
 Download:
Download:




-
Human immunodeficiency virus (HIV) remains a major global public health threat. The burden is disproportionately concentrated in settings with constrained health and economic resources, where access to timely diagnosis and sustained antiretroviral therapy (ART) is limited. Liangshan Yi Autonomous Prefecture, situated in southwest China, has been a focal area for national HIV prevention efforts. Following successful harm-reduction programs that curtailed injection drug use transmission, heterosexual contact emerged as the dominant transmission route from 2014 onward, accounting for 59.0% of newly diagnosed cases in 2017 and 79.4% in 2019 (1). Although national initiatives have slowed the overall epidemic trajectory (2–3), gaps remain along the HIV care cascade. Late presentation, delayed ART initiation, and poor retention in care leave a substantial proportion of HIV-positive individuals without durable viral suppression. Consequently, Liangshan’s treatment coverage and virological suppression continue to lag behind national averages, undermining the UNAIDS 95-95-95 targets and adversely affecting survival and secondary transmission (4–5).
To address these challenges, the “Action Plan for HIV Prevention and Health Poverty Alleviation in Liangshan Prefecture” was initiated in September 2017 (Phase I, 2017–2020), subsequently expanded into Phase II and hereafter referred to as the “Action Plan". The Action Plan introduced a comprehensive strategy, aiming to expand testing and treatment coverage, reduce mortality, and improve healthcare accessibility (3,6). Phase I targeted four “key counties” (Butuo, Zhaojue, Yuexi, Meigu) with high HIV prevalence, and Phase II extended these successful measures to all 17 counties in Liangshan. The core measures of the comprehensive strategy included universal HIV screening integrated into routine health checkups, real-time monitoring of the ART treatment cascade, “Three Lines and One Network Base” technical support system and “1+M+N” community-based management model, which were specifically designed to enhance multi-sector collaboration and deliver contextually adapted HIV/AIDS services.
While early reports documented substantial increases in HIV testing and treatment coverage, the long-term impact of the comprehensive strategy on treatment outcomes, particularly mortality, has yet to be formally evaluated. Therefore, this study conducted a population-based assessment of heterosexually transmitted HIV-infected individuals diagnosed during 2008-2024, employing interrupted time series (ITS) analysis and COX proportional hazards model to quantify changes in treatment coverage and mortality and to explore disparities across subgroup populations, to optimize HIV control strategies in Liangshan and other high-burden settings.
-
This study utilized routine case reporting data retrieved from China’s HIV/AIDS Comprehensive Response Information Management System (CRIMS). The study population comprised adults aged 15 years and older who were first diagnosed with heterosexually transmitted HIV in Liangshan between 2008 and 2024. Data were de-identified prior to analysis.
The comprehensive strategy combined several key measures: 1) universal HIV screening integrated into routine health checkups, achieving up to 98% coverage among residents in key counties; 2) real-time monitoring of the ART cascade with enhanced measures such as timely patient referrals and differentiated service delivery; 3) governance through the “Three Lines and One Network Base” technical support system, which integrates prefecture- and county-level CDC, hospitals, and maternal-child-health centers (“Three Lines”) with a robust grassroots community network (“One Network Base”) to ensure comprehensive care; and 4) the “1+M+N” community-based management model, which clearly defines the responsibilities of township government (“1”), township healthcare institutions (“M”), and village-level health workers (“N”) to maintain continuity and effectiveness of HIV care. Phase I focused resources on four HIV high-prevalence counties, while Phase II expanded to all 17 counties (3,6).
-
The primary outcomes for assessing the comprehensive strategy’s effectiveness were treatment coverage and mortality. Follow-up time, as recorded in months, started on the date of HIV diagnosis to either the date of death, date of last follow-up visit, or December 31, 2024, whichever came first. Cox proportional hazards regression was used to identify potential risk factors for mortality, with hazard ratios (HRs) quantifying the impact of the comprehensive strategy on mortality after controlling for demographic factors (7). A detailed methodological explanation is provided in the
Supplementary Material . -
Given that randomization was infeasible or unethical in this context, ITS analysis was conducted to evaluate the comprehensive strategy’s impact on treatment coverage and mortality at the population level. Segmented linear regression models quantified both the immediate and long-term effects of the intervention, with 2018 designated as the intervention (comprehensive strategy) start point in this study. The model is as follows:
$$ {Y} _{ {t} } \mathrm= {\beta } _{ {0} } {+\beta } _{ {1} } {T+\beta } _{ {2} } {X} _{ {t} } {+\beta } _{ {3} } {(T-T} _{ {0} } {)X} _{ {t} } {+\varepsilon } $$ Where: Yt denotes the outcome variable at time t, T is the continuous time variable, β0 is the pre-intervention initial level, β1 represents the slope before the intervention, reflecting the annual trend of change before the intervention, β2 is the immediate change in the level of the outcome indicator before and after the intervention, β3 represents the change in the slope before and after the intervention, (β1+β3) is the slope after the intervention, reflecting the annual average trend of change after the comprehensive strategy’s implementation, ε represents the random error (8). Additional detailed methodological explanations are provided in
Supplementary Material .The Newey-West method (9) was employed to control for autocorrelation and heteroscedasticity, providing 95% confidence intervals (CIs) with optimal lag selection through an automatic bandwidth procedure. Subgroup analyses were conducted to examine disparities by gender (male vs. female), region (key counties vs. non-key counties), disease stage (HIV vs. AIDS), and ART status (yes vs. no). The regional stratification of Liangshan was based on an HIV prevalence threshold of 1%. Four counties demonstrating HIV prevalence above 1% were classified as key counties (Butuo, Zhaojue, Yuexi and Meigu), while the remaining 13 counties were designated as non-key counties.
-
All statistical tests were two-sided, with a significance threshold set at P<0.05. Data analyses were performed using SPSS (version 29.0; IBM Corp., Armonk, NY, USA) and R software (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria).
-
Between 2008 and 2024, 37,034 individuals with heterosexually transmitted HIV were reported in Liangshan, with 16,326 cases reported before the comprehensive strategy implementation and 20,708 afterward. The number of reported cases peaked at 6,622 in the first year following implementation, then declined annually by 22% (
Supplementary Figure S1 ). Most cases involved females, individuals aged 30–44 years, and residents of key counties. Compared to the pre-implementation period, the post-implementation period showed a slight increase in the proportion of cases in the 30–44 year age group, while decreases were observed among females and residents of key counties. Concurrently, significant increases occurred in the proportion of cases among individuals aged over 45 years and those with a baseline CD4 count <200 (Supplementary Table S1 ).During the study period, 7,302 deaths were recorded (19.7% of total cases), including 1,084 AIDS-related deaths (2.9% of total cases). Cox regression analysis identified not receiving ART as the most significant risk factor for mortality (adjusted HR: 17.74, Table 1). After controlling for demographics and excluding ART status as a modifiable factor, the comprehensive strategy was independently associated with a 35% reduction in overall mortality (adjusted HR: 0.65, 95% CI: 0.64, 0.69) and a 60% reduction in AIDS-related mortality (adjusted HR: 0.40, 95% CI: 0.34, 0.46).
Variables Total
(n)Death
(n)Follow-up time
(person-months)Univariate analysis Multivariate analysis HR (95% CI) P HR (95% CI) P Gender Female 18,926 2,994 168.7 1 1 Male 18,108 4,308 146.9 1.69 (1.62, 1.78) <0.001 1.46 (1.38, 1.53) <0.001 Age (years) 15–29 12,710 1,860 172.2 1 1 30–44 15,498 3,027 158.6 1.55 (1.46, 1.64) <0.001 1.59 (1.49, 1.69) <0.001 45–59 6,093 1,205 148.2 1.92 (1.78, 2.06) <0.001 2.27 (2.09, 2.46) <0.001 ≥60 2,733 1,210 94.3 4.65 (4.32, 5.00) <0.001 3.87 (3.53, 4.24) <0.001 Occupation Farmers 31,803 6,130 159.3 0.87 (0.82, 0.93) <0.001 1.19 (1.12, 1.28) <0.001 Others 5,231 1,172 153.5 1 1 Education Illiterate 17,614 3,689 157.5 1.24 (1.16, 1.33) <0.001 1.16 (1.07, 1.25) <0.001 Primary School 13,207 2,605 156.5 1.23 (1.15, 1.33) <0.001 1.17 (1.08,1.26) <0.001 Junior High and Above 6,213 1,008 165.6 1 1 Disease stage HIV 30,745 5,652 160.8 1 1 AIDS 6,289 1,650 147.0 1.41 (1.34, 1.49) <0.001 1.40 (1.30, 1.51) <0.001 Baseline CD4 count (cell/μL)* <200 5,802 1,409 146.9 1 1 200–349 10,336 1,488 167.0 0.53 (0.49, 0.57) <0.001 0.71 (0.65, 0.77) <0.001 350–499 9,050 1,290 170.1 0.48 (0.44, 0.51) <0.001 0.65 (0.59, 0.71) <0.001 ≥500 9,855 1,300 173.5 0.43 (0.40, 0.46) <0.001 0.58 (0.53, 0.63) <0.001 Missing 1,991 1,815 13.4 16.36 (15.22, 17.59) <0.001 2.28 (2.06, 2.52) <0.001 Current ART status No 3,263 3,196 22.4 25.12 (23.91, 26.40) <0.001 17.74 (16.54, 19.02) <0.001 Yes 33,771 4,106 173.8 1 1 Study phase Pre-Action Plan 16,326 5,062 150.5 1 1 Post-Action Plan 20,708 2,240 76.0 0.54 (0.51, 0.57) <0.001 1.13 (1.06, 1.19) <0.001 * The initial CD4 count at diagnosis. Action Plan refers to the comprehensive strategy implemented in 2018.
Abbreviation: ART=antiretroviral therapy; CI=confidence interval; HR=hazard ratios; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome.Table 1. Factors associated with mortality among heterosexually transmitted HIV-infected individuals in Liangshan, 2008 to 2024 (n=37,034).
-
From 2008 to 2024, treatment coverage demonstrated a significant upward trend (P<0.05), with a compound annual growth rate (CAGR) of 34.79%. The median annual coverage increased from 38.46% (IQR: 13.03–56.16) with a CAGR of 62.16% pre-implementation to 97.61% (IQR: 95.17–99.39) with a CAGR of 1.88% post-implementation. In key counties, ART coverage improved from 54.74% (IQR: 48.66–59.54) to 95.63% (IQR: 92.52–97.91), while in non-key counties it increased from 57.36% (IQR: 50.02–63.22) to 96.40% (IQR: 90.17–97.99) (Figure 1). Segmented linear regression revealed an immediate 21.62% increase (95% CI: 16.63, 26.62) in treatment coverage during the first implementation year, followed by a steady annual increase of 1.48%. By 2024, treatment coverage reached 99.68%, slightly exceeding the expected level (8.95%, 95% CI: −4.12, 22.02).
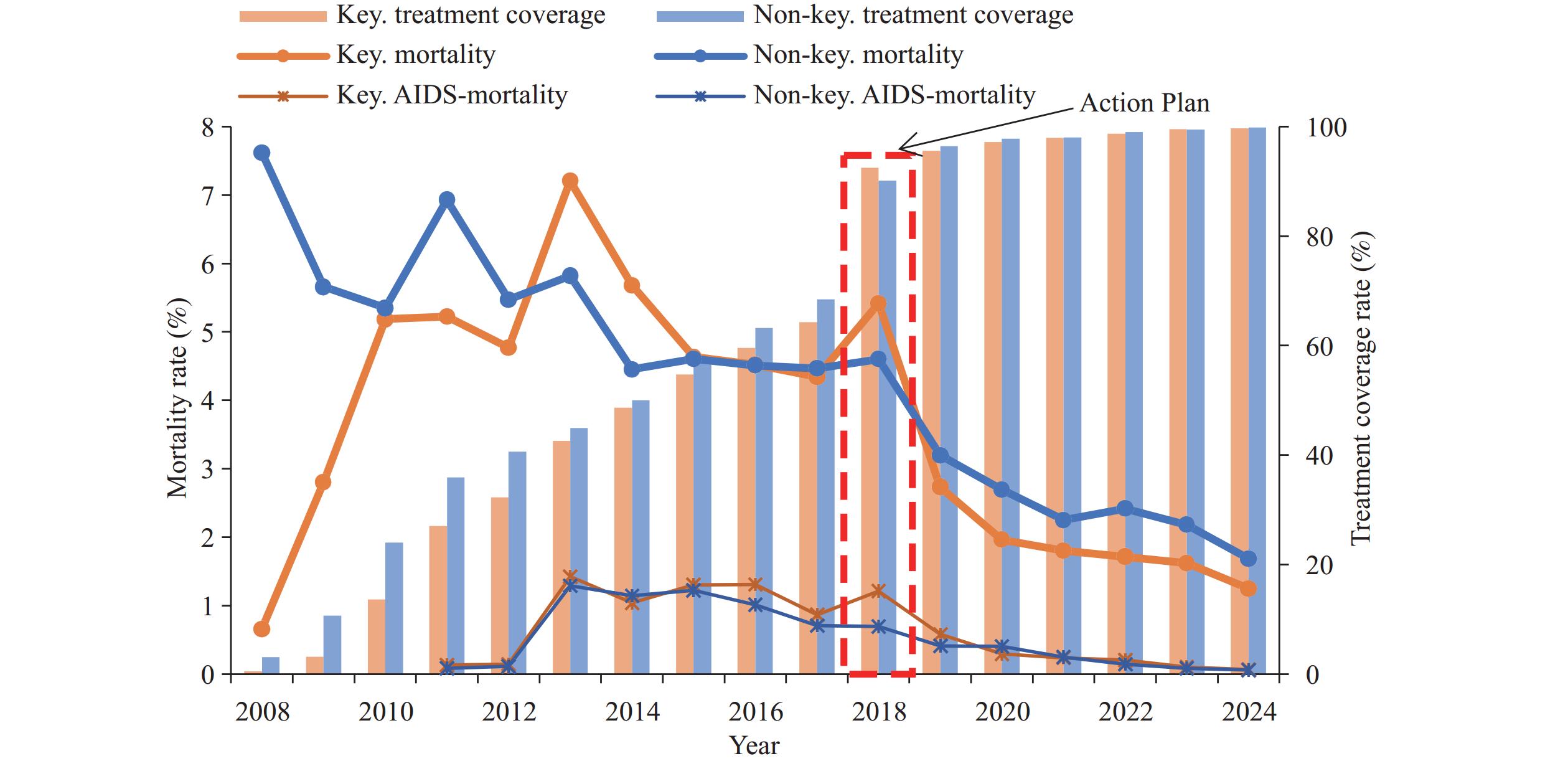 Figure 1.
Figure 1.Trends in treatment coverage and mortality among heterosexually transmitted HIV-infected individuals in Liangshan Prefecture, 2008–2024. Action Plan refers to the comprehensive strategy implemented in 2018.
Abbreviation: AIDS-mortality=acquired immunodeficiency syndrome-related mortality; Key.=Key counties (Butuo, Zhaojue, Yuexi, and Meigu); Non-key.=Non-key counties (all counties in Liangshan except for key counties).Concurrently, overall mortality exhibited a significant downward trend (P<0.05), decreasing from a median of 4.83% (IQR: 4.15–5.37) before implementation to 2.06% (IQR: 1.90–2.95) afterward. Key counties demonstrated a mortality reduction from 4.64% (IQR: 4.52–5.68) pre-implementation to 2.73% (IQR: 1.80–5.42) post-implementation, while non-key counties showed a decrease from 4.51% (IQR: 4.47–4.61) to 3.20% (IQR: 2.42–4.60) (Figure 1). AIDS-related mortality similarly declined significantly (P<0.05) from 1.09% (IQR: 0.13–1.27) pre-implementation to 0.24% (IQR: 0.09–0.50) post-implementation (Figure 2). Although no immediate change was detected in 2018, segmented linear regression showed that mortality decreased by 0.47% annually following the intervention (95% CI: −0.73, −0.21). By 2024, mortality was 4.89% lower than expected (95% CI: −8.02, −1.75), corresponding to an 81.2% reduction (Table 2 and Figure 2).
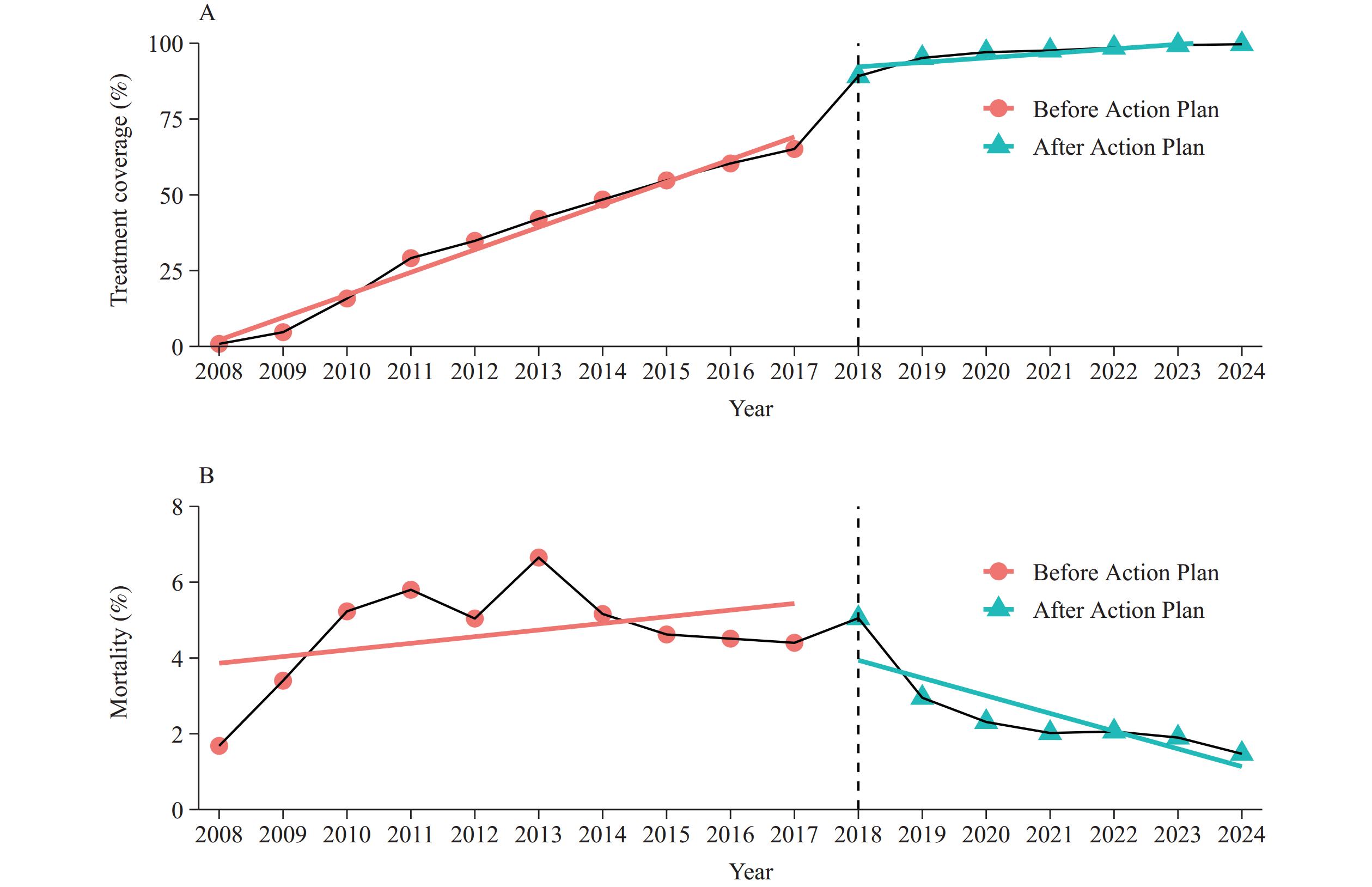 Figure 2.
Figure 2.Segmented linear regression models of outcome indicators for heterosexual HIV-infected individuals in Liangshan Prefecture, 2008–2024. The solid pink and blue lines represent the model-fitted lines. Action Plan refers to the comprehensive strategy implemented in 2018. (A) Treatment coverage; (B) Mortality.
Note: Treatment coverage means treatment coverage rate per year; mortality calculated by all-cause mortality rate per year.Variables Level change at
Action PlanLevel change in
2024Trend before
Action PlanTrend after
Action PlanTreatment coverage rate Total 21.62 (16.63, 26.62) 8.95 (−4.12, 22.02) 7.44 (6.80, 8.09) 1.48 (0.73, 2.24) Gender Male 21.97 (17.06, 26.88) 10.17 (−1.87, 22.21) 7.26 (6.62, 7.90) 1.72 (0.96, 2.49) Female 21.39 (16.28, 26.51) 8.01 (−5.90, 21.91) 7.59 (6.93, 8.25) 1.29 (0.54, 2.04) Region Non-key counties 20.31 (15.29, 25.33) 8.01 (−4.81, 20.83) 7.09 (6.31, 7.87) 1.30 (0.53, 2.07) Key counties 24.18 (20.27, 28.09) 10.50 (−4.16, 25.15) 7.57 (6.82, 8.33) 1.11 (0.75, 1.46) Disease stage HIV 32.50 (26.85, 38.14) 22.22 (12.28, 32.16) 6.73 (5.97, 7.49) 1.94 (1.23, 2.66) AIDS 3.61 (−5.26, 12.47) −5.31 (−19.77, 9.15) 5.06 (2.98, 7.13) 0.87 (0.42, 1.32) Mortality rate Total −1.03 (−2.85, 0.79) −4.89 (−8.02, −1.75) 0.18 (−0.11, 0.46) −0.47 (−0.73, −0.21) Gender Male −1.08 (−2.78, 0.63) −5.22 (−7.84, −2.61) 0.18 (−0.09, 0.45) −0.51 (−0.71, −0.32) Female −0.99 (−3.08, 1.10) −4.58 (−8.05, −1.11) 0.16 (−0.16, 0.47) −0.44 (−0.74, −0.13) Region Non-key counties −0.62 (−1.84, 0.60) −2.88 (−5.23, −0.52) −0.02 (−0.29, 0.26) −0.39 (−0.53, −0.26) Key counties −1.27 (−4.04, 1.50) −6.16 (−9.67, −2.66) 0.28 (−0.11, 0.67) −0.54 (−0.85, −0.22) Disease stage HIV −1.02 (−3.12, 1.08) −3.83 (−6.32, −1.35) 0.04 (−0.24, 0.33) −0.42 (−0.69, −0.16) AIDS 0.04 (−2.01, 2.09) −2.31 (−6.47, 1.85) −0.13 (−0.61, 0.35) −0.52 (−0.82, −0.23) ART No 9.50 (0.65, 18.35) 12.31 (6.59, 18.02) 0.51 (0.22, 0.79) 0.98 (−0.99, 2.94) Yes −0.90 (−1.86, 0.07) −2.69 (−4.71, −0.67) 0.14 (−0.15, 0.43) −0.16 (−0.22, −0.10) Note: Data are rate (95% CI) or trend (95% CI). Key counties: Butuo, Zhaojue, Yuexi, and Meigu. Non-key counties: all counties in Liangshan except for key counties. Action Plan: the comprehensive strategy was implemented in 2018.
Abbreviation: ART=antiretroviral therapy; CI=confidence interval; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome.Table 2. Segmented linear regression models of the impact of comprehensive strategy on treatment coverage and mortality among heterosexually transmitted HIV-infected individuals in Liangshan from 2008 to 2024.
-
Subgroup analysis revealed disparities in treatment coverage improvements and mortality reductions across gender, region, and disease stage. Greater improvements in both outcomes occurred among males, patients in key counties, and those diagnosed at the HIV infection stage. Among AIDS patients, the immediate increase in treatment coverage was small and insignificant (3.61, 95% CI: −5.26, 12.47), followed by a modest annual increase of 0.87%. The mortality of AIDS patients showed an insignificant immediate change (0.04%, 95% CI: −2.01, 2.09), but declined significantly thereafter. By 2024, mortality among those receiving ART was 2.69% (95% CI: −4.71, −0.67) lower than expected, whereas mortality among patients not receiving ART rose immediately after implementation (9.50, 95% CI: 0.65, 18.35) and remained elevated compared to expected levels (Table 2 and Figure 2).
-
This study provides compelling evidence that the comprehensive strategy substantially accelerated progress towards universal ART coverage and produced a marked, sustained reduction in mortality among heterosexually transmitted HIV-infected individuals in Liangshan. These findings align with studies from other high HIV prevalence settings (10–11) and underscore the value of integrating routine HIV services with locally tailored governance, real-time cascade tracking, and poverty-reduction initiatives in high-burden, resource-constrained settings.
A notable achievement is the remarkable increase in treatment coverage following implementation of the comprehensive strategy, approaching universal coverage. This achievement exceeds national and international benchmarks for the treat-all policy (12–14). The near-universal uptake resulted from several mutually reinforcing measures implemented under Liangshan’s comprehensive strategy, including universal HIV testing integrated into health checkups, real-time cascade tracking of each patient, and two complementary service governance models — “Three Lines and One Network Base” and “1+M+N” — that mobilize multisectoral accountability down to the grassroots community level. These measures shortened the interval from diagnosis to treatment, enhanced ART retention, and facilitated differentiated care, thereby maximizing the population-level preventive and therapeutic benefits of ART.
Our findings further confirmed the role of ART scale-up, demonstrating that Liangshan’s comprehensive strategy primarily reduced mortality risk through ART expansion, with this effect being particularly pronounced in reducing the risk of AIDS-related deaths. The magnitude of mortality decline observed in Liangshan exceeds that reported from universal test and treat programs in other settings, where reductions have ranged from 10% to 50% (5,11–12). This might be attributed to Liangshan’s rapid escalation in ART coverage from 65% in 2017 to 95% within three years.
Subgroup analysis revealed larger improvements in treatment coverage and mortality among males, residents of key counties, and individuals at HIV infection stage. For males, who typically present later, exhibit poorer ART adherence, and experience higher mortality than females (4,13), the tailored peer-navigation, workplace outreach, and culturally adapted counseling embedded in the comprehensive strategy may have reduced gender-related barriers to care. The greater improvements in both outcomes and a lower proportion of cases in key counties underscore the amplifying effect of geographic prioritization and concentrated resource inputs. The transient mortality increase observed immediately after implementation, particularly among patients at AIDS stage and not receiving ART, was attributable to the surge in case detection that accompanied expanded screening in 2018 (3). Many newly diagnosed patients had advanced disease stage and therefore faced high short-term mortality despite rapid linkage to ART (15). Sustained decreases in both all-cause mortality and AIDS-related mortality over subsequent years suggest that early treatment initiation and improved care management rapidly offset this initial increase.
Notably, expanded screening also increased case detection among older patients, a demographic shift partially attributable to prolonged HIV transmission dynamics and delayed diagnosis, but also suggesting unmet prevention needs in aging populations. For AIDS patients, our findings reinforce the necessity of integrated management protocols encompassing uninterrupted ART delivery, psychosocial support, and multidisciplinary chronic care integration to mitigate mortality risks. The program’s success extends prior evidence by demonstrating that scalable HIV response models can yield equivalent benefits in an ethnically diverse region with historically limited health infrastructure. Coupling HIV prevention with poverty alleviation initiatives likely enhanced health gains by addressing structural determinants that impede sustained engagement in care. To consolidate gains, Liangshan should prioritize earlier diagnosis through intensified outreach in non-key counties, expand immediate ART initiation, and develop age- and gender-specific adherence interventions. Implementation science studies should delineate which components of the comprehensive strategy are most cost-effective and transferable to other regions.
This study has several limitations. First, concurrent national public health initiatives may have contributed to the observed trends, although our ITS modeling mitigated this risk by accounting for pre-intervention trajectories. Second, potential underreporting and misclassification of deaths, particularly before the implementation of the comprehensive strategy, could bias the actual impact of the strategy on mortality (3). Last, our findings may not generalize to settings without comparable political commitment or community governance structures.
In conclusion, our results demonstrate that the comprehensive strategy in Liangshan, as a data-driven, multisectoral approach, can achieve near-universal ART coverage and an unprecedented reduction in mortality among heterosexually transmitted HIV-infected individuals. Scaling and adapting this comprehensive model could accelerate progress towards the 95-95-95 targets and the broader goals of the Sustainable Development Agenda in similar high-burden regions.
-
Approved by the Institutional Review Board of the National Center for AIDS/STD Control and Prevention, Chinese CDC (X140121318), with informed consent waived due to the retrospective nature of aggregated data.
HTML
Data Source and Comprehensive Strategy
Outcomes and Survival Analysis
Interrupted Time Series (ITS) Analysis

Software
Treatment Coverage and Mortality
Subgroup Analysis
| Citation: |

|