
 Download:
Download:




-
Malaria is a significant mosquito-borne parasitic disease that substantially impedes social and economic development in endemic countries (1). According to the World Health Organization’s malaria report (2), global malaria incidence and mortality rates slightly increased in 2022. Compared to 2021, there were an additional 5 million malaria cases worldwide in 2022, totaling approximately 249 million cases. In 2022, 94% of all malaria cases (233 million cases) and 95% of all malaria deaths (580,000 cases) occurred in the African region of the WHO (2). Tanzania is among the 11 countries with the heaviest malaria burden globally, accounting for 3.1% of global cases and deaths in 2021, and 4.1% of global deaths (3). Since the early 2000s, Tanzania has expanded malaria prevention and control efforts by improving case management, distributing insecticide-treated nets (ITNs), implementing indoor residual spraying, and combining these measures with malaria treatment. These interventions successfully reduced the country’s malaria parasite prevalence by 50%. However, malaria remains a leading cause of death and morbidity across all age groups in Tanzania, particularly among pregnant women and children under five (4).
China was once a region with high malaria incidence. After launching its malaria elimination program in 2010, China implemented the “1-3-7” strategy, achieving zero local malaria cases in 2017. In 2021, China was certified as malaria-free by the World Health Organization. The National Institute of Parasitic Diseases (NIPD) at the China CDC and the Ifakara Health Institute in Tanzania jointly implemented the “China-Tanzania Pilot (Phase I) and Demonstration Projects (Phase II) on Malaria Control” from April 2015 to October 2021(5). The prevalence of malaria in the pilot areas was reduced from 25.7% to 4.9%, representing an 81% reduction (6).
Malaria morbidity control requires long-term and sustained interventions. Interruptions in 1,7-mRCTR implementation are consequences of undesirable incidents that may influence malaria control effectiveness. Due to security problems, the implementation of the Phase I project in the Rufiji intervention area was interrupted for 8 months (January 2017–August 2017). During the implementation stage of the Phase II project, an epidemic of infectious diseases caused the project to be temporarily interrupted again (March 2020–May 2020), and malaria prevention and control work in the intervention area stagnated. Although cross-sectional survey data confirmed the effectiveness of our implementation, the impact of these two interruptions on intervention effectiveness is currently unknown. Therefore, this study used data on malaria cases reported by local health facilities in the intervention area to analyze the impact of implementation interruptions using an interrupted time-series model, which provides a theoretical basis for further optimizing preventive and control measures and improving intervention effectiveness.
-
The China-Tanzania Pilot and Demonstration Projects on Malaria Control were implemented in two phases: Phase I (January 2016 to April 2018) and Phase II (September 2019 to October 2021). The project proposed and tested an integrated package of intervention measures called 1,7-malaria Reactive Community-Based Testing and Response (1,7-mRCTR) at two intervention sites (Chumbi and Ikwiriri) in the Rufiji Region, South Tanzania, which has been described previously (7). Phase II expanded 1,7-mRCTR from two to six sites in Tanzania, funded by the Bill and Melinda Gates Foundation (BMGF). It covered Kilwa District (Lindi Region) and Rufiji and Kibiti Districts (Pwani Region) in southeastern Tanzania, with two wards per district representing four catchment populations. However, as Rufiji District received additional interventions beyond larvicidal treatment, only Kilwa and Kibiti Districts were included in assessing Phase II interruption impacts.
-
We obtained patient registration data from health institutions through an information reporting system developed by professional technicians at the Ifakara Health Institute. The data included demographic information of patients, their village addresses, and malaria status. Weekly malaria incidence per 100 people was calculated based on all confirmed malaria cases.
-
All individuals registered in health facilities within the study period were included in the analysis. During Phase II, there were very few weeks with missing values for malaria case numbers in the intervention areas’ health facilities, which were addressed using multiple imputation (MI). MI was selected over complete-case analysis due to its ability to preserve statistical power and reduce bias under the missing-at-random (MAR) assumption, implemented via the R mice package. We decomposed the weekly malaria incidence changes by applying seasonal and trend decomposition using loess (STL) (7–8).
Interrupted time series analysis (ITSA) (9-10) was used to evaluate the impact of the 1,7-mRCTR implementation interruption on intervention effectiveness. Considering the seasonal nature of malaria incidence, the decompose function in R was first used to remove the effect of seasonal factors, and one-period lagged Newey-west regression was used to assess the effect of intervention interruptions on malaria control in the intervention area. Statistical analyses were performed using Stata version 15 (StataCorp, College Station, USA) and R statistical software, version 4.3.2 (R Foundation for Statistical Computing,Vienna, Austria). All reported P values are two-tailed, with P value <0.05 considered statistically significant.
-
As shown in Figure 1, during Phase I, the Rufiji intervention area experienced a 0.13% weekly decline in malaria incidence, while the control area showed a 0.10% weekly increase (Figure 1A). In Phase II, the Kilwa and Kibiti intervention areas maintained a declining trend of 0.08% weekly, outperforming the control area which decreased at a rate of 0.04% weekly (Figure 1B).
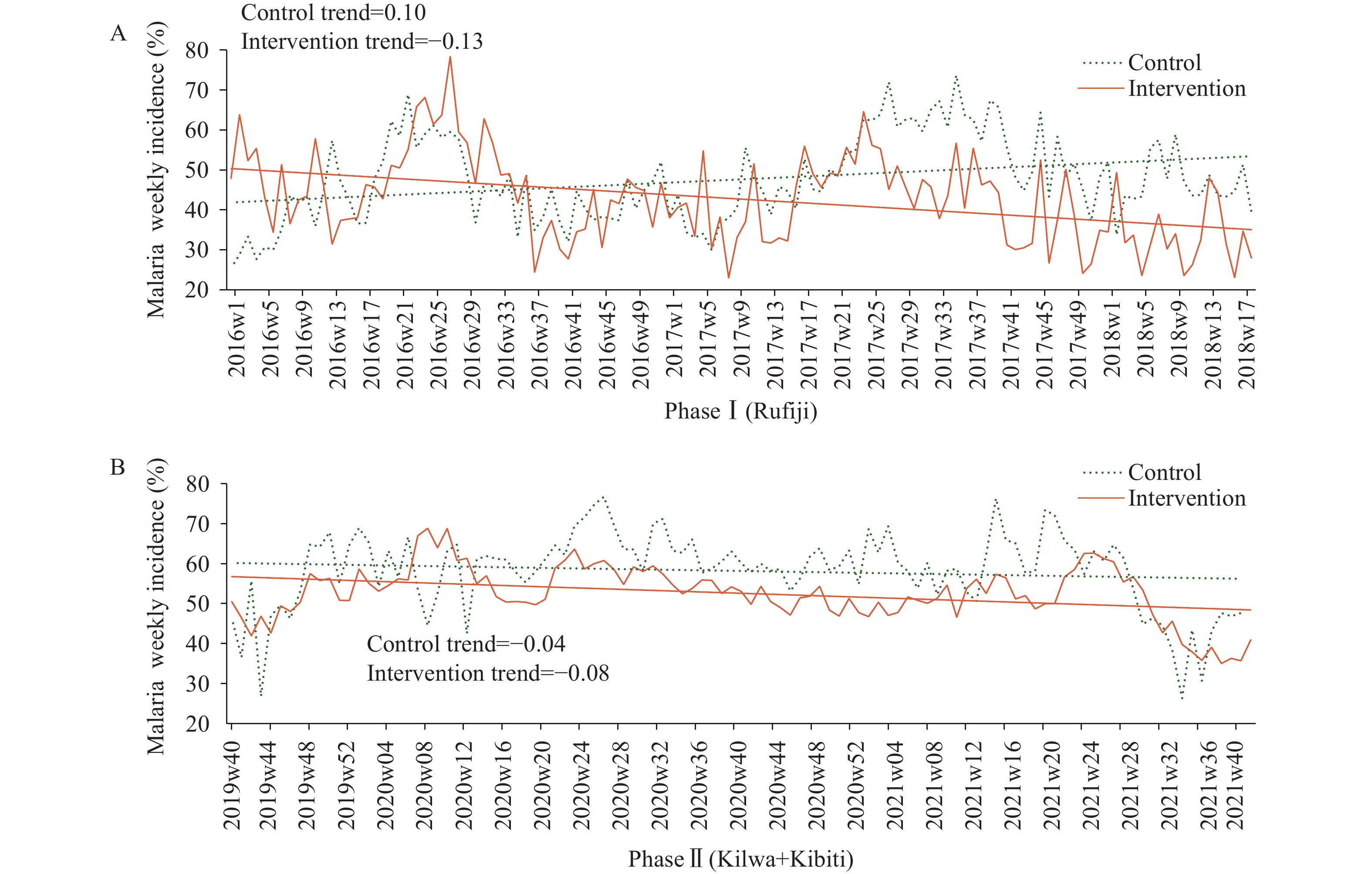 Figure 1.
Figure 1.Weekly incidence changes of malaria in 1,7-malaria Reactive Community-Based Testing and Response intervention and control areas in Tanzania. (A) Phase I; (B) Phase II.
-
Figure 2 demonstrates that despite the overall downward trend in malaria incidence in Phase I intervention areas, a substantial rebound occurred from January to May 2017. Similarly, malaria incidence in Phase II intervention areas showed a sharp increase during the pre-intervention period, approximately from January to May 2020. Additionally, clear seasonal patterns in malaria incidence were observed across the implementation areas. Further analyses revealed that the peak malaria transmission season in the Tanzanian intervention area occurred from November to December, with a secondary peak from June to July (
Supplementary Figure S1 ).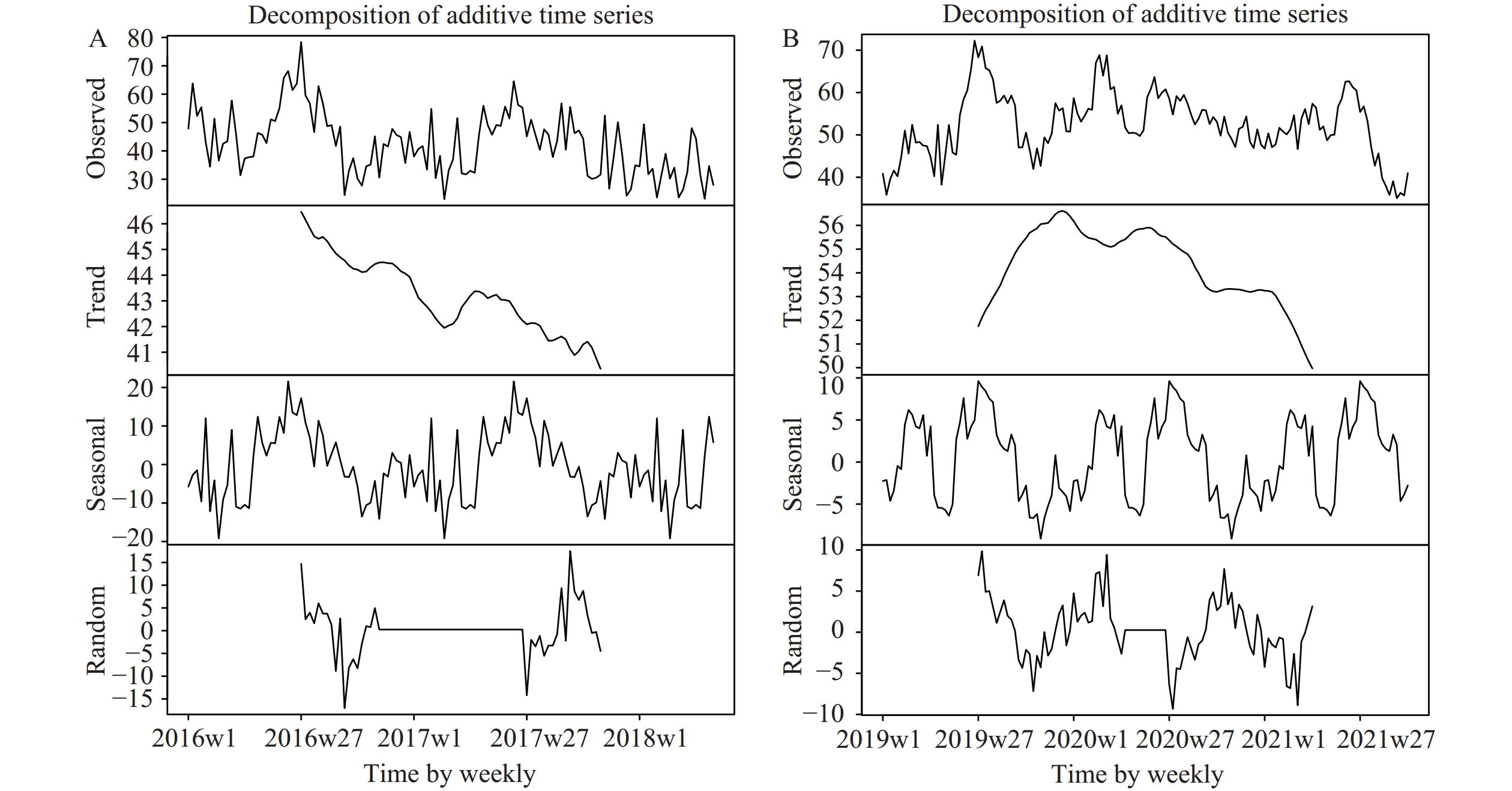 Figure 2.
Figure 2.Time series decomposition plot of malaria incidence in 1,7-malaria Reactive Community-Based Testing and Response implementation areas. (A) Phase I; (B) Phase II.
-
As shown in Figure 3 and Table 1, Phase I intervention areas initially demonstrated a 51.10% weekly malaria incidence with a 0.17% weekly decline. A one-week interruption caused an immediate 6.69% drop (P=0.116) but reversed the trend from a 0.17% decline to a 0.58% increase. Following resumption (Figure 3B), incidence dropped by 8.96% (P=0.039) with a sustained 0.39% long-term decline (P=0.003). Seasonally adjusted analysis revealed that the interruption reduced the downward trend from 0.08% to 0.02%, with post-resumption recovery maintaining a 0.07% weekly decline (P=0.003).
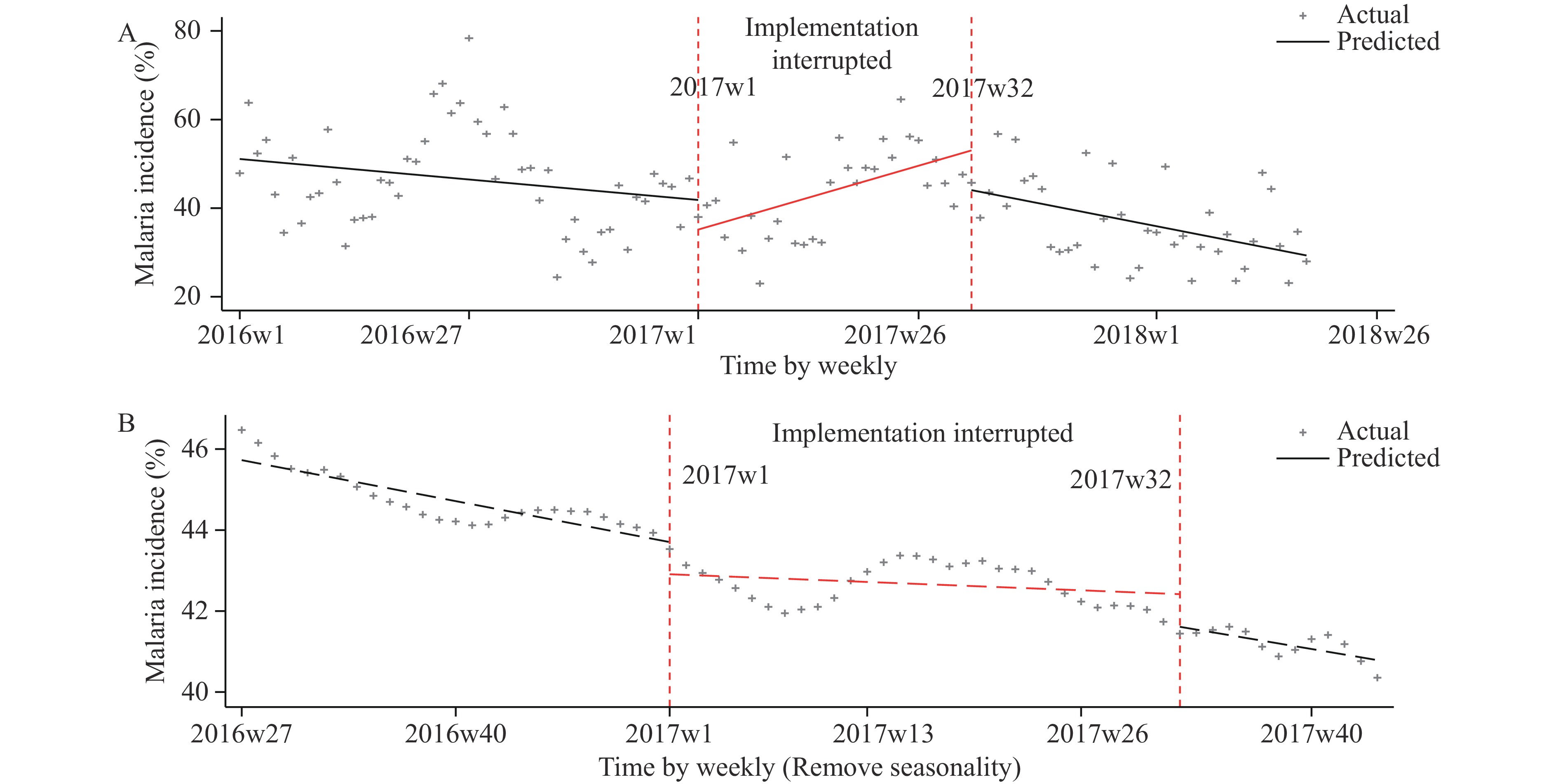 Figure 3.
Figure 3.ITS scatter plot of the weekly malaria incidence in Phase I implementation areas, Tanzania. (A) Implementation interrupted; (B) Implementation interrupted after removing seasonality.
Period Variables Phase I Phase I (Adjust seasonality) Coefficient 95% CI P Coefficient 95% CI P 2016w1–
2016w12Initial level 51.1 45.01, 57.19 <0.001 45.73 45.33, 46.12 <0.001 Trend −0.17 0.01, −0.36 0.049 −0.08 0.05, 0.10 <0.001 2017w1–
2017w32Immediate level change after
interrupted 1 week−6.69 −15.06, 1.68 0.116 −0.79 0.22, 1.37 0.008 Trend changes after interrupted 0.75 0.37, 1.14 <0.001 0.06 0.03, 0.10 0.001 Trend 0.58 0.23, 0.92 0.001 −0.02 −0.04, 0.01 0.209 2017w33–
2018w18Immediate level change after implementation recovery 1 week −8.96 0.45, 17.48 0.039 −0.81 0.33, 1.29 0.001 Trend changes after
implementation recovery−0.96 0.55, 1.38 <0.001 −0.05 0.01, 0.11 0.047 Trend −0.39 0.15, 0.63 0.002 −0.07 0.02, 0.11 0.003 Abbreviation: CI=confidence interval. Table 1. Estimated level and trend changes of malaria weekly incidence before and after 1,7-malaria Reactive Community-Based Testing and Response interruption (Phase I).
Phase II intervention areas began with 44.48% incidence and an early 0.87% weekly increase (Table 2). A one-week interruption caused a 0.35% rise but reversed the trend from increasing 0.87% to decreasing by 1.16% weekly (P<0.001). Following resumption (Figure 4A), incidence surged 10.3% (P=0.007) but stabilized to a 0.19% long-term decline (P<0.001). Seasonally adjusted data revealed an initial 0.02% decline (Figure 4B), interrupted by a 0.70% drop and a trend shift from a decrease of 0.02% to an increase of 0.08%. Post-resumption, malaria weekly incidence decreased by 0.30% [95% confidence interval (CI): −0.62, 0.02; P=0.063] in the first week, though this effect was not statistically significant. After continuous implementation, the incidence trend changed by 0.18% and maintained a long-term decline of 0.11% (95% CI: 0.09, 0.12; P=0.001) per week.
Period Variables Phase II Phase II (Adjust seasonality) Coefficient P 95% CI Coefficient P 95% CI 2019w40–
2020w8Initial level 44.48 <0.001 40.75, 48.21 56.15 <0.001 55.69, 56.62 Trend 0.87 <0.001 0.48, 1.25 −0.02 0.293 −0.06, 0.02 2020w9–
2020w22Immediate level change after interrupted 1 week 0.35 0.918 −6.47, 7.18 −0.7 0.007 0.20, 1.21 Trend changes after interrupted −2.03 <0.001 1.12, 2.94 0.1 0.001 0.06, 0.14 Trend −1.16 0.006 0.34, 1.98 0.08 <0.001 0.06, 0.09 2020w23–
2021w40Immediate level change after implementation recovery 1 week 10.3 0.007 2.89, 17.71 −0.3 0.063 −0.62, 0.02 Trend changes after implementation recovery 0.98 0.021 0.15, 1.81 −0.18 <0.001 0.16, 0.21 Trend −0.19 <0.001 0.09, 0.29 −0.11 0.001 0.09, 0.12 Table 2. Estimated level and trend changes of malaria weekly incidence before and after 1,7-mRCTR interruption (Phase II).
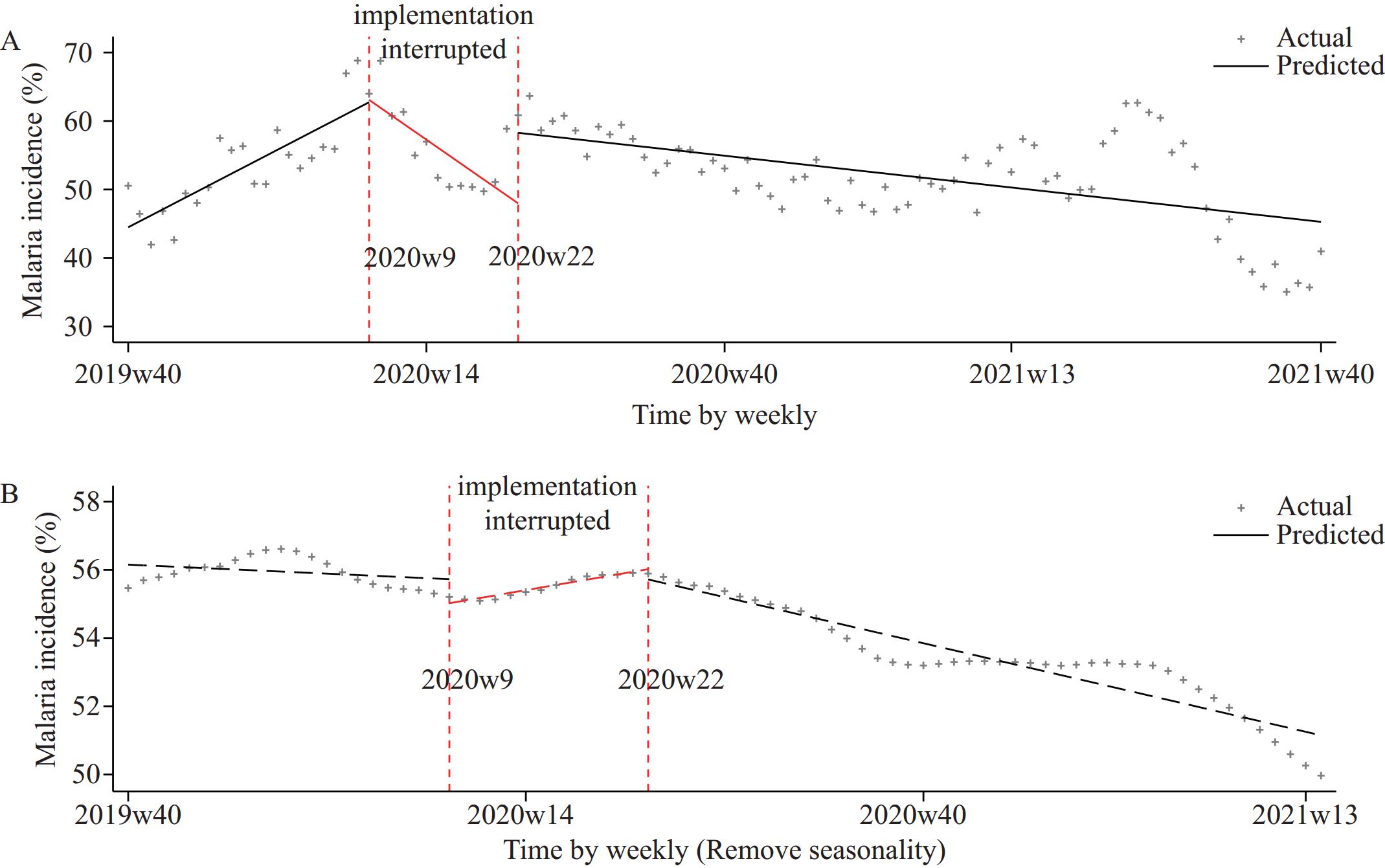 Figure 4.
Figure 4.ITS scatter plot of the weekly malaria incidence in Phase II implementation areas, Tanzania. (A) Implementation interrupted; (B) Implementation interrupted after removing seasonality.
-
Disease control requires sustained, long-term efforts which are vulnerable to disruptions from program continuity issues, climate shifts, and policy changes. Despite these challenges, limited guidance exists for addressing implementation interruptions, which often compromise study outcomes (11). By examining implementation gaps in the China-Tanzania Malaria Control Project, we assessed the impacts of both short- and long-term disruptions to inform strategies for minimizing interruptions and optimizing interventions. In Rufiji, Tanzania — the first site to implement China’s 1,7-mRCTR approach — malaria incidence in intervention villages decreased by over 15.7% by the end of Phase I (12). Longitudinal health facility data confirmed a consistent downward trend in intervention areas during Phase I, validating the effectiveness of the 1,7-mRCTR strategy.
Phase I data revealed that malaria incidence increased by 0.58% weekly during the 8-month interruption, returning to pre-implementation levels. Despite Tanzania’s ongoing long-term insecticidal net campaigns, seasonally adjusted analysis showed that the interruption reduced the downward trend to 25% of pre-interruption rates, with post-resumption weekly declines decreasing from 0.08% to 0.07% (a 12.5% reduction). The infectious disease pandemic disrupted malaria control efforts globally (13-14), halting Tanzania’s interventions for 3 months (March–May 2020) due to logistical challenges and RDT shortages, with an additional 13 weeks of intermittent interruptions following resumption. Phase II incorporated larval control and insecticide spraying in Rufiji (15), so this district was excluded from our analysis to avoid confounding effects.
In Phase II (beginning October 2019), malaria incidence initially increased before the infectious disease pandemic (likely due to seasonal peaks) but showed a downward trend when adjusted for seasonality. During the pandemic, reported cases decreased (possibly due to reduced mobility), though seasonally adjusted data revealed a transient upward trend, indicating that interrupted interventions allowed a slow resurgence of malaria. Phase II’s post-resumption RDT shortages caused sporadic interruptions over 13 weeks with irregular, brief disruptions, so their impact was not separately analyzed. Our analysis demonstrated that while weekly malaria incidence fluctuated during supply shortages, seasonally adjusted data showed minimal long-term effect. This highlights the importance of stockpiling malaria supplies, particularly in high-transmission areas. We recommend that healthcare facilities pre-stock RDTs and treatments based on local population needs to maintain screening capabilities during emergencies.
This study has several limitations: its retrospective design potentially introduced uncontrolled biases and confounders; reliance on RDTs may have missed low-density malaria infections; and the infectious disease pandemic could have delayed malaria case reporting.
-
The eight-month interruption during Phase I reduced the effectiveness of the 1,7-mRCTR implementation by 12.5%. In contrast, the three-month passive interruption during Phase II caused only minor transient fluctuations with minimal impact on the overall effectiveness of the 1,7-mRCTR approach. Additionally, temporary shortages of RDT reagents had negligible effects on implementation effectiveness.
-
Ifakara Health Institute.
-
The Medical Research Coordination Committee of the National Institute for Medical Research (NIMR) granted the permit to conduct this study (NIMR/HQ/R.8a/Vol.IX/2005 and 3634). Institutional ethical approval was also obtained from the Ifakara Health Institute Institutional Review Board (IHI/IRB/No: 18-2015 and 18-2020) and the Chinese Center for Disease Control (201,505).
HTML
Study Area
Data Sources
Statistical Analysis
Description of Malaria Incidence Changes
Time Series Feature Decomposition
Interruption Time Series Analysis
| Citation: |

|