
 Download:
Download:




HTML
-
Introduction: The Global Activity Limitation Indicator (GALI) offers a simpler and more efficient approach to measuring disability compared to traditional instruments. While GALI’s reliability has been validated across different regions, its effectiveness is influenced by cultural differences. This study aims to assess GALI’s applicability in China and examine the relationships between GALI and mortality rates, as well as health human resources.
Methods: We analyzed data from the Resident Health and Health Service Monitoring survey, a nationally representative cross-sectional survey conducted annually from 2019−2022. Multivariate and multinomial logistic regression models were employed to estimate odds ratios and activity limitation probabilities. Mixed effect models were used to explore county-level associations.
Results: GALI demonstrated high response rates and reliability throughout the survey period. Significant associations were observed between GALI and traditional disability instruments, as well as disease prevalence. At the county level, GALI showed positive associations with mortality rates and negative associations with the number of physicians per thousand residents.
Conclusions: GALI represents a reliable measure of disability for the Chinese mainland population and could serve as a potential predictor for cardiovascular diseases, respiratory system diseases, and unintentional injuries. Our findings suggest that increasing the number of physicians per thousand residents may be associated with reduced activity limitation, though additional research is needed to validate this relationship.
-
As societies worldwide experience aging populations, increasing attention is being paid to monitoring disability. Healthy life expectancy (HLE) is a crucial indicator that goes beyond life expectancy (LE) to measure both mortality and quality of life (QoL) within a population. QoL is closely linked to disease burden and disability, which underscores the need for culturally adaptable tools to assess health outcomes. The concept of disability can vary depending on different definitions of health (1). Different from the health-adjusted life expectancy (HALE) from the Global Burden of Diseases 2021 (GBD2021) that applied the disease/impairments to measure health, the Global Activity Limitation Indicator (GALI), a convenient and simple one-item survey tool to measure disability, has been validated and applied for HLE estimation in many countries (2–5). GALI was developed by Euro-REVES, and has been proven to be correlated with other traditional disability instruments, socioeconomic characteristics, and comorbidity in the European population (4,6–10). However, the applicability of GALI remains unvalidated in China, which represents a critical gap given the country’s rapidly aging demographics, unique cultural perceptions of disability, and urgent policy mandates (9). Specifically, the Healthy China 2030 Planning Outline, the Healthy China Action (2019−2023)and the 14th Five-Year National Health Plan all prioritize increasing HLE as one of their key tasks, aiming to improve the HLE in proportion to LE. Despite these efforts, an official HLE framework with a standardized definition of disability is still lacking in China, which hinders progress toward these national targets.
Using data from the nationally representative Resident Health and Health Service Monitoring (RHHSM) survey covering approximately 100,000 residents annually across diverse regions, we aim to evaluate the applicability of GALI in China by comparing it with traditional disability instruments at the individual level. Further, we propose to examine the relationship between GALI and disease mortality, as well as health human resources at the county level, in order to reveal the factors that could be associated with reduced activity limitation.
GALI, traditional disability instruments, and demographic information were obtained from the RHHSM. The RHHSM survey is a nationwide survey conducted by the Center for Health Statistics and Information, National Health Commission of China (CHSI). Detailed introduction to RHHSM can be found in Supplementary Methods.
The response variable in our research was GALI, which measured the extent to which individuals were limited in their activities due to a health problem over the past six months. Participants were asked a simple question: “To what extent have you been limited because of a health problem in activities people usually do?” We categorized any response indicating limitation (both severely and not severely) as disability (11). Traditional disability instruments included activities of daily living (ADL) (12), instrumental ADL (iADL) (13), EuroQol five dimensions questionnaire (EQ5D), and EQ5D-visual analoguescale (EQ5D-VAS) (14). Individuals aged over 8 were required to complete the EQ5D and EQ5D-VAS, and those over 60 were required to complete the ADL and iADL. Those who reported any difficulties in all six questions in ADL and iADL were classified as having a disability. For EQ5D, the model MULT8r was used to generate population norms for the EQ5D-5L questionnaire, utilizing coefficients fitted by 8 multiplicative models with a random intercept (15). The EQ5D-VAS was a self-report question that allowed respondents to rate their general health state on a visual analogue scale ranging from 0 to 100, with 0 indicating the worst imaginable health state and 100 indicating the best imaginable health state.
The total household resident income and the number of household resident population were collected during the survey, and individual income was calculated by dividing the total registered household resident income by the number of registered household resident population. Income was transformed to logarithmic form in the model. Disease prevalence was determined based on self-reported questionnaires in the survey. Respondents were asked to report any existing conditions, including hypertension, diabetes, chronic respiratory diseases, acute respiratory infections, acute gastroenteritis, and other diseases.
At the county level, each individual’s responses to the GALI questionnaire were aggregated by age and county to obtain county-level GALI measurements. The county-level GALI was then analyzed in relation to county-level mortality rates and the number of physicians per thousand residents. Population counts by age in each county were obtained from the National Bureau of Statistics (NBS), which were estimated using the Chinese Seventh National Population Census. Information on cause-specific mortality from 2019 to 2021 was obtained from the China Cause of Death Reporting System (CDRS), which served as the official platform for reporting individual-level deaths in real-time (16). Healthcare human resources were sourced from the National Hospital Annual Report (HAR) Database in China (17). We estimated the number of physicians per thousand residents by combining this data with the population size of each county.
Cronbach’s alpha was employed to assess the reliability of the questionnaires used in the survey. At the individual level, Spearman correlation coefficients were utilized to investigate relationships between questionnaires, health-related outcomes, and socioeconomic characteristics. Multivariate logistic regression models were used to examine odds ratios between GALI and other variables. To predict the probability of GALI responses based on different EQ-5D and EQ-5D-VAS values, multinomial logistic regression models were applied. At the county level, we assessed associations between GALI, cause-specific mortality rates, and healthcare human resources using mixed effect models. All P values were calculated using a two-tailed approach, with statistical significance defined as P<0.05. All statistical analyses were performed using R version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria).
The RHHSM survey in 2022 included 93,189 participants. Only 3 individuals did not respond to the GALI questionnaire, resulting in a nearly 100% response rate. Among 87,281 participants over 8 years old, 99.5% completed both the EQ5D and EQ5D-VAS questionnaires. Similarly, among 29,490 participants over 60 years old, the completion rate for ADL and iADL questionnaires was 96.6%. The Cronbach’s alpha for the survey was 0.962. Regarding demographic characteristics, respondents reporting no activity limitations in GALI were generally younger, had higher education levels, resided in urban areas, and had higher incomes. They also had fewer diseases, lower scores on EQ5D and EQ5D-VAS questionnaires, and fewer limitations in ADL and iADL, indicating better overall health. Detailed baseline characteristics stratified by GALI response are presented in Table 1. Correlation analysis revealed that GALI was associated with most demographic characteristics and all four other measurements (
Supplementary Table S1 ). Multinomial logistic regression models showed that as EQ5D and EQ5D-VAS scores increased, the predicted probability of having no limitations also increased, while the probability of severe limitations decreased significantly (Figure 1A and 1B). Further stratification by ADL and iADL limitations demonstrated clear dose-response relationships between the number of limitations in EQ5D questionnaires (Figure 1C) or GALI limitation levels and disease prevalence (Figure 1D). Additionally, GALI was significantly associated with injuries (Supplementary Figure S1 ).Characteristics No, not limited Yes, limited Yes, strongly limited P Sample size 84,648 6,688 1,850 Age [mean (SD)] 44.52 (21.98) 64.37 (15.72) 66.55 (17.14) <0.001 Female (%) 42,607 (50.30) 3,595 (53.80) 946 (51.10) <0.001 High school or above (%) 25,197 (29.80) 746 (11.20) 202 (10.90) <0.001 Rural area (%) 40,297 (47.60) 3,950 (59.10) 1,004 (54.30) <0.001 Income [mean (SD)] 24,774.26 (35,327.64) 18,375.48 (18,830.42) 21,404.49 (54,957.85) <0.001 Prevalence (%) <0.001 Disease-free 60,421 (71.40) 1,632 (24.40) 323 (17.50) One disease 17,313 (20.50) 2,406 (36.00) 607 (32.80) Two or more diseases 6,914 (8.20) 2,650 (39.60) 920 (49.70) EQ5D-VAS [mean (SD)] 85.70 (11.85) 67.56 (14.74) 50.47 (19.63) <0.001 EQ5D [mean (SD)] 0.99 (0.04) 0.85 (0.15) 0.37 (0.40) <0.001 ADL limited (%) 741 (3.30) 1,724 (38.80) 1,105 (85.60) <0.001 iADL limited (%) 2,396 (10.50) 2,602 (58.60) 1,200 (93.00) <0.001 Note: EQ5D-VAS and EQ5D were used to measure disability among the population aged over 8, while ADL and iADL measured those aged over 60.
Abbreviation: GALI=global activity limitation indicator; ADL=activities of daily living; iADL=instrumental activities of daily living; EQ5D=EuroQol five dimensions questionnaire; EQ5D-VAS=EuroQol five dimensions questionnaire-visual analogue scale; SD=standard deviation.Table 1. Characteristics of population stratified by GALI responses.
 Figure 1.
Figure 1.Association between GALI and ADL/iADL stratified by disease prevalence status. (A) and (B) show the association between GALI responses and EQ5D/EQ5D-VAS scores. (C) illustrates the association between GALI and the 5 questions of the EQ5D questionnaire, where 1 indicated complete health and 5 indicated the opposite. (D) demonstrated the association between GALI and disease prevalence stratified ADL limitation.
Note: For (A) and (B), the probability of GALI responses was estimated using multinomial logistic regression adjusted for age, gender, race, education level, rural area, and income.
Abbreviation: GALI=global activity limitation indicator; ADL=activities of daily living; iADL=instrumental activities of daily living; EQ5D=EuroQol five dimensions questionnaire; EQ5D-VAS=EuroQol five dimensions questionnaire-visual analogue scale.
Our investigation revealed that GALI showed consistent associations with activity limitations across all dimensions of the EQ5D questionnaire, particularly in relation to depression. When stratifying the results according to ADL/iADL limitation status, we found that individuals with depression were more likely to report limitations when measured by GALI, and this association was even stronger among those without ADL/iADL limitations (P for interaction for both ADL and iADL <0.001,
Supplementary Figure S2 ). When incorporating GALI into the prediction model alongside covariates such as gender, minority status, urban residence, education, and income, we observed a 1.88% improvement in prediction accuracy for self-reported diseases (P<0.001,Supplementary Figure S3A ).We conducted an analysis of 2019–2021 data on activity limitation rates measured by GALI, EQ5D, and ADL at the county level. We found that at both individual and county levels, activity limitation proportions decreased with increasing income levels or GDP (
Supplementary Figure S3B–C ). Further, we explored associations among these limitation rates, county-level mortality, and the number of physicians per thousand residents. Our findings revealed that counties with higher limitation rates tended to have higher mortality rates (Figure 2A). Specifically, the association between GALI and mortality rates related to cardiovascular diseases, respiratory system diseases, and unintentional injuries was particularly pronounced (Figure 2B–D). The association between GALI and mortality rates for other diseases is presented inSupplementary Table S2 . Additionally, our research indicated that a higher number of physicians per thousand residents was associated with lower activity limitation rates (Figure 2E).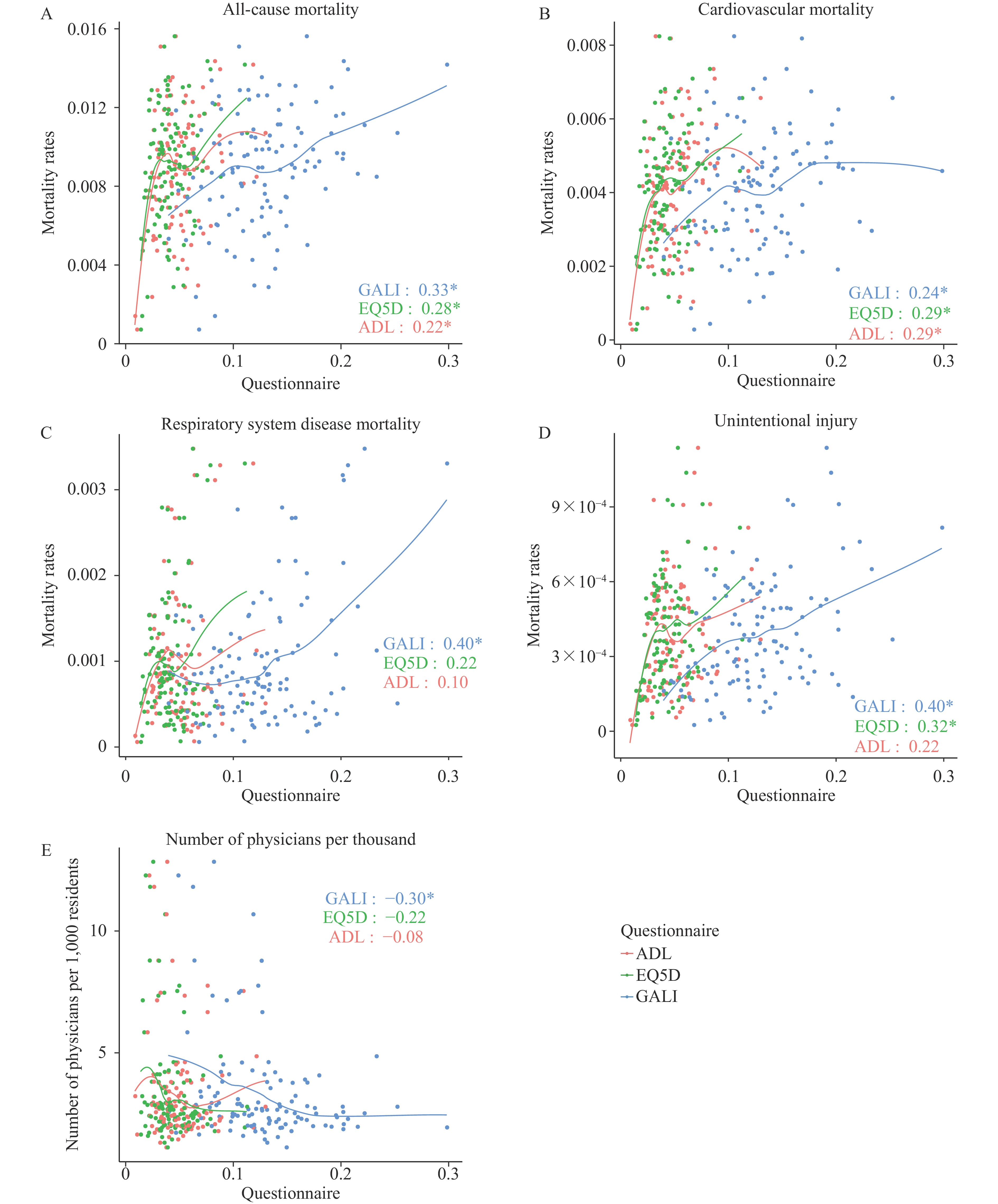 Figure 2.
Figure 2.Correlation between limitation measurements and mortality or healthcare human resources at the county level. (A) demonstrates the association between 3 questionnaires (GALI, EQ5D, and ADL) and all-cause mortality rates. (B–D) show the association between the questionnaires and mortality rates of cardiovascular diseases, respiratory system diseases, and unintentional injury, respectively. (E) indicates the association between the questionnaires and physician density.
Note: Pearson correlation was used to calculate the correlation between measurements and county-level mortality rate or healthcare resources. In panels (A−E), the horizontal axis represents the measured limitation, and the vertical axis represents the mortality rate in panels (A–D), and the number of physicians per 1,000 residents in panel E.
Abbreviation: GALI=global activity limitation indicator; ADL=activities of daily living; iADL=instrumental activities of daily living; EQ5D=EuroQol five dimensions questionnaire; EQ5D-VAS=EuroQol five dimensions questionnaire-visual analogue scale.
-
This study presented the first comprehensive evaluation of the GALI in the Chinese population using a nationally representative survey. Our findings demonstrated that GALI achieved the highest response rate among all disability assessment instruments due to its simplicity and convenience, indicating its reliability as a population-wide disability measure. Importantly, we observed strong correlations between GALI and traditional disability instruments, including ADL, iADL, EQ5D, and EQ5D-VAS. Furthermore, GALI showed potential as a predictor of health outcomes related to depression and chronic disease prevalence at the individual level. At the county level, reduced mortality rates and increased physician density were associated with lower activity limitation rates.
Our study identified a significant predictive role of the GALI scale in mental health assessment. Individuals with more pronounced depressive symptoms were more likely to report limitations on GALI, particularly among those without ADL/iADL limitations. This suggests that GALI may detect depression-related symptoms in populations without apparent physical activity limitations. While previous research has demonstrated GALI’s potential in predicting mortality in European populations (18-19), we extended these findings to disease prevalence. When incorporated into predictive models alongside demographic factors such as gender, urban status, education, and income, GALI improved the prediction accuracy of self-reported diseases by 1.88%. These findings highlight GALI’s multifaceted utility in comprehensive health assessment.
We analyzed county-level activity limitation rates measured by GALI, EQ5D, and ADL from 2019 to 2021, exploring associations with county-level mortality and physician density — relationships rarely examined in previous studies due to limited sample sizes. Our results revealed that counties with higher activity limitation rates exhibited elevated mortality rates. Particularly noteworthy was the significant association between GALI and mortality rates related to unintentional injuries, which was stronger than associations with other measurements. Additionally, we identified a negative correlation between GALI and physician density (physicians per thousand residents). While previous European studies were constrained by limited population sizes and focused primarily on individual-level associations. China’s large population and remarkable diversity enabled us to explore regional disparities in activity limitation at the county level. These findings have significant implications for health policy development and healthcare resource allocation.
Several limitations should be acknowledged in this study. As a retrospective investigation, biases and confounding factors related to survey methodology may have influenced our results. To ensure data quality, the RHHSM implemented a quality review within one month after survey completion, focusing on eight objective questions and involving 5% of respondents. The 2022 review demonstrated a consistency rate exceeding 95%. It should be noted that our findings are specifically generalizable to the Chinese population.
To our knowledge, this is the first study in Chinese mainland investigating the population applicability of GALI. By examining the spectrum of associations between GALI and health-related factors at the individual level, our research contributes to the current understanding of healthy life expectancy estimation in China and provides evidence supporting GALI’s use as a health indicator for Chinese populations. Our county-level findings suggest that increasing healthcare resources, particularly physician density, could be an important consideration in policy initiatives aimed at enhancing healthy life expectancy in China. Future research should include real-world evidence and intervention studies to validate these results.
-
This survey was approved by the institutional review board of the Chinese National Bureau of Statistics, and the ethical approval was granted by the medical ethical review committee of the Southern University of Science and Technology (Approval No. 20240210). All participants provided oral consent prior to the interview.
| Citation: |

|