
 Download:
Download:




-
Introduction: On April 1, 2024, a severe thunderstorm occurred in Chongqing, followed by a surge in patients with suspected asthma presenting to the Emergency Department of the First Affiliated Hospital of Chongqing Medical University. A retrospective investigation was conducted to identify the causes and risk factors of this incident, aiming to guide the prevention and control of similar events.
Methods: A questionnaire was designed for telephone follow-up to collect basic information, disease onset characteristics, and residential environment data from patients and their cohabitants. Descriptive analysis and a retrospective case-control study were employed to analyze epidemiological features and risk factors. Meteorological data and environmental indices were concurrently collected.
Results: Ninety suspected thunderstorm asthma (TA) cases were identified, with disease onset predominantly clustered between 21:00 on April 1, 2024 and 03:00 on April 2, 2024. The epidemic curve suggested a point-source exposure or short-term continuous exposure pattern. Among 57 clinically diagnosed TA cases and 111 controls, multivariate analysis revealed allergic rhinitis as an independent risk factor for thunderstorm asthma [odds ratio (OR)=13.129, 95% confidence interval (CI): 2.782, 61.960].
Conclusion: Based on epidemiological investigation, environmental assessment, and laboratory testing results, this incident was classified as a thunderstorm asthma event, with allergic rhinitis identified as an independent risk factor.
-
Thunderstorm asthma (TA) is defined as the sudden onset of asthma symptoms in many individuals due to a rare interaction between specific types of thunderstorms and high levels of airborne allergens. It can lead to a dramatic surge in emergency department visits within a short period and pose a significant strain on medical resources (1-2). This phenomenon primarily occurs in countries such as Australia and the United Kingdom. To date, three incidents have been reported in China (3). We report the first documented TA event in Chongqing. Through a case-control study, we aimed to identify risk factors associated with this condition. Multivariate analysis revealed that allergic rhinitis was an independent risk factor among susceptible individuals.
-
From 21:00 on April 1, 2024 to 00:00 on April 2, 2024, heavy rainfall and thunderstorms affected a wide area of Chongqing. During this period, the First Affiliated Hospital of Chongqing Medical University observed a sharp increase in patients with respiratory symptoms visiting the emergency department. This was reported to the Yuzhong District CDC as a potential group health anomaly. Following an on-site epidemiological investigation, the event was classified as a suspected thunderstorm asthma event by the Yuzhong District CDC and the First Affiliated Hospital of Chongqing Medical University. A retrospective case-control study was conducted to identify potential risk factors.
The study focused on patients who visited the Emergency Department and Respiratory Medicine Department of the First Affiliated Hospital of Chongqing Medical University between 21:00 on April 1 and 00:00 on April 2. Case definitions were established based on the Guidelines for the Prevention and Control of Bronchial Asthma (2020 Edition) (4) and the on-site investigation findings. Suspected cases were defined as individuals experiencing symptoms such as cough, wheezes, dyspnea, shortness of breath, or chest tightness during or after the thunderstorm within 24 hours. Clinically diagnosed cases were those confirmed to have bronchial asthma during or after the thunderstorm, excluding other conditions such as tuberculosis, airway foreign bodies, bronchopulmonary dysplasia, and congenital heart disease.
The Emergency Medicine Department and Respiratory Medicine Department of the First Affiliated Hospital of Chongqing Medical University recorded 16, 27, 124, 26, and 18 patients with respiratory symptoms from March 31 to April 4, respectively. A dramatic surge in patient visits was observed on April 2, with the number of cases increasing five-fold compared to the previous two days. A similar trend was noted across other medical institutions in the city. To further investigate, we collected data on outpatient and emergency department visits from medical institutions in the central city between March 31 and April 2, 2024, using the Social Yuyue Epidemic Prevention and Control application platform. The analysis revealed a significant increase in patients reporting symptoms such as cough, dyspnea, or asthma on April 2, with the majority of cases occurring between 00:00 and 03:00 (
Supplementary Figure S1 ).A total of 90 suspected TA cases were identified, with clinical manifestations including cough, dyspnea, and wheezes (
Supplementary Table S1 ). The onset of symptoms was concentrated between 21:00 on April 1, 2024 and 03:00 on April 2, 2024, accounting for 73 cases (81.1%). The prevalence curve displayed a single peak, indicating a point-source exposure or short-term persistent exposure. The distribution of onset times in the 90 patients is shown in Figure 1. Most patients experienced mild symptoms, except for an 81-year-old woman with a history of hypertension, coronary artery disease, chronic obstructive pulmonary disease, and a tumor. She was admitted to the intensive care unit (ICU) due to severe symptoms. Nine patients received symptomatic treatment and observation in the emergency department for 24 hours, after which they recovered and were discharged.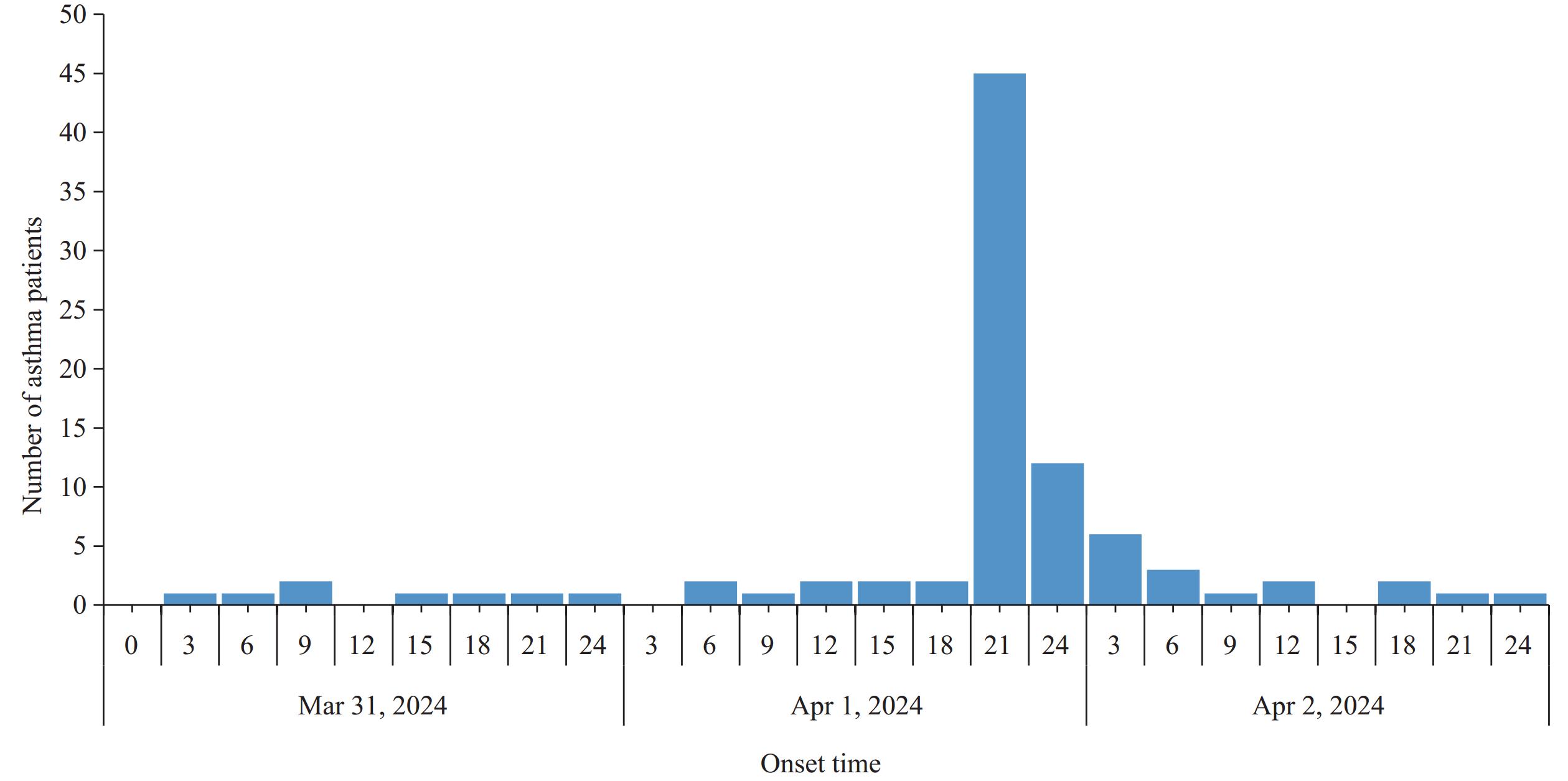 Figure 1.
Figure 1.Distribution of onset time in patients with suspected thunderstorm asthma (n=90).
Among the 90 suspected cases, 60 (66.7%) were female and 30 (33.3%) were male, with a mean age of 41.2±12.3 years. Occupational distribution showed the top three occupations were cadres/employees, commercial services, and domestic/non-domestic work. The cases were distributed across 13 districts and counties (
Supplementary Table S2 ), with the highest concentrations in Jiulongpo District (31 cases, 38.3%), Yuzhong District (19 cases, 23.5%), and Nan’an District (14 cases, 17.3%).Of the 90 patients, 23 underwent routine blood tests. Among these, 18 showed elevated eosinophil levels, and 2 had increased leukocyte and neutrophil counts. Additionally, throat swabs were collected from 9 patients for respiratory multi-pathogen nucleic acid testing. The tested pathogens included influenza A and B viruses, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), adenoviruses, respiratory syncytial viruses, parainfluenza viruses (types I, II, III, and IV), rhinoviruses, human metapneumoviruses, Boca viruses, enteroviruses, coronaviruses (NL63, OC43, 229E, HKU1), Legionella pneumophila, Haemophilus influenzae, Bordetella pertussis, Klebsiella pneumoniae, Chlamydia pneumoniae, and Mycoplasma pneumoniae. Only one patient tested positive for nucleic acids of Haemophilus influenzae and Klebsiella pneumoniae.
A thunderstorm occurred on April 1, starting at 21:00 and lasting until 24:00. It was accompanied by short-term heavy rainfall, with wind speeds reaching levels 2–3 between 21:00 and 23:00. Detailed weather conditions are summarized in
Supplementary Table S3 . During April 1–2, Chongqing Municipality experienced excellent air quality. However, according to China Weather, the daily average pollen concentration in the region was 251–400 grains per thousand square millimeters from March 31 to April 1, reaching a Level 3 warning. This indicates a high likelihood of triggering allergic rhinitis.A total of 57 cases out of the 90 suspected TA patients were clinically diagnosed. Among these, allergen testing was conducted for 13 patients, revealing that 8 had pollen allergies. Additionally, only 16 cases stayed indoors with windows closed during the thunderstorm. These 57 cases were included in a case-control study as the TA group, while 111 non-thunderstorm asthma cases (33 patients who were excluded from the 90 suspected TA patients visiting the Emergency Department of the First Affiliated Hospital of Chongqing Medical University during the thunderstorm and 78 healthy individuals living with the 90 suspected TA patients) were included as the control group. The measurement data between the two groups were analyzed using t-test, while the count data were analyzed using chi-square test. The TA group had more females, patients with a history of allergies, and allergic rhinitis compared to the control group (P<0.05) (Table 1). Factors with P<0.1 in the univariate analysis were further included in a logistic multivariate analysis. This analysis identified a history of allergic rhinitis as an independent risk factor [odds ratio (OR)=13.129, 95% confidence interval (CI): 2.782, 61.960].
Risk factors TA group (n=57) Control group (n=111) P OR 95% CI Age (years) 40.68±12.34 42.69±14.29 0.368 Sex Female 40 49 0.002* 0.336 (0.170, 0.663) Male 17 62 Underlying disease Yes 9 23 0.536 0.717 (0.308, 1.674) No 48 88 History of asthma Yes 5 13 0.793 1.380 (0.466, 4.082) No 52 98 History of allergic diseases Yes 51 51 <0.001* 10.000 (3.967, 25.209) No 6 60 Allergic rhinitis Yes 49 31 <0.001* 15.806 (6.724, 37.156) No 8 80 Stayed indoors with windows closed during the thunderstorm Yes 16 48 0.066* 0.512 (0.257, 1.020) No 41 63 Lived on higher floors (9th floor and above) Yes 30 54 0.745 0.853 (0.450, 1.616) No 27 57 History of respiratory infection in the week before the thunderstorm Yes 20 23 0.061* 2.068 (1.015, 4.214) No 37 88 Active respiratory infection during the thunderstorm Yes 20 20 0.021* 2.459 (1.187, 5.094) No 37 91 * Variables included in Binomial Logistic Regression Analysis (P<0.1).
Abbreviation: TA=thunderstorm asthma; OR=odds ratio; CI=confidence interval.Table 1. Risk factors analysis for TA in the case-control study.
Risk factors β P OR 95% CI Sex −0.618 0.146 0.558 0.245, 1.274 History of allergic diseases 0.138 0.875 0.997 0.181, 5.491 Allergic rhinitis 2.562 0.001* 13.129 2.782, 61.960 Stay indoors with windows closed during the thunderstorm −0.669 0.124 0.529 0.228, 1.227 History of respiratory infection in the week before the thunderstorm 0.252 0.723 1.202 0.316, 4.571 Active respiratory infection during the thunderstorm 0.393 0.585 1.431 0.369, 5.552 * The independent risk factor for TA (P<0.05).
Abbreviation: TA=thunderstorm asthma; β=slopes; OR=odds ratio; CI=confidence interval.Table 2. Binomial logistic regression analysis of risk factors for TA in the case-control study.
-
The first documented TA event was reported in 1983 in Birmingham, UK (5). Over the past 40 years, 32 thunderstorm asthma events have been recorded globally, with the majority occurring in Australia and the UK. The most severe incident to date occurred in Melbourne, Australia, in 2016. Following a thunderstorm, thousands of individuals experienced asthma symptoms, leading to a six-fold increase in emergency department visits for respiratory symptoms within 12 hours compared to the same period in the previous year. Additionally, asthma-related hospitalizations surged nearly 10-fold, resulting in 10 fatalities and drawing global attention (6).
In China, 3 TA events have been reported thus far, occurring in Shaanxi Province (Yulin City), Ningxia Hui Autonomous Region, and Inner Mongolia Autonomous Region (Hohhot City) (7–9). This paper presents the first documented case of a TA event in southwest China. Interestingly, while most previously reported TA events have occurred in plains or flat regions, Chongqing Municipality, where this event took place, is characterized by predominantly mountainous and hilly terrain. This rare occurrence highlights the need for increased attention to the prevention and control of TA, even in mountainous areas.
The pathogenesis of TA remains unclear. However, the widely accepted hypothesis suggests it results from a combination of specific meteorological conditions, high concentrations of airborne allergens, formation of inhalable sensitizing particles (<10 μm in diameter), and exposure of susceptible individuals (1,8). The primary aerial allergens involved are pollen and fungal spores. While allergic rhinitis is closely associated with whole pollen particles, these particles are typically too large to penetrate the lower airways. During thunderstorms, cold air currents can transport pollen or mold particles into clouds, where moisture and lightning cause pollen grains to rupture, releasing smaller allergenic particles. These particles can then be inhaled by susceptible individuals, potentially triggering bronchial asthma (6,10). A relevant example occurred in Chongqing on the night of April 1, 2024, when a thunderstorm coincided with high pollen concentrations in the air, providing the necessary environmental conditions for TA.
TA arises from the interactions between susceptible individuals and environmental factors. In this study, 18 out of 23 patients showed elevated eosinophil levels, suggesting that thunderstorm asthma may be an allergic reaction. Although previous studies indicate that 60%–90% of TA patients have pollen allergies or suffer from allergic rhinitis (11-12), which is consistent with our findings, few studies have explored the risk factors associated with TA in susceptible populations. In our risk factor analysis, univariate analysis revealed that a history of allergies, allergic rhinitis, and current respiratory tract infections was significantly more prevalent in TA patients compared to the control group. However, multivariate analysis identified only a history of allergic rhinitis as an independent risk factor. Additionally, univariate analysis showed a higher proportion of females among TA patients, which may be attributed to the higher prevalence of allergic rhinitis in females. Therefore, individuals with allergic rhinitis represent a key population for TA prevention and control efforts.
This incident exemplifies a typical TA event. Although only one severe case was reported, the sudden surge in asthma patients within a short period placed significant strain on emergency medical resources. Healthcare organizations should develop robust contingency plans to manage similar incidents effectively. Concurrently, public health agencies should improve early warning systems for thunderstorm asthma events (TAEs) and enhance public education to improve awareness and understanding of TA, promoting scientific prevention and control measures. To develop effective early warning systems for TAEs, further studies are needed to investigate the specific meteorological conditions that lead to these events.
This study has two limitations. First, the data were sourced from a single hospital. Second, the retrospective design of the risk factor analysis, coupled with potential recall bias during telephone follow-ups, may affect the reliability of the findings.
-
We thank the staff of the Communicable Disease Prevention and Control Institute of Chongqing CDC, Yuzhong District CDC, and the Emergency Department of the First Affiliated Hospital of Chongqing Medical University for their support and assistance during the investigation.
-
This study was approved by the Research Ethics Board of the Chongqing CDC (approval number: KY-2024-036-2).
HTML
| Citation: |

|