
 Download:
Download:




-
Scrub typhus, also known as jungle typhus, represents a significant public health challenge in the Asia-Pacific region. This vector-borne disease is transmitted to humans through the bite of infected chiggers carrying Orientia tsutsugamushi (formerly Rickettsia tsutsugamushi) (1). The first documented case of human infection with O. tsutsugamushi in China was identified in 1948 in Guangzhou City, Guangdong Province (2). By the 1980s, scrub typhus cases occurred predominantly in regions south of the Yangtze River, including Zhejiang Province in eastern China and Yunnan Province in western China (3). Since the 1980s, the epidemiological distribution of scrub typhus has expanded rapidly throughout China. The geographic spread has gradually extended from provincial-level administrative divisions (PLADs), south of the Yangtze River to northern PLADs, including Tianjin, Shandong, and the three northeastern PLADs (4). The incidence of scrub typhus has demonstrated a marked increase in recent years, rising from 0.09/100,000 in 2006 to 1.60/100,000 in 2016, yet it remains an underrecognized tropical infectious disease (5).
In recent years, climate change and human expansion into previously uninhabited areas have contributed to a clear upward trend in scrub typhus incidence. This study analyzed the epidemiological characteristics and spatiotemporal clustering patterns of scrub typhus in China from 2006 to 2023 to identify high-risk populations and geographic aggregation areas. These findings will provide an evidence base for local health departments to implement targeted surveillance and control strategies, and will inform the development of preventive measures for travelers to endemic regions.
-
Scrub typhus data were obtained from the China Information System for Disease Control and Prevention (CISDCP). Case definitions followed guidelines established by the Chinese Center for Disease Control and Prevention (6). We utilized Excel 2010 (Microsoft, Redmond, WA, USA) for data analysis and statistical visualization. Temporal trend analysis employed Joinpoint 5.1.0 to calculate the average annual percentage change (AAPC) and annual percent change (APC). Statistical analyses were conducted using RStudio (version 4.4.1, Posit, Boston, MA, USA), including Mann-Whitney U tests for non-parametric comparisons, Cochran-Armitage tests for trend analysis, and binary logistic regression modeling to examine the relationship between median interval from illness onset to case diagnosis (Tdiag) and mortality risk. Spatial-temporal clustering analysis utilized SaTScan software (version 9.1.1, Martin Kulldorff, Boston, MA, USA) for space-time scan statistics (STSS) as developed by Kulldorff. We identified high-risk clusters of scrub typhus at the county level across four distinct time periods. Monte Carlo simulations generated P values using a Poisson model, while loglikelihood ratio (LLR) and relative risk (RR) values were calculated to test hypotheses for each scanning window. ArcGIS Desktop software (version 10.3, Esri, Redlands, California, USA) provided visualization capabilities for spatial analysis results.
-
Between 2006 and 2023, China reported a total of 283,102 scrub typhus cases. Of these, 272,061 cases (96.1%) received clinical diagnoses, while 11,041 cases (3.9%) were confirmed through laboratory testing. Additionally, 103 deaths were documented, yielding an average annual incidence rate of 1.12 per 100,000 individuals. The Average Annual Percentage Change demonstrates that scrub typhus incidence in China increased by an average of 19.4% annually. The Joinpoint regression model revealed 2 significant turning points in scrub typhus incidence from 2006–2023, allowing categorization into 3 distinct phases: a rapid increase period [APC2006–2013= 37.1%, 95% confidence interval (CI): 31.4%, 43.0%], a slow increase period (APC2014–2018=13.4%, 95% CI: 4.6%, 23.0%), and a peak-plateau period (APC2019–2023=−0.2%, 95% CI: −3.2%, 3.0%) (Figure 1).
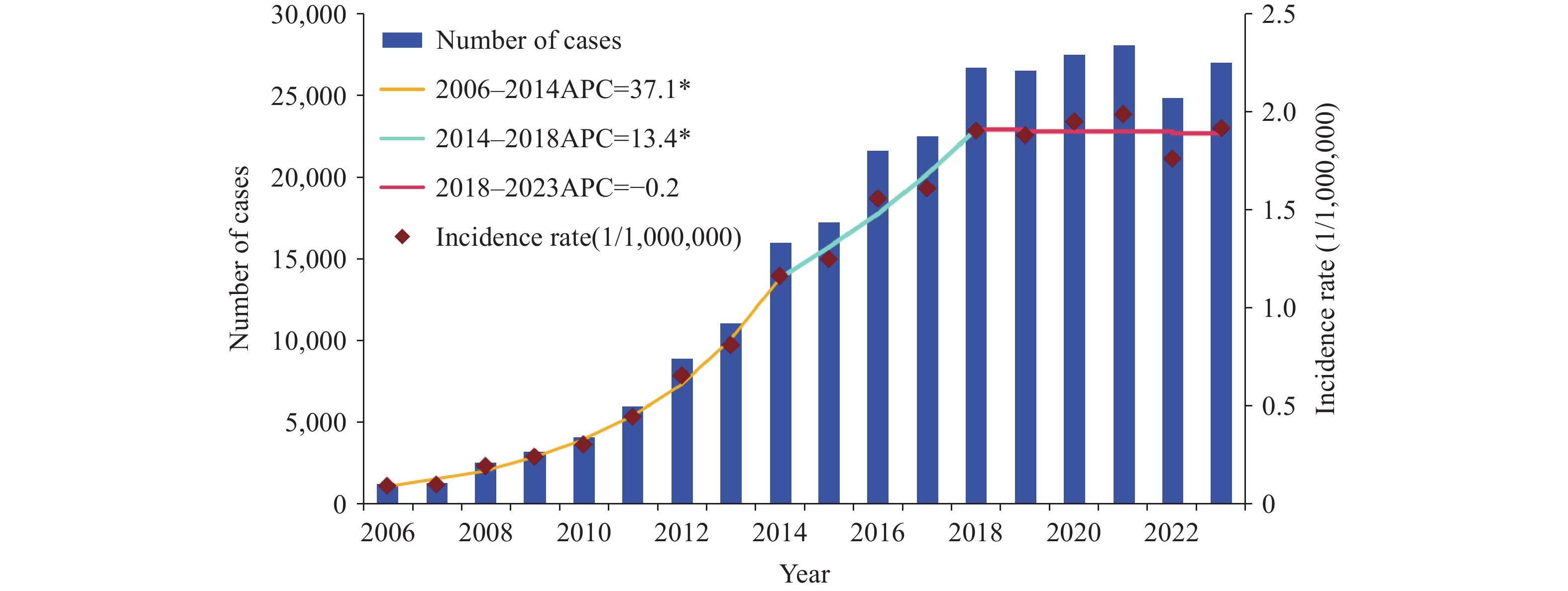 Figure 1.
Figure 1.Trends in the incidence of scrub typhus, 2006–2023.
Abbreviation: APC=annual percent change.
* Indicates that the APC is significantly different from zero at the α=0.05 level (P<0.05).
Seasonal analysis revealed that peak incidence occurred between June and November, accounting for 88.47% of total cases, while lower incidence was observed from December to May, with consistent patterns maintained across different years (Figure 2A). Analysis of the 14 PLADs with the highest case numbers, collectively representing 98.82% of all reported cases, demonstrated 3 distinct seasonal patterns throughout China: 1) Autumn pattern: This pattern exhibited a distinct single-peak configuration with maximum incidence in October-November and a brief epidemic duration, encompassing Beijing, Henan, Shandong, Anhui, and Jiangsu PLADs (Figure 2B); 2) Summer pattern: This pattern demonstrated a single peak during the summer months, with epidemics spanning June through September, including Yunnan, Sichuan, and Hunan provinces (Figure 2C); 3) Summer-autumn pattern: This pattern displayed 2 peaks occurring in June-July and September-October, respectively, resulting in the most extended epidemic period and including Guangdong, Guangxi, Fujian, Jiangxi, and Zhejiang PLADs (Figure 2D).
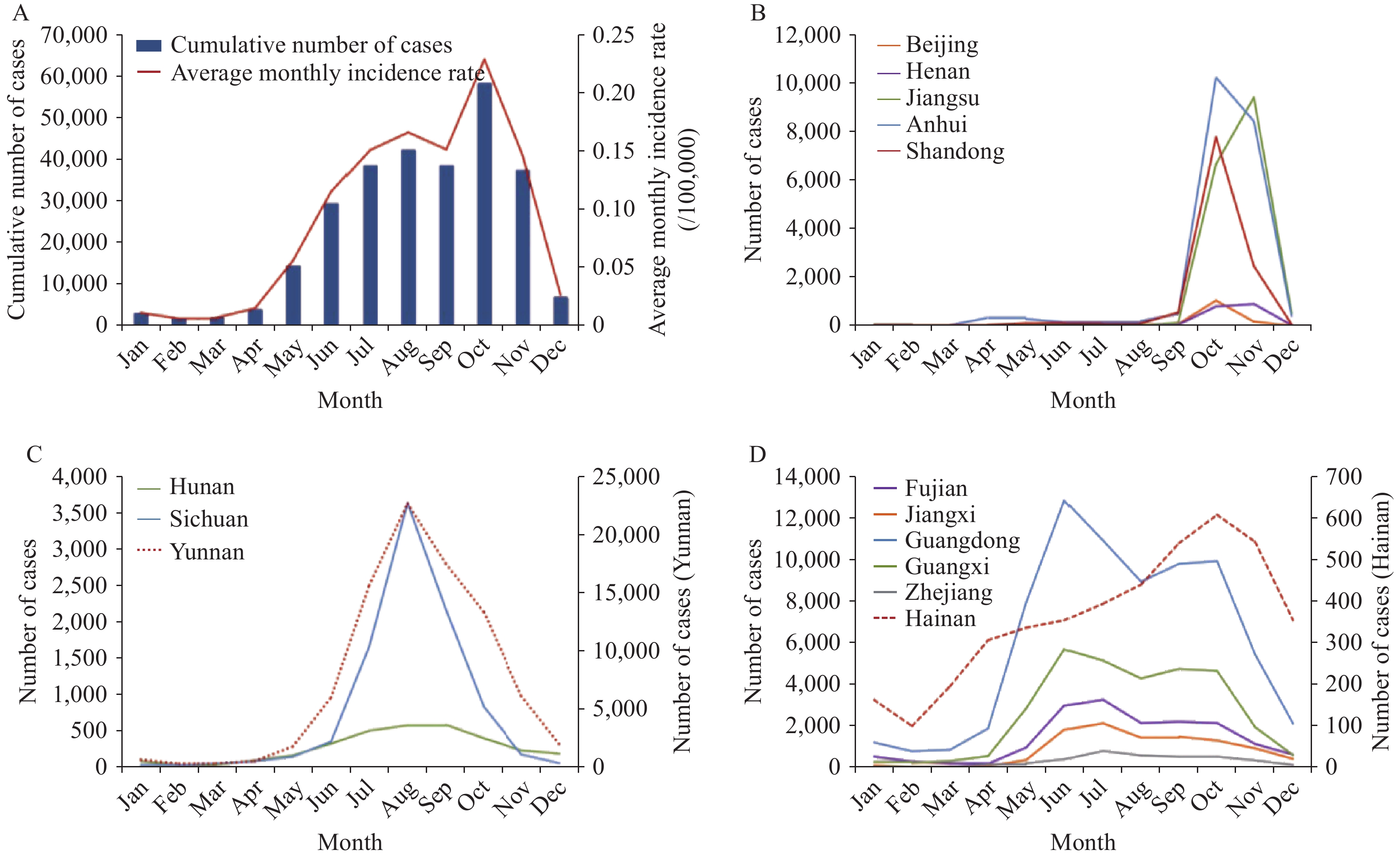 Figure 2.
Figure 2.Seasonal distribution of scrub typhus cases in China, 2006–2023. (A) Seasonal distribution in China; (B) Autumn pattern; (C) Summer pattern; (D) Summer–autumn pattern.
-
Age distribution analysis revealed a growing proportion of individuals aged ≥45 years (AAPC=2.0%, 95% CI: 1.0%, 2.9%). The incidence across different age groups displayed a bimodal distribution, with peaks primarily between 55–84 years and, to a lesser extent, in the 0–9 years age bracket. The highest incidence was observed among children aged 1–5 years (Figure 3B). Regarding gender distribution, the male-to-female ratio was 0.89:1. A significant decrease in male cases was noted with advancing age (Z=−62.78, P<0.001), with a higher proportion of males in the 0–45 age group and more females in the ≥45 age group (Figure 3A). Occupational analysis revealed that farmers comprised the majority of cases at 76.81%, followed by children in scattered rural areas (5.30%), household members and preschool children (5.09%), and students (4.44%). There was a significant steady increase in the proportion of farmers from 2006 to 2023, rising from 60.29% to 76.69% (AAPC=1.2%, 95% CI: 0.7%, 1.7%).
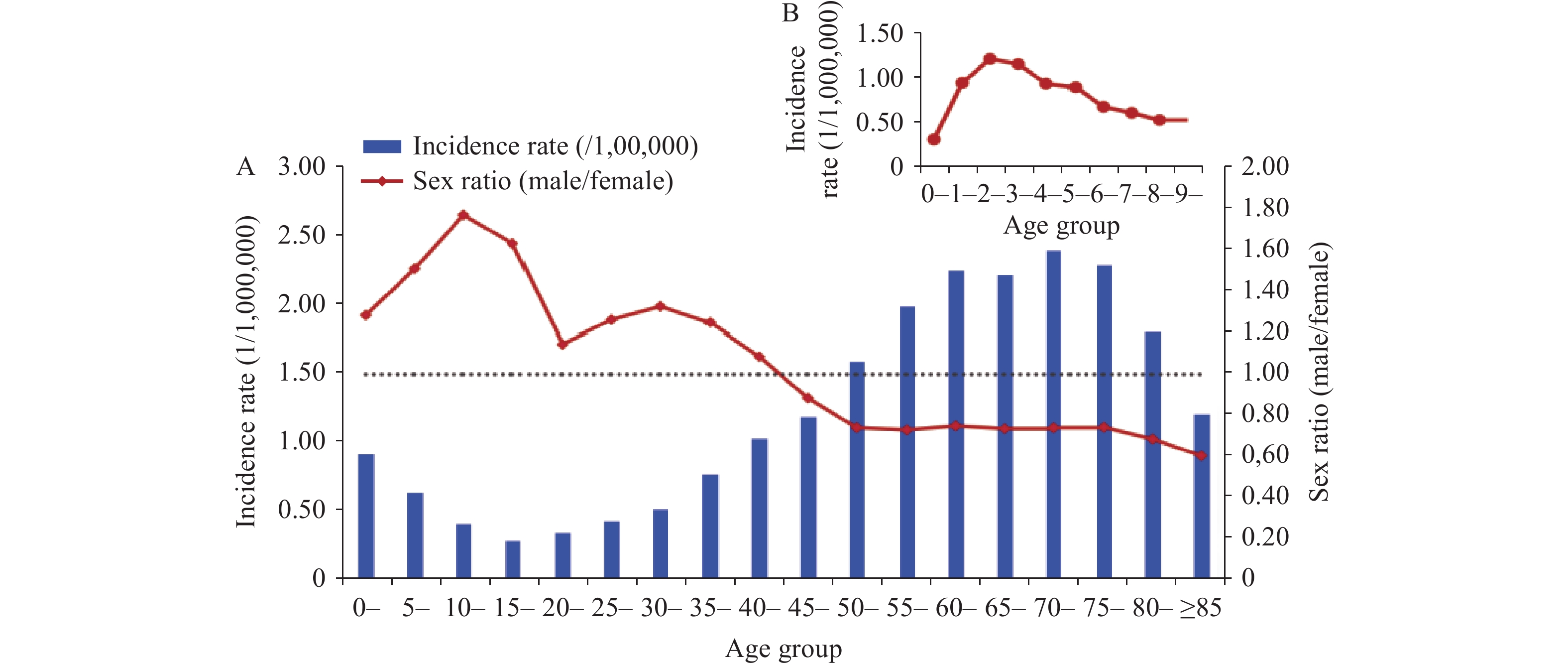 Figure 3.
Figure 3.Age and sex distribution of scrub typhus. (A) Age and sex distribution of scrub typhus; (B) Incidence among children aged 0–10 years.
-
The incidence of scrub typhus in China increased dramatically from 0.095/100,000 to 2.357/100,000 between 2006 and 2023. During this 18-year period, a total of 283,102 cases were reported across China. The geographic distribution was notably concentrated in 5 PLADs, which collectively accounted for 80.18% of all cases: Yunnan Province with 84,735 cases (28.87%), Guangdong Province with 69,957 cases (25.26%), Guangxi Zhuang Autonomous Region with 30,133 cases (10.88%), Anhui Province with 20,491 cases (7.40%), and Jiangsu Province with 16,765 cases (6.05%). The geographic scope of scrub typhus expanded substantially from 2006 to 2023, with affected areas growing from 217 counties/districts in 2006 to 1,086 counties/districts in 2023. To characterize the evolving geographic distribution patterns of scrub typhus in China from 2006 to 2023, we divided the study period into 4 phases: 2006–2009, 2010–2013, 2014–2018, and 2019–2023, and generated incidence maps at the county level. The analysis revealed that geographic distribution changes were minimal in 2010–2013 compared with 2006–2009. However, during 2014–2018, the geographic distribution expanded significantly from southwestern, southern, and eastern China to central and northern China, with further widespread expansion occurring in 2019–2023 (Figure 4).
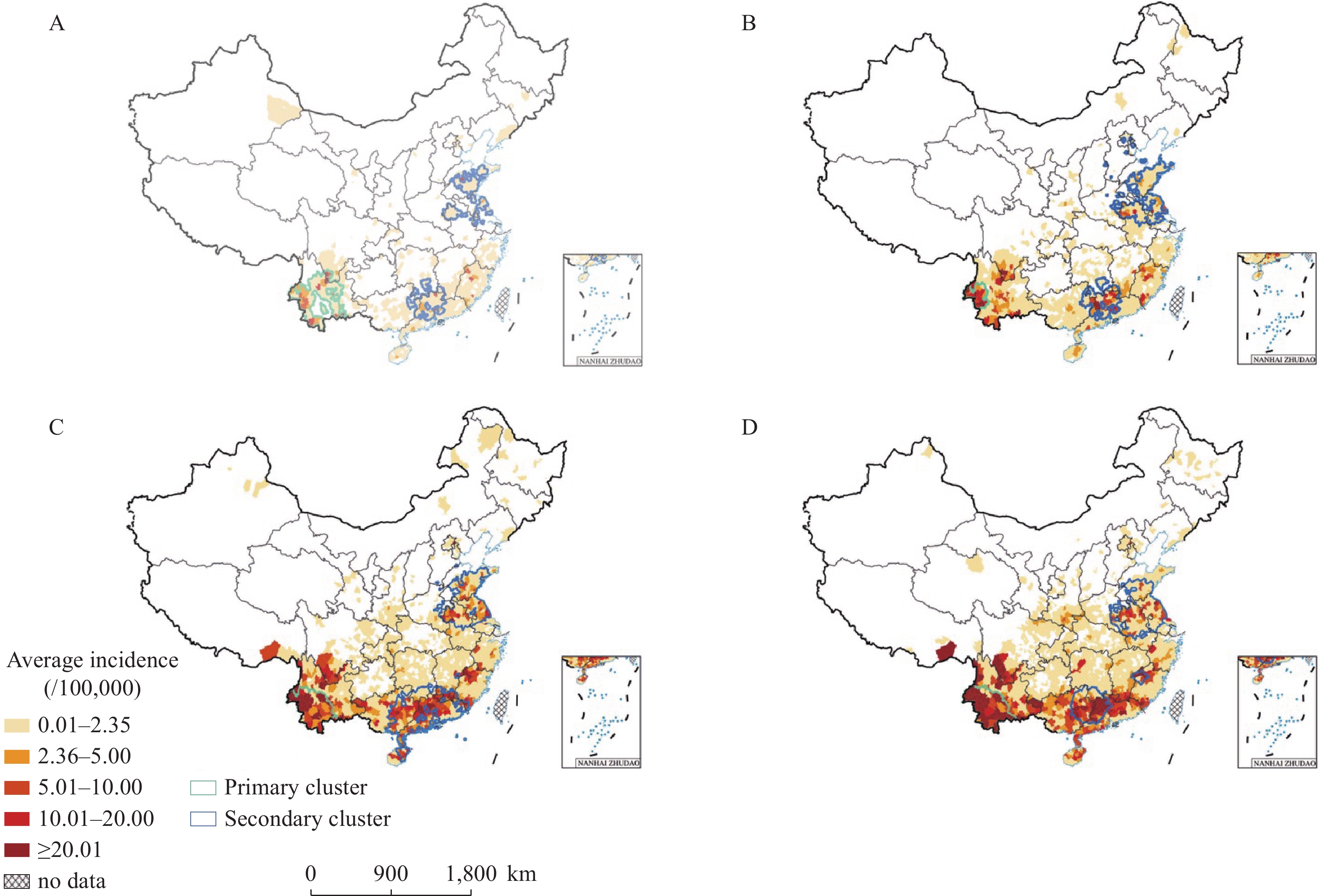 Figure 4.
Figure 4.Annualized average incidence and space-time clusters of scrub typhus cases at the county level in China, 2006–2023. (A) Spatial clustering from 2006 to 2009; (B) Spatial clustering from 2010 to 2013; (C) Spatial clustering from 2014 to 2018; (D) Spatial clustering from 2019 to 2023.
Map approval number: GS京(2025)0900号The spatiotemporal cluster analysis at the county level revealed distinct clustering patterns across different time periods (
Supplementary Table S1 ). During 2006–2009 (Figure 4A), the primary cluster was centered in Gengma County, Yunnan Province, with a radius of 458.1 km encompassing 5 counties in Panzhihua, Sichuan Province, and 65 counties in Yunnan Province, active from June 6, 2008, to December 3, 2009. Two secondary clusters were identified: one centered in Tancheng County, Shandong Province, and another in Yangshan County, Guangdong Province, collectively affecting 134 counties across Jiangsu, Anhui, Shandong, Henan, Guangdong, Hunan, Guangxi, and Jiangxi PLADs. During 2010–2013 (Figure 4B), the primary cluster shifted to Mang City, Yunnan Province, with a 181.7 km radius covering 17 counties, active from June 6, 2012, to December 3, 2013. Two secondary clusters were centered in Yangshan County, Guangdong Province, and Weicheng County, Shandong Province, impacting a total of 228 counties across Guangdong, Guangxi, Hunan, Jiangxi, Shandong, Jiangsu, Anhui, Henan, Beijing, Hebei, Shanxi, and Tianjin. During 2014–2018 (Figure 4C), the predominant cluster was located in Menglian County, Yunnan Province, with a radius of 354.2 km, covering 44 counties from June 7, 2016, to December 3, 2018. Two secondary clusters emerged, one centered in Jinwan County, Guangdong Province, and the other in Feixian County, Shandong Province, encompassing a total of 373 counties across Guangdong, Guangxi, Hunan, Fujian, Jiangxi, Hainan, Hebei, Jiangsu, Anhui, and Shandong PLADs. During 2019–2023 (Figure 4D), the primary cluster remained in Menglian County, Yunnan Province, with a radius of 376.2 km, encompassing 47 counties from June 7, 2021, to December 3, 2023. Additionally, 3 secondary clusters emerged, centered in Pinggui County, Guangxi Zhuang Autonomous Region; Lingbi County, Anhui Province; and Taining County, Fujian Province, affecting 271 counties across Guangdong, Guangxi, Hunan, Jiangsu, Anhui, Shandong, Henan, Fujian, and Jiangxi PLADs. -
During 2006–2023, 103 deaths were reported, yielding a case fatality rate of 36.4 per 100,000 cases, with fatalities documented in every year except 2009. The years with the highest mortality burden were 2016 and 2011, recording 12 and 11 deaths, respectively. The male-to-female ratio among fatal cases was 1.4:1. Age distribution was predominantly concentrated in the ≥45 years group, with 87 cases (84.5%) in this demographic. The highest case fatality rates were observed in the ≥80 years group (103.8 per 100,000), followed by the 70–74 years group (70.7 per 100,000), 75–79 years group (58.5 per 100,000), and 0–4 years group (52.6 per 100,000) (
Supplementary Table S2 ).The median interval from illness onset to case diagnosis (Tdiag) among fatal cases was 8 days [interquartile range (IQR): 4–10 days], compared to 5 days (IQR: 2–8 days) for non-fatal cases. The Mann-Whitney U-test demonstrated statistical significance (Z=−3.586, P<0.001). To investigate the effect of Tdiag (<2 days, 2–7 days, >7 days) on mortality risk, we developed a binary logistic regression model, adjusting for covariates including gender (male, female), age group (<20, 20–39, 40–59, ≥60 years), and occupation (farmers, others, students/preschool children). Results demonstrated that cases with Tdiag >7 days had significantly higher mortality risk than those with Tdiag <2 days [odds ratio (OR)=2.0, 95% CI: 1.2, 3.6]. Model fit was validated using the Hosmer-Lemeshow test, which indicated good model performance (χ2=12.098, P=0.147). We constructed a receiver operating characteristic (ROC) curve and calculated the area under the curve (AUC) to evaluate the model’s predictive capability. The AUC was 0.746 (95% CI: 0.6954, 0.7967), confirming the model’s accuracy (
Supplementary Table S3 ). -
The incidence of scrub typhus in China increased significantly from 2006 to 2023 (AAPC=19.4%) and has now reached a peak plateau phase. We identified 3 distinct seasonal patterns across China: summer, autumn, and summer-autumn patterns. The disease predominantly affects middle-aged and elderly farmers, with gender distribution varying across age groups. The geographical distribution has progressively expanded from southwestern, southern, and eastern China to central and northern regions, with primary clusters concentrated in Yunnan Province. Cases with diagnostic delays exceeding 7 days (Tdiag>7 days) demonstrated significantly higher mortality risk (OR=1.9, 95% CI: 1.1, 3.4).
Scrub typhus incidence has risen substantially in China and other countries, including Japan and Republic of Korea (1,3,7). This increase likely stems from multiple factors: advances in diagnostic techniques, human encroachment into previously uninhabited areas, and climate change (8-9). In 2009, the China CDC published the “Technical Guidelines for Prevention and Control of Tsutsugamushi (for Trial Implementation)”, which standardized case reporting and enhanced diagnostic capabilities nationwide, facilitating improved case identification. Research demonstrates that urbanization has increased human exposure to vector mites, elevating infection risk (7). Additionally, studies suggest that rising average temperatures and increased heatwave frequency correlate with higher scrub typhus case numbers, indicating that global warming may contribute to this trend (10). Scrub typhus has expanded across mainland China from southwestern, southern, and eastern coastal regions to central, northern, and northeastern areas, with new endemic locations continuously identified (4).
The seasonal distribution of scrub typhus exhibits regional variability, consistent with several previous studies (2). We identified 3 distinct seasonal patterns in China: summer, autumn, and summer-autumn patterns. This variation likely relates to the population distribution and seasonal fluctuation of chigger vectors (11). Leptotrombidium delicense, L. scutellare, L. sialkotense, L. rubellum, L. wenense, and L. insulare have been confirmed as scrub typhus vectors in China, though many potential vectors remain unidentified (11–13). Vector chiggers play crucial roles in scrub typhus epidemiology and disease transmission. Therefore, strengthening nationwide chigger monitoring is essential to fully understand vector distribution in epidemic regions. The age distribution primarily affects the 45–70-year age group, with occupational distribution mainly among farmers, aligning with numerous domestic and international studies (4,10,14). However, unlike other research (8), we observed higher male proportions in the 0–44 age group, while females predominated in the ≥45 age group. This pattern may reflect middle-aged male migration to urban areas for employment, leaving women and elderly individuals in rural areas where increased agricultural activities heighten scrub typhus exposure. The slight peak in scrub typhus incidence among children aged 0–9 years can be attributed to several factors: guardians may bring children to fields during labor, and children’s limited self-protection awareness increases disease exposure risk. Additionally, because children receive more intensive care and attention, illness detection occurs more readily. Misdiagnosis or delayed diagnosis can have severe consequences in children due to their lower immunity, necessitating heightened clinical attention.
Despite the availability of specific antimicrobial treatments for scrub typhus, the absence of distinctive clinical symptoms complicates its differentiation from other febrile illnesses, including dengue fever, severe fever with thrombocytopenia syndrome, and leptospirosis. Misdiagnosis or delayed diagnosis may result in severe complications and increased mortality (8). Our study demonstrated that patients with Tdiag >7 days had a 1.9-fold increased mortality risk compared to those diagnosed within 2 days, consistent with findings from other investigations (15). Therefore, diagnostic delays significantly elevate the risk of death. As scrub typhus continues to spread to emerging regions, enhanced training programs focusing on scrub typhus diagnosis should be developed for healthcare providers in these areas.
This research has several limitations. First, scrub typhus was incorporated into the infectious disease surveillance system in 2006, but standardized reporting criteria were not established until the release of ‘Technical Guidelines for Prevention and Control of Tsutsugamushi (for Trial Implementation)’ in 2009, which may have compromised reporting quality during the initial period. Second, the data originated from a passive surveillance system, potentially resulting in underreporting and misreporting that could affect data accuracy. Third, this study lacked vector and host data, which are considered important variables influencing disease transmission dynamics.
In conclusion, scrub typhus in China has reached a peak plateau with expanding epidemic regions. Therefore, comprehensive control measures must be implemented. These measures should include enhanced physician training in diagnosis and treatment, particularly in newly emerging areas, to ensure timely case detection. Additionally, increased public awareness and education campaigns in endemic areas can guide at-risk populations in adopting appropriate protective measures.
HTML
Temporal Trends and Seasonality
Social-Demographic Characteristics
Spatial and Temporal Distributions
Distribution of Fatal Cases and Mortality Risk Factors
| Citation: |

|