack of daring, and inability to save, continue to hinder timely emergency intervention (7). A critical limitation of current public training is the insufficient number of trainees reporting a strong intention to perform CPR following course completion. While structured training is a powerful and complementary strategy for addressing these barriers, current training primarily focuses on the “inability to save” issues related to CPR knowledge and skills, while neglecting the foremost “unwillingness to save.” We have previously proposed specialized national CPR legislation as one solution for “unwillingness to save” (8). This study further contributes by defining concrete educational objectives and offering a structured approach for improving training effectiveness at the population level.
The Healthy China goal for 2022 of certifying more than 1% of residents in first-aid training has been achieved, with 15.26 million people obtaining certificates after BLS training since 2019 (9–10). CPR is a mandatory course for this certification, and has a target to exceed 3% by 2030 (9). Health promotion policies were introduced to achieve this goal. For example, Chinese Citizens’ Health Literacy — Basic Knowledge and Skills (2024 Edition) states that when encountering patients with OHCA, citizens should be able to perform CPR and use automated external defibrillators (11). Furthermore, the World First Aid Day publicity campaign was included in the 2025 annual work point of the Healthy China Action Plan — Program for Cardiovascular and Cerebrovascular Disease Prevention and Treatment Campaign. There is a significant gap between China and advanced countries in the prevalence of CPR training and bystander CPR, which reflects the quantity and quality of public training. Our previous study indicated that CPR promotion measures involve numerous industries, departments, and institutions (12); therefore, we suggest incorporating CPR education and training into the national education system of China through legislation, especially basic education and vocational training.
This study had at least two limitations. Our study is not community-based but possesses good institutional representativeness, covering all types of public CPR training institutions, including BLS courses delivered by the RCS, the AHA, and medical institutions. Additionally, this study is short-term, although it has a prospective component. We did not conduct follow-up assessments to capture actual bystander CPR behavior as per the potential bystander monitoring theory proposed by China CDC (13).
-
The association between curriculum content and post-training intention to perform CPR has been well established in the real world. Identifying and improving curriculum factors associated with CPR intention are recommended to increase the prevalence of layperson interventions in China.
-
All participants contributed to the study. We thank Phoebe Chi, MD, from Liwen Bianji (Edanz) (www.liwenbianji.cn) for editing the manuscript.
-
Ethical approval was obtained from the Ethics Committee of the National Center for Chronic and Noncommunicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention (Approval No. 202428).
HTML
| Citation: |

|