
 Download:
Download:




-
Introduction: Mushroom poisoning remains a significant food safety concern in China, particularly in southern regions like Guangzhou City, Guangdong Province. Accidental consumption of toxic mushrooms often leads to severe health outcomes, including gastroenteritis, liver failure, renal failure, and psycho-neurological disorders. This study analyzes cases of mushroom poisoning admitted to the Guangzhou Twelfth People’s Hospital between 2016 and 2023, focusing on mushroom species, poisoning types, clinical trends, treatment outcomes, and diagnostic challenges.
Methods: This retrospective study included 112 patients with confirmed mushroom poisoning. Demographic, clinical, and epidemiological data were extracted from medical records, including age, gender, type of mushroom consumed, latency period, symptoms, and treatment outcomes. Statistical analyses examined the relationships between latency period, symptom severity, and hospitalization outcomes. Identification of mushroom species and toxicity classification was supported by the HOPE6 and TALK Chinese clinical assessment protocols.
Results: The cohort had a median age of 45 years, with a male-to-female ratio of 1.4:1. May and June were peak months for incidents. Four poisoning types were identified: gastroenteritis (62.5%), liver failure (25.0%), psycho-neurological disorders (9.8%), and renal failure (2.7%). Patients with delayed symptom onset (median latency of 10 hours) experienced more severe complications and prolonged hospital stays. Acute liver failure accounted for all 12 fatalities, predominantly linked to Amanita species. Prompt gastric lavage correlated with lower mortality in gastroenteritis and psycho-neurological cases, while blood purification showed efficacy for renal and liver failure patients.
Discussion: The study underscores the critical role of latency period and initial clinical assessment in determining treatment outcomes for mushroom poisoning. Enhanced diagnostic capabilities and multidisciplinary approaches are essential to reduce mortality. Future efforts should focus on improving mushroom identification protocols and expanding the application of standardized clinical assessment tools like HOPE6 and TALK
1 . -
Mushroom poisoning has emerged as a significant food safety concern with a notable increase in incidence over the past four years in China (1). Guangzhou, the capital city of Guangdong Province, has recorded a significant number of mushroom poisoning cases annually. These incidents typically result from accidental consumption and can occur throughout the year (2). This retrospective observational study aimed to investigate the diagnosis, prognosis, and outcomes of mushroom poisoning. We analyzed 112 cases admitted to Guangzhou Twelfth People’s Hospital from 2016 to 2023, providing key epidemiological data for Southern China. The study employed the HOPE6 (
Supplementary Table S1 ) and TALK (Supplementary Table S2 ) Chinese clinical assessment systems to assist with diagnosis and prognosis in clinical evaluations (2). Four types of mushroom poisoning were identified based on clinical consultation and mycological testing (2–3). Acute liver failure contributed to the most severe outcomes of mushroom poisoning. Nine poisonous mushroom species were identified, with Amanita exitialis (A. exitialis), Amanita rimosa (A. rimosa), and Amanita fuligineoides (A. fuligineoides) being the major species causing acute liver injury and leading to the highest mortality rates in the cohort. Our analysis revealed significant gaps in early diagnosis and initial treatment decision-making, particularly in cases of acute liver failure. Future efforts should focus on expanding collaboration to validate the HOPE6 and TALK system and improving prognostic accuracy.In this study, retrospective data from 2016 to 2023 were systematically reviewed from the Guangzhou Twelfth People’s Hospital. Patients of all ages with a history of suspected poisonous mushroom ingestion, especially wild or self-collected specimens, and exhibiting symptoms consistent with known poisoning syndromes after a latency period were included. Cases without symptoms attributable to mushroom poisoning or with hospitalization stays less than 3 days were excluded.
Poisonous mushroom species and poisoning types were systematically classified. Species identification employed both morphological and molecular methods. Morphological identification referenced literature including the “Atlas of Chinese Macrofungal Resources” and “Poisonous Mushrooms: Recognition and Poisoning Treatment” (4-5). Macro- and micro-morphological observations were recorded, with tissues stained with 5% Potassium Hydroxide (KOH) and 1% aqueous Congo red. DNA extraction was performed using a commercial kit, and primer pairs ITS5/ITS4 were used for sequencing (6).
Clinically, mushroom poisoning was categorized into four types based on syndromic diagnosis (7). Treatment strategies were determined by symptomatology, latency period, and pathological findings (2–3). Gastric lavage and activated charcoal were administered initially within 6 hours of ingestion. Blood purification was reserved for severe cases involving acute liver or kidney injury. Liver transplantation is an effective treatment for liver failure, with identified survival rates of up to 80% (8). In our cohort, liver transplantation was administered as part of intensive care in select cases.
All statistical analyses were conducted using R (version 4.2.3, R Foundation, Vienna, Austria). For patients with different types of mushroom poisoning, continuous data were presented as the median and interquartile range (IQR), while categorical data were presented as numbers and percentages. A scatter plot and Pearson correlation analysis were performed to explore the relationship between latency period and hospitalization length among all patients with mushroom poisoning. Multivariate logistic regression was used to examine the association between latency period and fatal mushroom poisoning. The latency period of various toxic mushroom species was presented as the median and range, and mortality rates were calculated for each species. Statistical significance was set at P<0.05 (two-tailed).
A total of 112 patients were included in the present study (Table 1), comprising 66 males (58.93%) and 46 females (41.07%), with a median age of 45 years. Incidence of mushroom poisoning peaked in May and June, with over 30 cases recorded in May. Four types of mushroom poisoning were identified: gastroenteritis (n=70), acute liver failure (n=28), acute kidney injury (n=3), and psycho-neurological disorder (n=11). The median hospitalization duration was 3.0 days, and the median latency period was 2.0 hours. Gastric lavage was performed in 65.18% of cases (n=73), and 26.79% underwent blood purification (n=30). Among all cases, 37 (33.04%) were recognized as fatal mushroom poisoning, with 75.68% (28/37) associated with acute liver failure. The overall inpatient mortality was 10.71% (n=12), with all deaths attributable to liver failure complications.
Variables Types of mushroom poisoning All patients
(N=112)Gastroenteritis
(n=70)Acute liver
failure (n=28)Acute kidney
injury (n=3)Psycho neurological
disorder (n=11)Age (IQR) 45.5 (34.2, 54.0) 37.5 (28.5, 55.5) 66.0 (55.5, 66.0) 49.0 (42.0, 56.0) 45.0 (34.0, 55.2) Gender Male (%) 41 (58.57) 15 (53.57) 2 (66.67) 8 (72.73) 66 (58.93) Female (%) 29 (41.43) 13 (46.43) 1 (33.33) 3 (27.27) 46 (41.07) Hospitalization length [day (IQR)] 3.0 (1.0, 3.0) 10.0 (6.0, 12.2) 24.0 (23.5, 25.5) 6.0 (2.5, 6.0) 3.0 (2.0, 6.0) Latency period [hour (IQR)] 1.8 (0.6, 3.0) 10.0 (7.0, 10.0) 7.0 (4.0, 9.5) 2.0 (1.0, 7.5) 2.0 (1.0, 7.0) Gastric lavage Yes (%) 58 (82.86) 8 (28.57) 0 (0) 7 (63.64) 73 (65.18) No (%) 12 (17.14) 20 (71.43) 3 (100.00) 4 (36.36) 39 (34.82) Blood purification Yes (%) 0 (0) 27 (96.43) 3 (100.00) 0 (0) 30 (26.79) No (%) 70 (100.00) 1 (3.57) 0 (0) 11 (100.00) 82 (73.21) Liver transplantation Yes (%) 0 (0) 3 (10.71) 0 (0) 0 (0) 3 (2.68) No (%) 70 (100.00) 25 (89.29) 3 (100.00) 11 (100.00) 109 (97.32) Fatal mushroom poisoning* Yes (%) 1 (1.43) 28 (100.00) 3 (100.00) 5 (45.45) 37 (33.04) No (%) 69 (98.57) 0 (0) 0 (0) 6 (54.55) 75 (66.96) Outcome Non-survival (%) 0 (0) 12 (42.86) 0 (0) 0 (0) 12 (10.71) Survival (%) 70 (100.00) 16 (57.14) 3 (100.00) 11 (100.00) 100 (89.29) * Fatal mushroom poisoning is ascertained from the HOPE6 and TALK scoring outcomes of patients ( Supplementary Material ,Supplementary Table S1-S2 ).
Abbreviation: IQR=Interquartile range.Table 1. Information of patients with 4 types of mushroom poisoning (N=112).
Nine species of poisonous mushrooms were identified (Table 2). Predominant symptoms included nausea, vomiting, dizziness, and abdominal pain. Among gastroenteritis cases, Entoloma omiense (n=24), Boletus spp. (n=7), and Chlorophyllum molybdites (C. molybdites) (n=23) were implicated, with C. molybdites accounting for the highest incidence, indicating its significant role in mushroom poisoning related to gastrointestinal distress. In cases of acute liver failure, 8 cases were associated with A. exitialis, 5 with A. rimosa, and 15 with A. fuligineoides. A. rimosa exhibited the highest mortality rate (100%), followed by A. fuligineoides (40.0%) and A. exitialis (12.5%). The longest latency periods were observed in cases involving A. exitialis and A. fuligineoides, with median times of 10.0 hours (Min=4.0, Max=14.0) and 10.0 hours (Min=7.0, Max=12.0), respectively. These prolonged latency periods may have delayed clinical recognition and intervention, potentially exacerbating disease severity. Additionally, one case of acute kidney injury was reported involving Amanita neoovoidea, with a latency period of seven hours. Regarding psycho-neurological disorders, the mushrooms identified included Amanita sychnopyramis (n=3), Lanmaoa asiatica (L. asiatica) (n=3), and Boletus spp. (n=5), with L. asiatica demonstrating the longest latency period [Median (M)=10.0 hours, Min=2.0, Max=16.0]. A limitation of the analysis was that 23 cases did not have a specific mushroom type identified. Most of these unidentified cases presented with gastroenteritis (n=16), with fewer cases of acute kidney injury (n=2) and psycho-neurological disorders (n=5).
Mushroom species Symptoms Latency hours [Median (Min, Max)] Number of incidents Number of patients Number of deaths Mortality (%) Gastroenteritis Entoloma omiense Nausea, Vomiting, Dizziness, Somnolence, Abdominal pain, Abdominal distension, Diarrhea 0.6 (0.3, 3.0) 9 24 0 0 Neoboletus venenatus Nausea, Vomiting, Abdominal pain, Diarrhea, Chills 2.0 (1.5, 3.0) 3 7 0 0 Chlorophyllum molybdites Nausea, Vomiting, Dizziness, Abdominal pain, Diarrhea 2.0 (0.2, 3.0) 12 23 0 0 Unknown Nausea, Vomiting, Dizziness, Fatigue, Abdominal pain, Diarrhea, Chest Tightness 2.3 (0.5, 24.0) 12 16 0 0 Acute Liver Failure Amanita exitialis Nausea, Vomiting, Abdominal pain, Diarrhea 10.0 (4.0,14.0) 2 8 1 12.5 Amanita rimosa Nausea, Vomiting, Diarrhea 1.0 (1.0,1.0) 1 5 5 100.0 Amanita fuligineoides Nausea, Vomiting, Diarrhea 10.0(7.0,12.0) 2 15 6 40.0 Acute Kidney Injury Amanita neoovoidea Nausea, Vomiting, Altered Consciousness, Convulsions 7.0 (7.0,7.0) 1 1 0 0 Unknown Nausea, Vomiting, Oliguria, Diarrhea 7.5 (1.0,12.0) 2 2 0 0 Psycho-neurological Disorder Amanita sychnopyramis Sialorrhea, Nausea, Vomiting 0.5 (0.5, 0.5) 1 3 0 0 Lanmaoa asiatica Fatigue, Hallucinations, Visual Hallucinations, Auditory Hallucinations, Agitation, Psychosis 10.0 (2.0,16.0) 3 3 0 0 Boletus sp. Dizziness, Chest Tightness, Nausea, Vomiting, Diarrhea, Auditory Hallucinations, Hallucinations 5.0 (1.5, 12.0) 3 5 0 0 Table 2. Toxic mushroom species causing poisoning incidents and mortality in Guangzhou, China, 2016–2023.
In this study, a linear relationship was observed between latency period and hospitalization length (P for linear <0.05). As both variables are quantitative, Pearson correlation analysis was conducted, revealing a moderate positive correlation between delayed symptom onset following mushroom ingestion and hospitalization stays (r=0.39, P<0.001). A non-parametric method (Spearman’s rank correlation) was used to verify the robustness of prior findings (r=0.50, P<0.001). Furthermore, a multivariate logistic regression indicated that patients with an hour increase in latency period were likely to have a 40% increase in the risk of being identified as fatal mushroom poisoning, after adjusting for age and gender [odds ratio (OR)=1.40, 95% confidence interval (CI): 1.24, 1.62, P<0.001]. Figure 1 illustrates that most patients clustered at less than ten days hospitalization stay with less than five hours latency period.
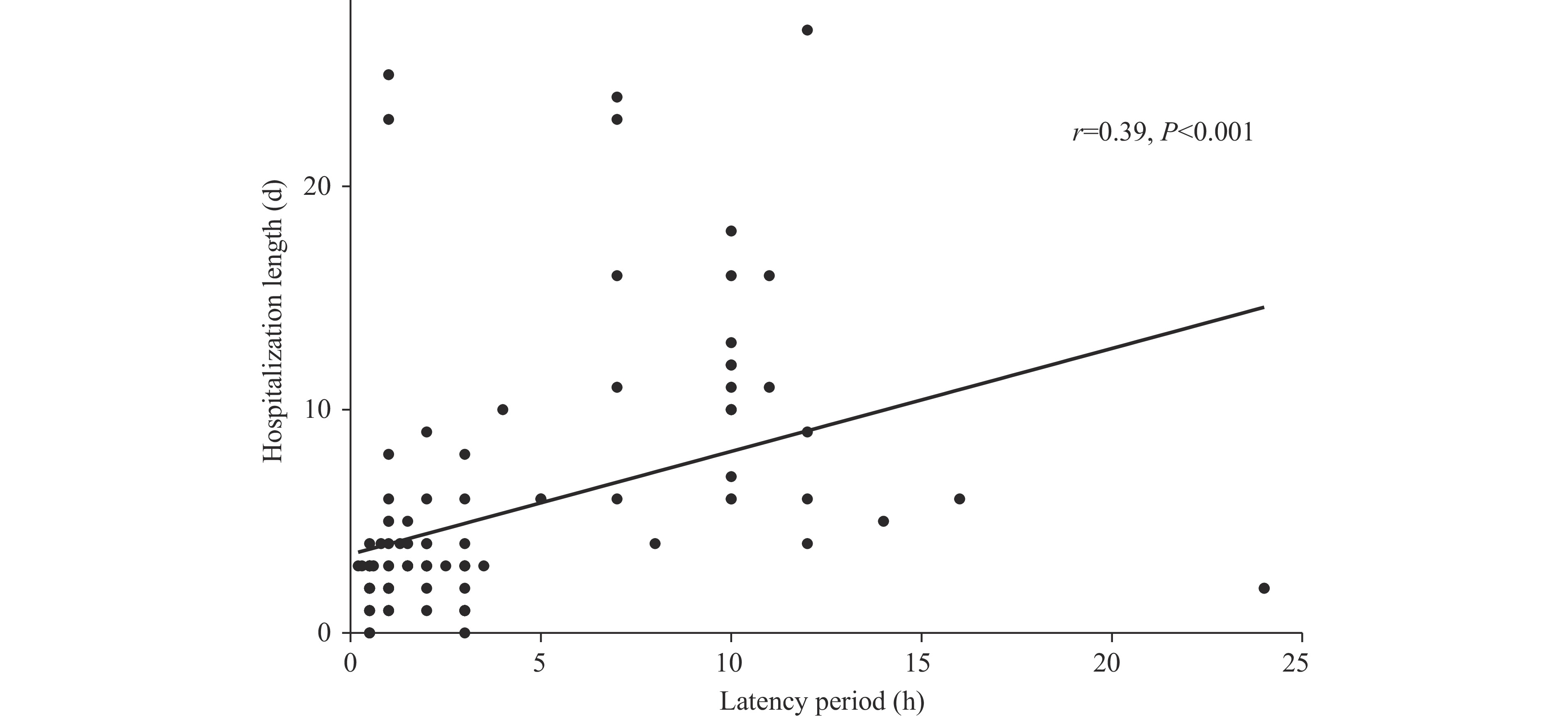 Figure 1.
Figure 1.Scatter plot for latency period in hours versus hospitalization length in days among 112 mushroom poisoning patients.
-
Mushroom poisoning remains a significant public health challenge and a notable food safety issue in China. Our study spans a 7-year period, encompassing 112 cases of mushroom poisoning reported between 2016 and 2023. Since 2002, Guangzhou Twelfth People’s Hospital has implemented comprehensive treatment protocols for acute mushroom poisoning in collaboration with the Institute of Microbiology, Guangdong Academy of Sciences, which assists with mushroom identification. Our methodology integrates three domestic scoring systems — HOPE6, TALK, and CGAMPS (3) (
Supplementary Table S3 ) — to evaluate mushroom poisoning severity and guide clinical interventions. This study analyzes disease progression patterns, optimal treatment timelines, and predictive markers through retrospective case reviews from our hospital database. The integrated framework aims to evaluate poisoning severity and inform treatment strategies across different stages of intoxication.Our study identified May and June as peak months for mushroom poisoning in Guangzhou, attributable to the region’s high humidity and heat during these months. These seasonal patterns align with observations from other regions and countries (9–11). The mortality rate in our cohort was 10.6%, with all fatalities resulting from acute liver injury. This mortality rate falls between those reported in Yunnan (23.5%) and other Chinese provincial-level administrative divisions including Zhejiang (6.8%), Jiangxi (4.1%), and Guizhou (1.8%) during comparable periods (9,12–14). Internationally, our findings are consistent with a 12.0% mortality rate in Iran, where all deaths were similarly linked to liver encephalopathy (10), and a 23.0% mortality rate among delayed liver failure patients in India, underscoring the detrimental impact of prolonged latency periods and delayed medical intervention (11). In Turkey, mortality rates were 6.8% for self-harvested and 15.2% for purchased wild mushrooms, with a 9.9% mortality and complication rate among gastrointestinal cases (15). These studies collectively highlight the negative impact of prolonged latency periods, mushroom source, and timing of initial interventions on patient outcomes. The liver-related mortality pattern in our cohort mirrors findings from Iran and India, reinforcing the severe hepatotoxicity of species such as A. rimosa. Previous research has also emphasized the importance of thorough clinical consultation and detailed patient histories in poisoning assessment, which are integral components of the HOPE6 and TALK evaluation frameworks (15).
Latency period emerged as a critical survival factor in our cohort, with patients experiencing symptoms after six hours showing significantly higher risk of fatal poisoning (2). Patients with acute liver injury exhibited the longest latency periods [M=10.0, Interquartile range (IQR): 7.0, 10.0] and highest mortality rates, followed by those with acute kidney injury (M=7.0, IQR: 4.0, 9.5), with both groups reporting 100% fatal poisoning. In contrast, patients with gastroenteritis (M=1.8, IQR: 0.6, 3.0) and psycho-neurological disorders (M=2.0, IQR: 1.0, 7.5) demonstrated shorter latency periods and substantially lower fatality rates (1.43% and 45.45%, respectively). Early gastric lavage was associated with improved survival, being performed in 82.86% of gastroenteritis cases and 63.64% of psycho-neurological cases. Blood purification therapy resulted in 100% survival among kidney injury patients.
Additionally, our study reveals that certain mushroom species can induce multiple types of complications. For instance, Boletus species triggered either gastroenteritis or psycho-neurological disorders. This highlights the complexity of mushroom poisoning cases and underscores the importance of multidisciplinary consultation based on poisoning type. Our analysis preliminarily determined mushroom types through assessment of latency period and symptomatology, which guided treatment strategies alongside morphological and molecular identification methods supported by the Institute of Microbiology Guangdong Academy of Sciences. This decision-making process aligned with the HOPE6 and TALK frameworks. Therefore, in mushroom poisoning diagnosis, HOPE6 and TALK standardized the process of clinical consultation, mushroom identification, and treatment strategy formulation. We recommend broader adoption of this system by hospitals and institutions, especially those with limited resources for mushroom identification support.
This study has several limitations. First, the retrospective design inherently carries risks of data accuracy and selection bias. Reliance on existing medical records means data may be inconsistently recorded or subject to documentation errors. For instance, HOPE6 and TALK scores were manually recorded by physicians upon patient admission, potentially introducing variability due to differences in record-keeping practices. Moreover, undocumented confounding factors, such as undiagnosed or pre-existing chronic conditions, may have influenced patient outcomes and prognostic assessments. Second, although the study spans 7 years, the sample size of 112 patients remains relatively small, limiting statistical power. Additionally, as data were collected from a single hospital in Guangzhou, the findings may not be generalizable to other regions. Selection bias also exists as patients presenting to our hospital may not reflect the broader population affected by mushroom poisoning.
Mushroom poisoning presents significant challenges in early diagnosis and treatment, particularly when the ingested mushroom species is unknown or identified late. This study implemented the HOPE6 and TALK Chinese clinical assessment protocols to identify mushroom poisoning types, demonstrating their potential to enhance multidisciplinary diagnostic processes. Future research should focus on prospective, multi-center collaborations to expand sample sizes, validate these scoring systems, and improve diagnostic accuracy. Strengthening collaboration across hospitals, toxicology centers, and CDC will be essential for integrating clinical and environmental data, ultimately improving national preparedness and outcomes in mushroom poisoning management.
HTML
FootNote
| ① | The HOPE6 and TALK scoring system, developed in 2019 based on both domestic and international literature along with clinical experience from specialists, is an assessment tool used to evaluate patients with suspected mushroom poisoning in order to identify fatal mushroom poisoning conditions, and has been recommended by Chinese mushroom experts. HOPE6: Medical history (H); Organ damage (O); Picture Identification (P); Eruption of symptom >6 hours (E6). TALK: Toxicant identification (T); APTT extension (A); Liver dysfunction (L); Kidney dysfunction (K). |
| Citation: |

|