
 Download:
Download:




-
Introduction: Myocarditis is a common cardiovascular disease that can lead to severe complications. This study investigates the epidemiological characteristics of myocarditis in China by analyzing incidence, mortality, and disability-adjusted life years (DALYs) trends from 1992 to 2021.
Methods: Using the Global Burden of Disease Study(GBD 2021)database, this study analyzed myocarditis incidence, mortality, DALYs, age-standardized rates, and average annual percent change (AAPC) from 1992 to 2021. An average percent change (APC) model was applied to assess the impact of age, period, and birth cohort on myocarditis mortality risk. Disease burden comparisons were made across different age and gender groups in China.
Results: Compared to 1992, China saw a decline in age-standardized incidence, mortality, and DALYs rates of myocarditis in 2021. From 1992 to 2021, the AAPC in the standardized incidence rate, mortality rate, and DALYs rate of myocarditis in China were −0.223 (95% CI: −0.234 to −0.212), −0.525 (95% CI: −0.861 to −0.187), and −1.958 (95% CI: −2.219 to −1.696), respectively. Males had higher rates than females, with faster declines observed in females. Risk factors for myocarditis mortality included being under 5 or over 70 years old, living in 2002–2016, and belonging to birth cohorts before 1957. APC model results were similar for males and females.
Conclusions: Although China’s myocarditis disease burden is decreasing,its age-standardized mortality and DALYs rates remain above global levels. Continued vigilance in prevention and control is essential. Priority should be given to primary and secondary prevention for individuals under 5, over 70, and males, with a focus on health education and management.
-
Myocarditis is an inflammatory lesion of the myocardium, which is a common one in cardiovascular diseases. It is characterized by inflammatory infiltration in the myocardium and degeneration and necrosis of non-ischemic cardiomyocytes (1). Meanwhile, myocarditis is also an important cause of sudden cardiac death, acute heart failure, and chronic dilated cardiomyopathy (2). Data from Global Burden of Diseases (GBD) 2019 reported that the number of patients, new cases, and deaths of myocarditis in China increased by 85.62%, 47.51%, and 50.22%, respectively, in 2019 compared with 1990. Before the coronavirus disease 2019 (COVID-19) pandemic, the global incidence of viral myocarditis was about 1 to 10 cases per 100,000 people per year (3). After the outbreak of COVID-19, it found that in patients hospitalized for COVID-19 the incidence of acute myocarditis is 2.4 to 4.1 cases per 1000 people (4). This study used GBD 2021 data and an age-period-cohort model to analyze the trend of the burden of myocarditis in China, and found that the burden of myocarditis in China has generally decreased from 1992 to 2021. However, the number of morbidity and mortality continue to rise, and both the ASMR and age-standardized disability-adjusted life-years (DALYs) rate remain above the global average the overall burden of myocarditis in China is showing a downward trend. The findings may assist policymakers in making more informed decisions, improving resource allocation, and optimize healthcare resources.
The data source is the Global Burden of Disease Research 2021 (GBD 2021) database.It documents the incidence, prevalence, mortality, years of life lost (YLLs), years lived with disability (YLDs), and DALYs due to 371 diseases and injuries in 204 countries or regions around the world (5). The IE algorithm of the age-period-cohort model was applied in this study. This algorithm integrates the three variables of age, period, and cohort into a single variable through a series of linear algebraic transformations, making the model estimable. This study selected three indicators: incidence, mortality and DALYs. Based on the globally age-standardized population figures provided by GBD 2021 (6), we conducted age-standardization for these indicators to investigate the epidemiological characteristics of myocarditis in the overall Chinese population and in male and female populations from 1992 to 2021.
Compared with 1992, the number of cases and deaths of myocarditis in China increased, and DALY decreased in 2021. Meanwhile, the age-standardized incidence rate, mortality rate and DALYs rate all decreased. The changes of disease burden of myocarditis in the world were consistent with those in China. Among them, the age-standardized incidence rate and DALYs rate changed more than the world, while the age-standardized mortality rate showed the opposite characteristics (Table 1).
Area Incidence Death DALYs Number (10,000) P’ Number (10,000) P’ Number (10,000) P’ Global 1992 82.13 16.87 2.26 0.56 104.25 19.78 2021 131.97 16.16 3.18 0.40 96.31 12.41 2021 vs. 1992 (%)* 60.69 −4.20 40.43 −28.53 −7.61 −37.28 China 1992 18.64 17.41 0.84 1.08 46.07 44.59 2021 26.93 16.33 1.42 0.92 34.35 25.26 2021 vs.1992 (%)* 44.47 −6.20 69.03 −14.41 −25.43 −43.36 Note: P’ was Age-standardized rate, expressed as 1/100,000.
* Percentage change (%) was calculated as the difference between 2021 and 1992 divided by the amount in 1992.
Abbreviations: DALYs=disability-adjusted life years.Table 1. The analysis of incidence, death and DALYs of myocarditis in China and the world in 1992 and 2021.
The ASIR of myocarditis in China is consistent with the global rates (Figure 1A), indicating similar trends and incidence levels. The ASMR and age-standardized DALYs rate initially increased and then decreased. However, the burden of disease in China was high, with a larger fluctuation range of ASMR and DALYs rates compared to the global average (Figure 1B, 1C). From 1992 to 2021, the ASIR, ASMR, and age-standardized DALYs rate of myocarditis exhibited similar characteristics among Chinese men and women when considering the entire population. The ASIR, ASMR, and age-standardized DALYs rate for myocarditis were higher in men than women; however, there is an overlap between their uncertainty intervals.
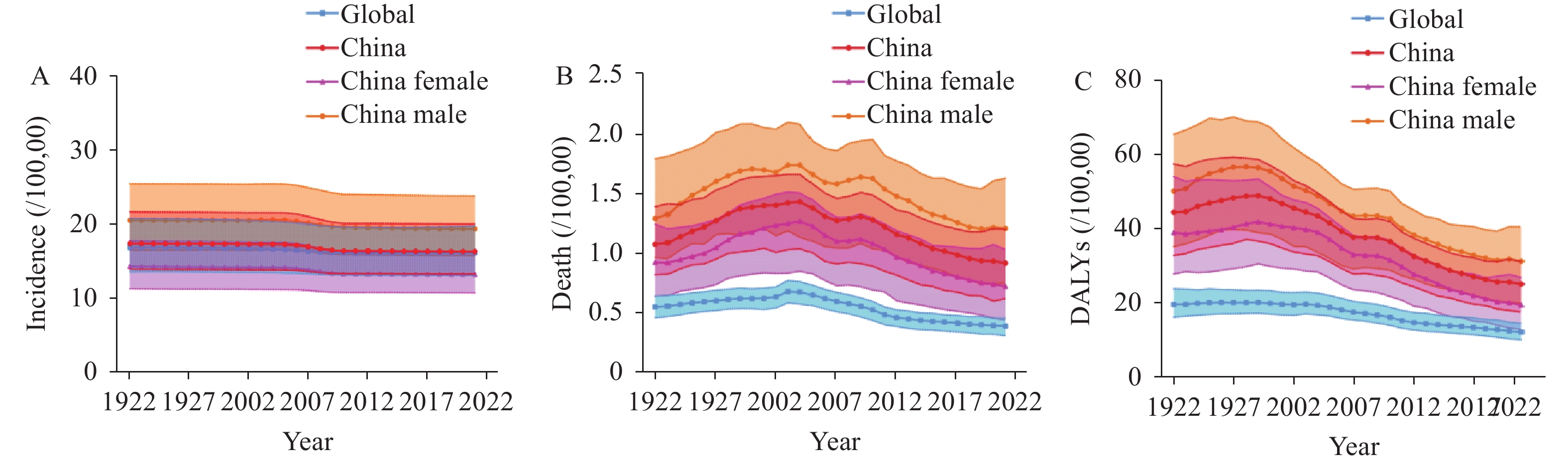 Figure 1.
Figure 1.Disease burden of myocarditis in China and the world from 1992 to 2021. (A) ASIR; (B) ASMR; (C) Age-standardized DALYs rate.
Note: Shaded sections indicate 95% uncertainty intervals.
Abbreviations: ASIR=age-standardized incidence rate; ASMR=age-standardized mortality rate; DALYs=disability-adjusted life years
The ASMR and age-standardized DALYs rate first increased and then decreased, and the turning points from increasing to decreasing were 2001 and 1999, respectively (
Supplementary Table S1 ). In general, the age-standardized incidence rate, mortality rate and DALYs rate of myocarditis in China showed a downward trend from 1992 to 2021, and the AAPC was −0.223 (95% CI: −0.234 to −0.212), −0.525 (95% CI: −0.861 to −0.187) and −1.958 (95% CI: −2.219 to −1.696), respectively. Meanwhile, the ASIR, ASMR, and age-standardized DALYs rate of myocarditis in Chinese men and women displayed a declining trend from 1992 to 2021, with a more rapid decrease observed in women. The AAPC of the disease burden of myocarditis in both genders was less than 0. Except for the AAPC of male ASMR, the AAPC of other disease characteristics were statistically significant (Table 2).Measure Sex AAPC 95% CI t P Age-standardized incidence rate Both −0.223 −0.234, −0.212 −39.738 <0.001 Female −0.270 −0.285, −0.256 −35.934 <0.001 Male −0.200 −0.216, −0.185 −24.724 <0.001 Age-standardized mortality rate Both −0.525 −0.861, −0.187 −3.045 0.002 Female −0.764 −0.963, −0.565 −7.5 <0.001 Male −0.23 −0.612, 0.154 −1.173 0.241 Age-standardized DALYs rate Both −1.958 −2.219, −1.696 −14.547 <0.001 Female −2.329 −2.645, −2.012 −14.251 <0.001 Male −1.610 −1.91, −1.309 −10.416 <0.001 Abbreviation: AAPC=average annual percent change; CI=Confidence Interval; DALYs=disability-adjusted life years. Table 2. Changes in AAPC for each indicator of myocarditis disease burden in China, 1992−2021.
The age-period-cohort model revealed that age significantly influences myocarditis mortality, with initial risk decline, subsequent stabilization, and later escalation (Figure 2). The highest risks were in those under 5 and over 95 years, with the latter 177.6 times more likely to die than the 25–29 age group. Age acted as a protective factor for 5–69-year-olds but a risk factor for younger and older ages. Period effects showed the lowest mortality risk in 1992–1996, peaking in 2007–2011, with a 1.41-fold increased risk compared to the earlier period. Cohort analysis indicated the highest death risk in those born 1912–1916 and the lowest during 2017–2021, with a 14.5-fold increased risk for the former. Meanwhile, the mortality risk of men and women was affected by age, period and birth cohort, which was basically consistent with the characteristics of the whole population (Figure 2). Under the age of five and over 95 years old for male and female two peak death risk, while both the lowest risk of death ages at 10–14 and 45–49 years old, respectively, where the highest risk of death is 163.52 and 239.71 times higher, respectively, than the lowest risk. Overall, both genders reflected the same results, with the age effect having the greatest impact on the risk of death, followed by the cohort effect, and finally the period effect having the least impact.
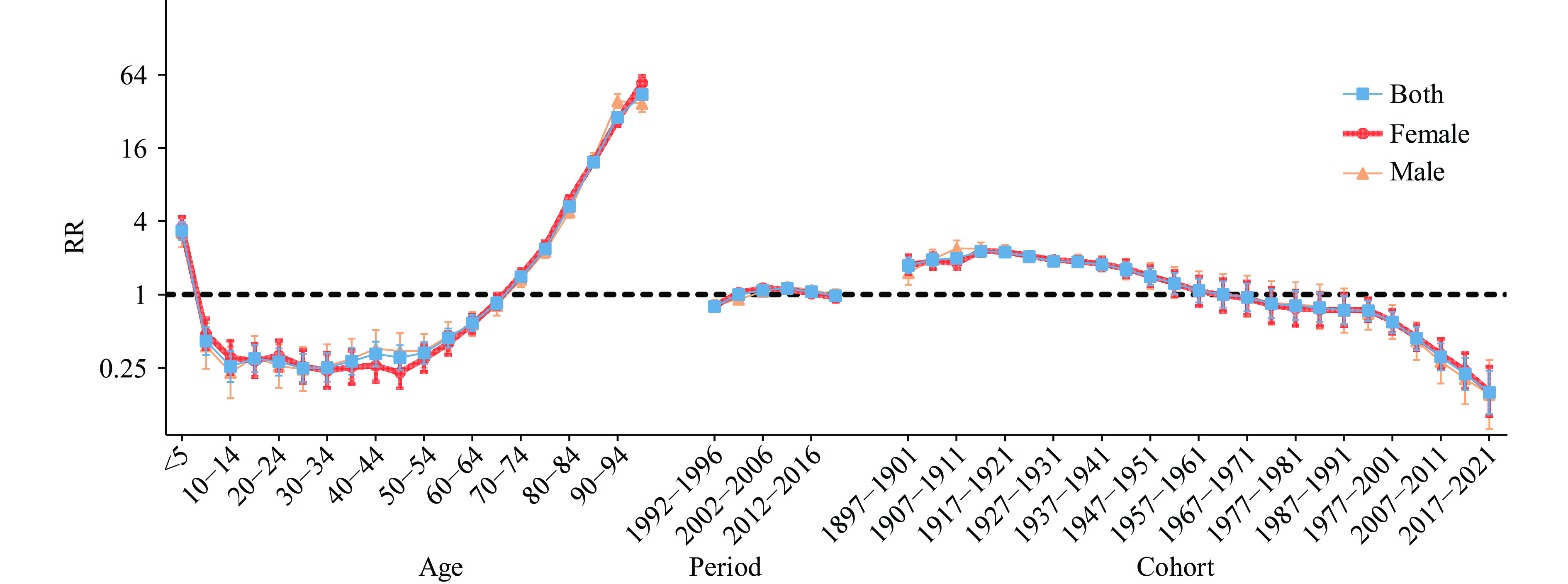 Figure 2.
Figure 2.Age-period-cohort modeling to analyze the risk and 95% CI of death from myocarditis in China.
Abbreviation: RR= relative risk; CI=confidence interval. -
In this article, Myocarditis estimated disease burden and its changes in China were analyzed in detail. The findings indicate that the ASIR, ASMR, and DALYs rate for myocarditis in China in 2021 were lower than those in 1992. Conversely, the incidence and mortality of myocarditis globally and within China in 2021 showed a marked increase from 1992, while DALY has decreased both globally and in China. This could stem from advancements in medical technology that allow more effective treatments, shortening recovery times and thus minimizing disability from the illness. Furthermore, an increase in the proportion of the older adult population might result in more deaths, yet potentially lower long-term disability impacts, thereby possibly reducing the overall DALYs. We found that the ASMR and age-standardized DALYs rates were higher than the global averages. This may be due to the uneven distribution of medical resources in China, lifestyle and environmental factors related to the progression of myocarditis. Nevertheless, given the significant rise in myocarditis cases and fatalities, a comprehensive understanding of myocarditis is essential, along with heightened focus on its prevention and treatment. Meanwhile, the AAPC of the burden of myocarditis was less than 0 in both men and women from 1992 to 2021, and it was lower in women than in men. This suggests that we should strengthen health management and health promotion for the male population. This phenomenon may be related to the differences in physiological structure and immune system between men and women. Some studies have shown that there is a significant gender difference between cardiomyocytes and fibroblasts, which affects the size of the heart; moreover, about 30% of men have larger hearts than women do (7). Furthermore, women have smaller coronary vessels than men do, premenopausal women have lower blood pressure, and the percentage of LVEF is higher in women than in men (8). In addition to the variations in cardiac physiological functions attributable to gender, differences in sex hormones may significantly contribute to the heightened incidence observed in males. Sex hormones seem to modulate the acute cardiac response to inflammation, potentially influencing the risk of progressing to chronic dilated cardiomyopathy (9). Conversely, testosterone promotes immune dysfunction by inhibiting anti-inflammatory cells and activating Th1-type immune responses, thus facilitating the development of myocarditis through abnormal immune-mediated mechanisms (10).
In this study, being under 5 years or over 70 years of age, during the period 2002–2016, and belonging to a birth cohort prior to 1957 were identified as risk factors for mortality from myocarditis. This indicates that prevention and treatment efforts for myocarditis should particularly target children under 5 years of age and older adult individuals over 70. Pediatric myocarditis is a condition that can develop rapidly, leading to severe complications such as acute heart failure, cardiogenic shock and fatal arrhythmias. Fulminant myocarditis, a particularly severe form of myocarditis, has a sudden onset and rapid progression, causing hemodynamic changes that typically result in heart failure and life-threatening arrhythmias as well as cardiogenic shock within 2 to 3 days. This form of myocarditis is more common in children and has a high mortality rate, with serious arrhythmias being a common cause of sudden death in children. Myocarditis has been identified as an important cause of sudden cardiac death in young children (11). The challenge of diagnosing myocarditis in this group, coupled with the disease’s swift progression, leads to a high mortality rate among affected children. Additionally, children’s immune systems may overreact to pathogens, exacerbating myocardial damage. Thus, the swift progression of myocarditis and the potential for severe cardiac complications, along with an overactive immune response, contribute to the high mortality rate in children with the disease. Therefore,early identification and provision of appropriate testing and supportive care for affected children are essential to mitigate mortality rates. Additionally, the increased mortality observed in older adult may stem from diminished immune function associated with aging, which impairs the immune system’s adaptability to infections and reduces the influx of T cells from the thymus into the periphery. Concurrently, chronic immune activation and memory cell expansion may also contribute, ultimately leading to immune cell senescence and disorders within the immune system, diminishing the capacity to respond to new antigens (12). Furthermore, the comparative analysis of age-period-cohort model results between male and female populations revealed no significant disparity in mortality risk across genders. This indicates that age, period, and birth cohort are not significant determinants of mortality differences between men and women.
Nevertheless, this study was subject to at least two limitations. Primarily, it relies on GBD 2021 data analysis, yet the database does not specify myocarditis incidence and prevalence across different provincial-level administrative divisions, regions, and seasons. Secondly, GBD data is mainly estimated by combining statistical models and system dynamics models, and there may be some differences between the data and the actual situation.
This research found that the disease burden of myocarditis in China has decreased in the past 30 years. However, the incidence and mortality rates continue to rise, and the ASMR and the ratio of DALYs remain higher than the global average. Although there is a significant downward trend in mortality and DALYs rates among children under 5, both the under-5 and over-70 age groups are still identified as risk factors for myocarditis mortality. The probability of myocarditis occurrence in men is higher than in women in China, with the AAPC of myocarditis burden being negative for both genders, and lower in women than in men. Therefore, we should focus on the myocarditis burden in men, young children, and the elderly, and relevant departments should adopt more proactive measures to mitigate this burden, including enhancing health education and advancing medical diagnosis and treatment levels.
-
The GBD 2021 team.
HTML
| Citation: |

|