
 Download:
Download:




-
Benzene, classified as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC), can induce benzene poisoning characterized by reduced blood cell counts and lead to hematopoietic malignancies following prolonged occupational exposure (1). In 2002, China reduced the occupational exposure limit for benzene from 40 mg/m3 (Maximum Allowable Concentration, MAC) to 6 mg/m3 (Permissible Concentration-Time Weighted Average, PC-TWA). Consequently, OCBP incidence decreased from 1.69‰ in 1979–1981 to 0.54‰ in 2017 (2). Previous studies have reported that improvements in workplace hygiene conditions and reduced occupational benzene exposure limits have gradually decreased the number of OCBP cases in China from an average of 892 cases per year during 1979–1982 to an average of 256 cases per year during 2005–2019. Correspondingly, the primary industries in which OCBP occurs shifted from coal and coal tar distillation, which involves direct contact with pure benzene, to the general/special-purpose equipment manufacturing industry, which uses benzene-containing raw materials (3). As a major global producer and consumer of benzene, China faces significant occupational health challenges, with over one million workers annually exposed to benzene. Since 2005, OCBP and benzene-induced leukemia have been the most prevalent occupational hazards among COP and occupational tumor cases in China (3). In 2022, China’s occupational exposure limits (OELs) for benzene were further reduced to 3 mg/m3. Nevertheless, despite intensified national regulatory oversight and restrictions on benzene-containing raw materials, uncertainties remain regarding current OCBP distribution patterns.
Based on high benzene production and usage, a relatively developed manufacturing industry, and a large population exposed to benzene, we selected six representative PLADs from the Occupational Disease and Health Monitoring Information System and conducted a descriptive analysis of their reported OCBP cases. The analysis revealed that the industries primarily associated with OCBP have shifted from the general/special-purpose equipment manufacturing industry to the chemical raw materials and chemical products manufacturing industry, followed by the petroleum, coal, and other fuel processing industry. This study underscores the necessity of sustained surveillance of evolving industry patterns in OCBP occurrence to implement targeted regulatory interventions.
-
Six PLADs with substantial benzene production and usage — Jiangsu, Zhejiang, Shandong, Sichuan, Fujian, and Tianjin — were selected for analysis. These PLADs all feature highly developed manufacturing industries. All OCBP patients were diagnosed by local occupational disease diagnosis teams according to the “Diagnostic Criteria for Occupational Chronic Benzene Poisoning” (GBZ 68-2002, GBZ 68-2013, and GBZ 68-2022) of the National Occupational Health Standards of the People’s Republic of China. This study retrieved OCBP data from 2020 to 2023 from the occupational disease reporting systems of the six PLADs and standardized patients’ occupational information using the Industrial Classification for National Economic Activities (GB/T 4754-2017). Data were processed using Excel (Microsoft Office Home and Student 2019, Microsoft Corporation, Redmond, USA).
-
From 2005 to 2023, the overall incidence of OCBP in China exhibited a gradual decline. The highest number of cases was recorded in 2011 (354 cases), while the lowest occurred in 2023 (56 cases) (Figure 1). The proportion of OCBP among COP cases showed an upward trend from 2005 to 2019, but then declined sharply after 2020 (15.26% in 2023 compared to 45.55% in 2019) (Figure 1).
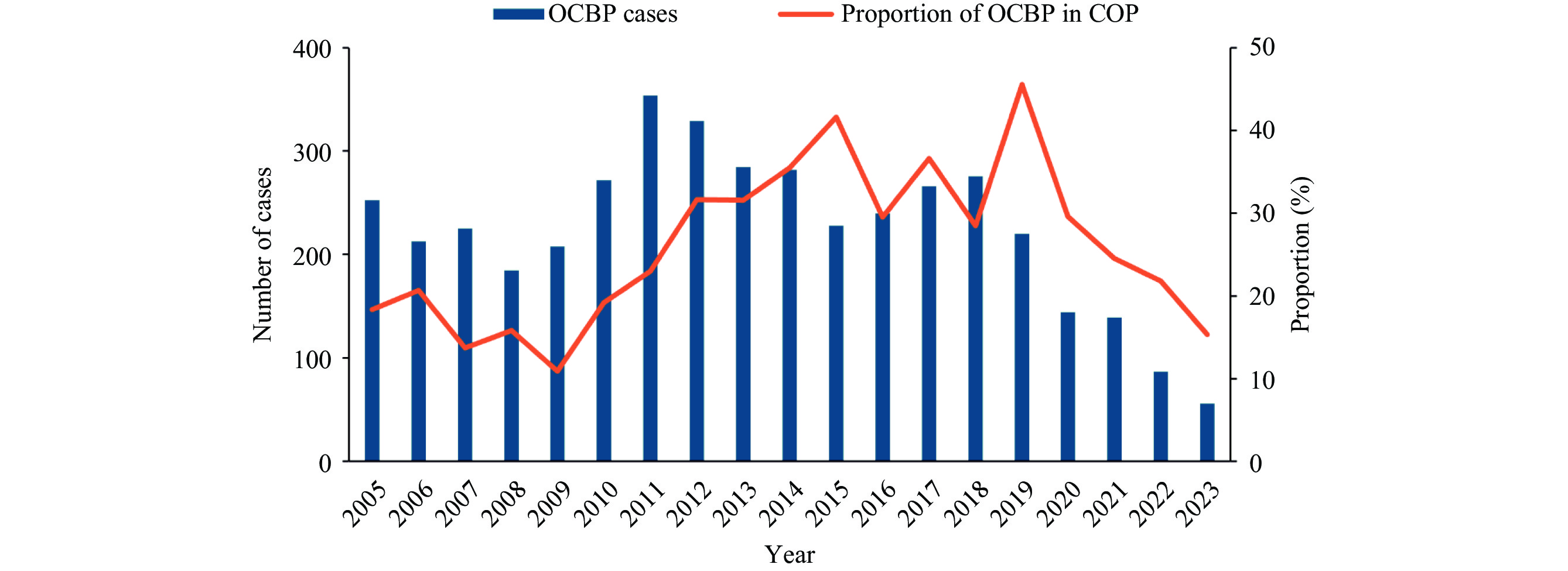 Figure 1.
Figure 1.New cases of OCBP and its proportion of COP cases in China, 2005−2023.
Abbreviation: OCBP=occupational chronic benzene poisoning; COP=chronic occupational poisoning.Between 2020 and 2023, 6 PLADs reported 162 new OCBP cases, accounting for 38% of all nationally reported new COP cases in China. The overall incidence rate of OCBP decreased by 65% from 2019 to 2023 (0.142‰ vs. 0.049‰, based on the number of occupational hazard surveillance populations exposed to benzene). As shown in Table 1, men slightly outnumbered women among OCBP cases (92 vs. 70). Small enterprises constituted the predominant enterprise scale (41.36%), followed by medium-sized enterprises (34.57%). Privately owned (37.65%) and foreign-funded (37.65%) enterprises represented the primary economic types of enterprises with OCBP cases. Sectoral analysis revealed that 85.2% of OCBP cases originated from the manufacturing sector, with construction (2%) and wholesale/retail (2%) being secondary contributors (Figure 2A). In terms of manufacturing sub-sectors, the chemical raw materials and chemical products manufacturing industry accounted for 25% of cases (2020–2023), followed by the petroleum/coal/other fuel processing industry (16%) and the rubber/plastic products industry (13%) (Figure 2B). Further analysis of OCBP in Jiangsu, Sichuan, Shandong, and Tianjin PLADs showed that the industries of OCBP cases in these four regions changed significantly in 2020–2023 compared with 2005–2019 (Figure 3A). The general/special-purpose equipment manufacturing industry is no longer the primary industry of OCBP cases, which is consistent with the overall industry change trend. The number of OCBP cases in the chemical raw materials and chemical products manufacturing industry rose first, followed by the petroleum, coal, and other fuel processing industry, and the rubber and plastic products industry. Notably, the proportion of sporadic cases has increased (2005–2019, 50% vs. 2020–2023, 56%) (Figure 3B).
Item Number of OCBP cases (%) 2020 2021 2022 2023 Total 43 52 42 25 Gender Man 31 (72.1) 26 (50.0) 21 (50.0) 14 (56.0) Woman 12 (27.9) 26 (50.0) 21 (50.0) 11 (44.0) Enterprise scale Large 13 (30.2) 8 (15.4) 8 (19.0) 3 (12.0) Medium 11 (25.6) 21 (40.4) 11 (26.2) 10 (40.0) Small 16 (37.2) 20 (38.5) 20 (47.6) 11 (44.0) Mini 2 (4.7) 2 (3.8) 3 (7.1) 1 (4.0) Unrevealed 1 (2.3) 1 (1.9) 0 0 Ownership type State-owned 4 (9.3) 3 (5.8) 7 (16.7) 4 (16.0) Collective 2 (4.7) 0 1 (2.3) 0 Pooling 0 1 (1.9) 0 0 Private 16 (37.2) 22 (42.3) 13 (31.0) 10 (40.0) Foreign 6 (14.0) 14 (26.9) 11 (26.2) 1 (4.0) Enterprises with Investment from Hong Kong, Macao, and Taiwan 5 (11.6) 2 (3.8) 0 2 (8.0) Stock 6 (14.0) 6 (11.5) 4 (9.5) 3 (12.0) Unrevealed 4 (9.3) 4 (7.7) 6 (14.3) 5 (20.0) Abbreviation: PLAD=provincial-level administrative division; OCBP=occupational chronic benzene poisoning. Table 1. Distribution of enterprise scale and ownership type with OCBP cases in 6 PLADs, 2020–2023.
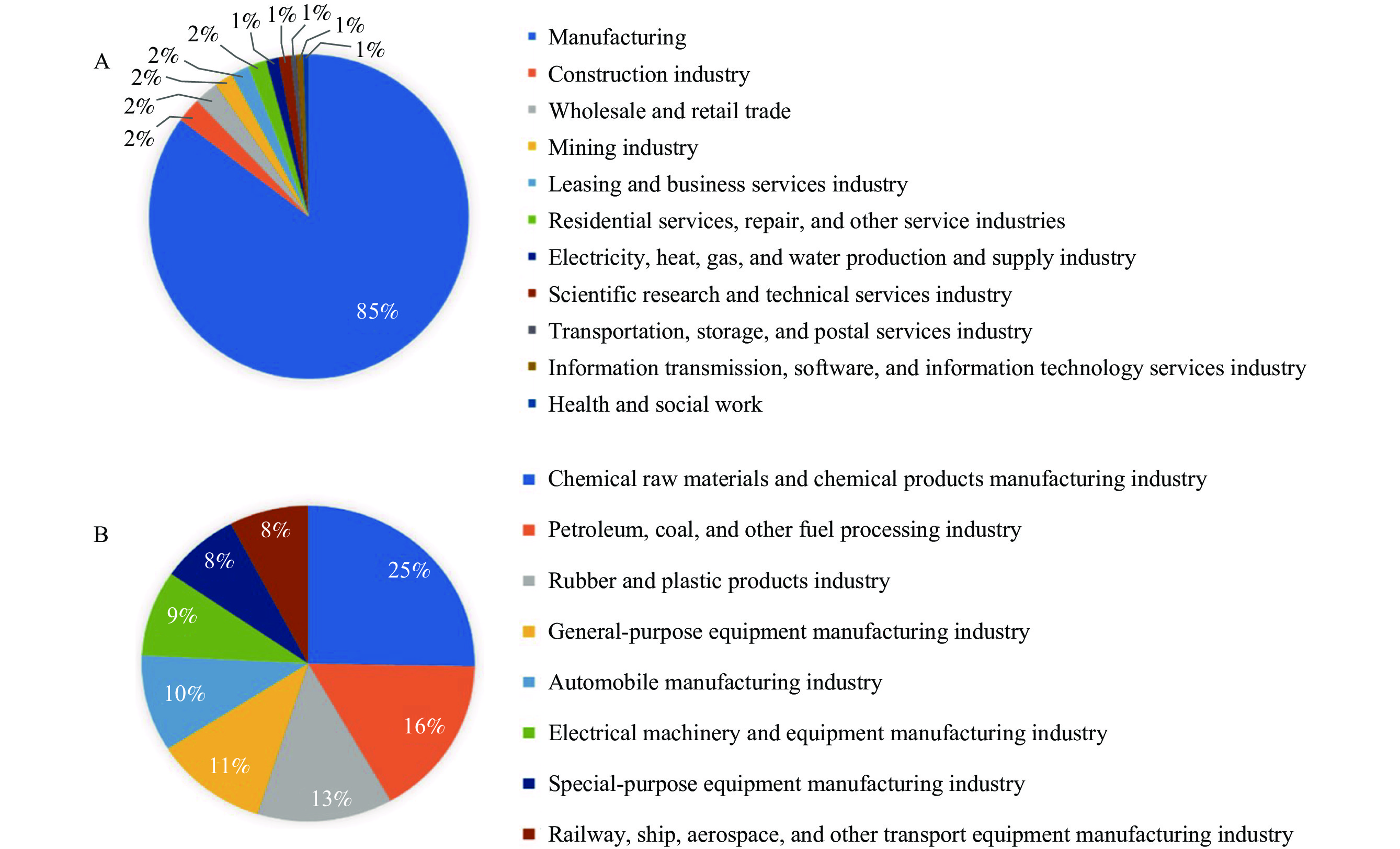 Figure 2.
Figure 2.Distribution of industries with the most OCBP cases from 2020 to 2023 in 6 PLADs. (A) Distribution of OCBP cases between manufacturing and non-manufacturing industries; (B) Distribution of OCBP cases in manufacturing.
Abbreviation: OCBP=occupational chronic benzene poisoning; PLAD=provincial-level administrative division.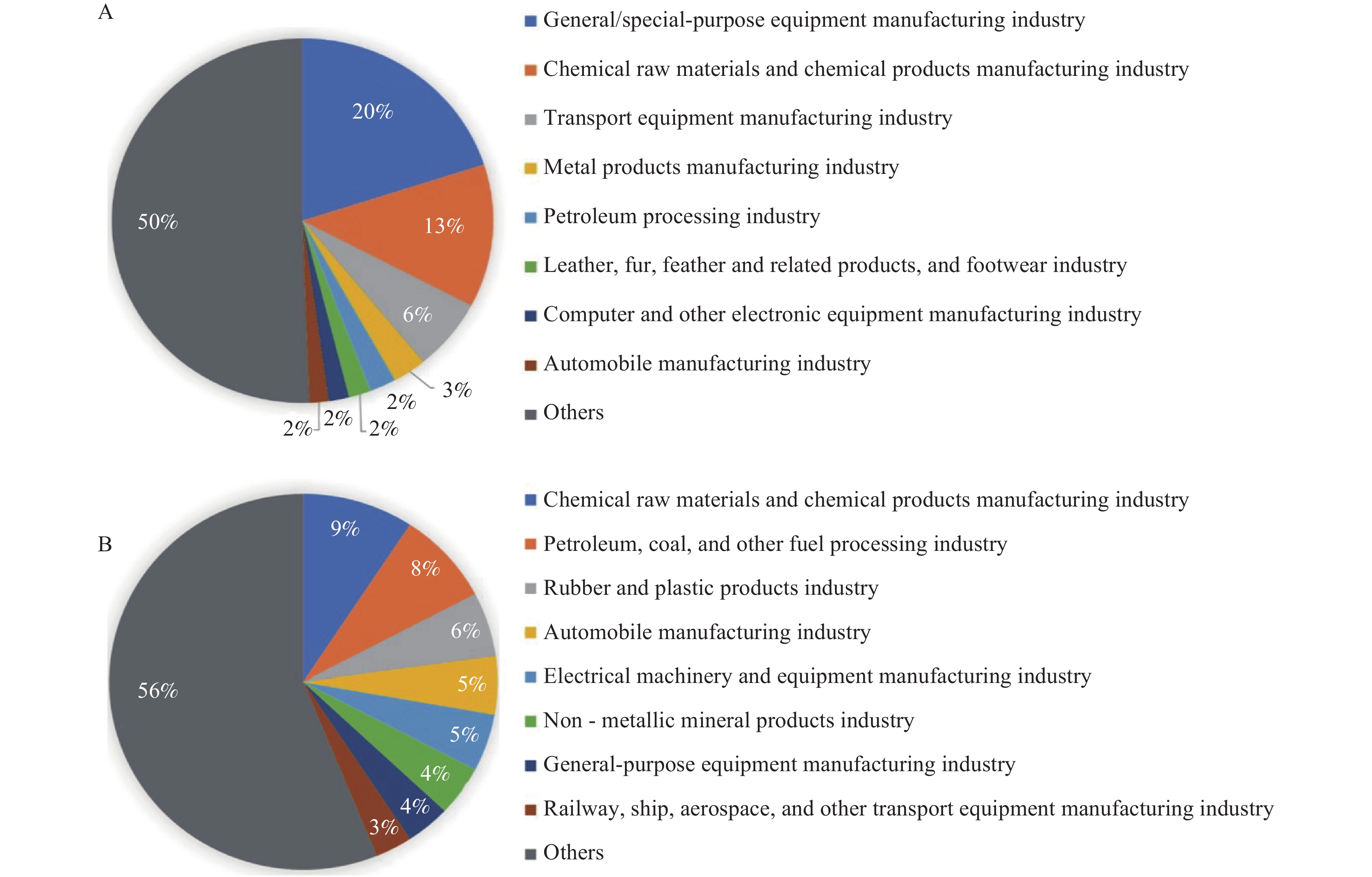 Figure 3.
Figure 3.Dynamic distribution of OCBP cases in Jiangsu, Sichuan, Shandong, and Tianjin manufacturing sub-industries. (A) 2005–2019; (B) 2020–2023.
Abbreviation: OCBP=occupational chronic benzene poisoning. -
The sharp decline in OCBP incidence and its proportion among COP cases from 2020 to 2023 likely reflects reduced workplace benzene exposure. We selected occupational hazard surveillance populations exposed to benzene in six PLADs in 2019 and 2023 to estimate OCBP incidence, with results confirming both decreasing absolute case numbers and composition ratios. Surveillance data from 2019 indicate that 98.6% of benzene-exposed enterprises in six PLADs (Shandong, Jiangsu, Fujian, Sichuan, Guangdong, and Tianjin) maintained time-weighted average benzene concentrations ≤3 mg/m3, with 99.4% complying with short-term exposure limits (≤6 mg/m3) (4). Based on these findings and nearly three decades of molecular epidemiological studies on benzene conducted by our research group and other researchers, we revised the occupational exposure limit for benzene from 6 mg/m3 to 3 mg/m3 in November 2022, which is lower than that in developed countries such as the United States (1 ppm, equivalent to 3.25 mg/m3) (4). Currently, the main occupational benzene exposure in the United States occurs in the petrochemical industry, with an average exposure level of only 0.24 ppm (0.78 mg/m3) and an occupational benzene poisoning incidence rate of 0.004‰ (5–6). China leads the world in benzene production and use, with the total number of benzene workers (over 1,000,000) far exceeding that of other countries, including Brazil (approximately 770,000) (7), the United Kingdom (approximately 300,000) (8), Poland (approximately 13,000) (9), and Finland (less than 2,300) (10). Since low-concentration benzene exposure (<3.25 mg/m3) poses hematotoxicity and carcinogenic risks (11), China needs to enhance its management and control systems for benzene and related occupational diseases to protect its large benzene-exposed population and reduce the risk of benzene poisoning and leukemia. This study found that as new benzene poisoning cases decrease, the industries with high incidence rates are also changing. Given the lag period associated with benzene poisoning, ongoing monitoring of benzene poisoning incidence and the dynamic changes in high-risk industries following China’s reduction of the time-weighted average benzene exposure limits can provide direction for supervision and enhance preventive measures.
This study compares the dynamic changes in industries where OCBP occurred from 2020 to 2023 versus 2005 to 2019, identifying the primary industries where benzene poisoning currently occurs. This research provides direction for strengthening supervision of key occupational diseases and further reducing the incidence of benzene-induced leukemia. Our investigation found that foreign-funded enterprises were also one of the main economic types associated with OCBP. These enterprises often employ a “core factory + subcontracting” model, potentially outsourcing benzene-related processes to smaller facilities with inadequate occupational health investments, thereby exacerbating OCBP risks (12–13). Notably, the manufacturing sub-sectors with high OCBP incidence shifted from general/special-purpose equipment manufacturing to chemical/petroleum industries during 2020−2023, reflecting sector-specific benzene utilization patterns. While technological advancements, such as electrostatic spraying and benzene-free solvents, have reduced benzene dependence in equipment manufacturing (14–15), foundational chemical industries remain challenged by their intrinsic reliance on benzene and limited technical alternatives, highlighting disparities in occupational protection during industrial upgrading.
This study was subject to several limitations. First, incomplete coverage of benzene-exposed workers in occupational health examinations may result in many workers missing check-ups, underestimating the total number of benzene-exposed workers, and possibly inflating the calculated OCBP incidence rates. Second, the regional data from six PLADs may not fully represent national epidemiological patterns. Expanded multi-regional investigations could inform more targeted interventions. Third, while changes in the composition ratio (OCBP/COP) can partially reflect trends in occupational chronic benzene poisoning cases, the lack of precise baseline data on benzene-exposed workers limits the interpretability of this metric. Specifically, it cannot distinguish between: 1) a true reduction in the absolute risk of OCBP, and 2) a relative increase in other occupational poisoning cases. Future studies should include population data on benzene exposure to allow for more accurate risk assessments.
This study suggests that both the number of cases and the incidence of OCBP in China are declining, indicating substantial progress in controlling occupational benzene exposure. However, since benzene poisoning represents a high-risk group for leukemia, strengthened occupational disease surveillance remains critical for sector-specific OCBP management. Current epidemiological features should guide resource allocation and cost-effective policy formulation. Preventive measures should emphasize rigorous enterprise monitoring, including regular assessments of benzene concentration to ensure compliance with national standards (PC-TWA ≤3 mg/m3, PC-STEL ≤10 mg/m3), especially for manufacturing, private, and small- and medium-sized enterprises, alongside enhanced worker education and health management protocols. For foreign-funded enterprises, it is necessary to strengthen the supervision of supply chains and subcontracting links by requiring integration of original entrusted manufacturers (OEM) factories and contractors into a unified occupational health management system, and improve occupational health surveillance.
-
All the participants involved in this study.
HTML
Epidemiological Profile
| Citation: |

|