
 Download:
Download:




-
Introduction: Tetanus remains a significant public health concern in China, with a notable proportion of injured patients declining tetanus vaccination. This study aims to investigate the prevalence and determinants of tetanus vaccine hesitancy and identify effective strategies to address this critical public health challenge.
Methods: We calculated tetanus vaccine hesitancy rates among trauma patients presenting at eight hospitals across China from April 1 to June 30, 2024. A comprehensive questionnaire survey was conducted from June 3 to June 27, 2024, targeting patients aged 11 years and older who had open wounds requiring tetanus immunization but refused vaccination. The survey assessed participants’ sociodemographic characteristics, knowledge, attitudes, and practices regarding tetanus and tetanus vaccines. Statistical analyses included Pearson’s Chi-squared tests, multiple response analyses, and goodness of fit tests.
Results: Among 8,993 trauma patients requiring tetanus vaccination, 26.78% declined immunization. Analysis of 503 consecutively collected questionnaires revealed low overall awareness of tetanus and tetanus vaccines, with only 20.1% of respondents demonstrating comprehensive knowledge of tetanus-related questions. The predominant reason for vaccine hesitancy (34.5%) was the perception that post-injury tetanus risk was minimal. Across all age groups, medical institutions and healthcare professionals were consistently identified as the most effective sources for tetanus prevention information.
Conclusion: This study demonstrates that enhancing public awareness about tetanus and its vaccines while addressing complacency are fundamental to reducing vaccine hesitancy. Targeted educational interventions delivered by healthcare institutions and professionals can significantly improve public knowledge and acceptance of tetanus vaccination.
-
Tetanus is an acute, specific, toxic disease caused by Clostridium tetani (1). The condition is preventable through vaccination and post-exposure prophylaxis (2). While the incidence of tetanus has declined substantially in developed countries (3), it remains a significant public health challenge in regions with inadequately implemented immunization programs and in middle- and low-income countries (3).
Since the 1970s, China has prioritized tetanus prevention and control, progressively implementing policies to enhance vaccine accessibility. In 2019, guided by the World Health Organization (WHO) “Tetanus vaccines: WHO position paper, February 2017 — Recommendations” (4) and considering China’s healthcare landscape, the National Health Commission of the People’s Republic of China issued the “Diagnostic and Treatment Protocol for Non-Neonatal Tetanus (2019 edition)” and the “Guidelines for the Use of Tetanus Vaccine and Passive Immunizing Agents After Injury (2019 edition)” (5-6). These guidelines, revised in October 2024, established the first clear standards for post-trauma tetanus vaccination. They stipulate that patients with unreliable or absent tetanus immunization history should complete the full immunization schedule, while those vaccinated more than 5–10 years prior should receive a booster dose. However, emergency physicians in China generally possess limited knowledge of tetanus treatment and prevention, resulting in overutilization of tetanus immune globulin (TIG) or tetanus antitoxin (TAT) in clinical practice, while vaccines are often neglected (2). Additionally, a significant proportion of trauma patients continue to refuse tetanus vaccination for complex and poorly understood reasons.
In 2012, the WHO defined vaccine hesitancy as the delay in acceptance or refusal of vaccines despite their availability (7-8). Multiple factors influence vaccine hesitancy, including the recipient’s perception of disease risk, trust in healthcare systems, cost considerations, and socioeconomic factors (7,9). Public health and vaccine policies, healthcare practitioners’ communication skills, and vaccine promotion channels all interact with vaccine hesitancy (9). This hesitancy can ultimately contribute to the resurgence and spread of preventable infectious diseases.
This study represents the first investigation in China to examine knowledge (K), attitudes (A), and vaccination intentions (practice, P) (10) among patients exhibiting hesitancy toward tetanus vaccination following injury. Conducted across eight hospitals in seven cities, the research explores the underlying reasons for tetanus vaccine refusal among trauma patients, providing valuable insights for developing targeted tetanus prevention strategies tailored to China’s specific national context.
-
From April 1, 2024, to June 30, 2024, this study documented the number of trauma patients requiring tetanus vaccination across eight hospitals, tallied those who refused vaccination, and calculated the vaccine hesitancy rate. The primary descriptive cross-sectional study was conducted consecutively with patients who met the following criteria: aged over 11 years, presenting with open wounds requiring tetanus immunization, and refusing the recommended vaccination. Participants were recruited from eight hospitals: Peking University First Hospital, Dezhou Municipal Hospital, Changshu Hospital Affiliated to Nanjing University of Chinese Medicine, Dazhou City Center Hospital (Sichuan Province), Qingdao Children and Women’s Hospital, Qingdao Eighth People’s Hospital, Norinco General Hospital, and The First People’s Hospital of Lanzhou City. The questionnaire study was administered face-to-face between June 3, 2024, and June 27, 2024. Participation was entirely voluntary.
-
The formula n=Z2a/2×p×(1-p)/ε² was employed, where Za/2 represents the value of the standard normal distribution, ε represents the margin of error, and p denotes the prevalence of tetanus. Assuming a=0.05, then Za/2=1.96 with a margin error of 5%, a minimum of 385 participants were required. Since the prevalence of tetanus in China was indeterminate, we opted for the most conservative estimate by assuming p=0.5, thereby maximizing the sample size for calculations.
-
The questionnaire comprised sections on sociodemographic characteristics (Questions 1–5), knowledge of tetanus disease and tetanus vaccine (Questions 6–9), reasons for vaccine hesitancy (Question 10), and practices regarding tetanus vaccination (Questions 11–13). The complete questionnaire is available in
Supplementary Table S1 . -
Data analysis was performed using SPSS Statistics (version 29.0.2.0, IBM, Chicago, United States). Categorical variables were expressed as percentages and compared using Pearson’s Chi-squared test. Goodness of fit test and multiple response analysis were employed for multiple-choice questions. Statistical significance was defined as P<0.05.
-
From April 1, 2024, to June 30, 2024, a total of 8,993 trauma patients required tetanus vaccination across the eight participating medical institutions. Among these patients, 2,408 (26.78%) refused vaccination, while 6,585 (73.22%) accepted it. During the focused survey period from June 3, 2024, to June 27, 2024, we collected 503 completed questionnaires from vaccine-hesitant patients. Table 1 presents the demographic and socioeconomic characteristics of the respondents.
Characteristics N (%) Age (years) 11–17 25 (5.0) 18–45 261 (51.9) 46–65 166 (33.0) >65 51 (10.1) Gender Female 276 (54.9) Male 227 (45.1) Education background Postgraduates 41 (8.2) Graduates 125 (24.9) College graduates 50 (9.9) High school graduates 77 (15.3) Junior high school graduates 78 (15.5) Primary school graduates 63 (12.5) Other 69 (13.7) Hospital Peking University First Hospital 58 (11.5) Dezhou Municipal Hospital 88 (17.5) Changshu Hospital Affiliated to Nanjing University of Chinese Medicine 49 (9.7) Dazhou City Center Hospital, Sichuan Province 10 (2.0) Qingdao Children and Women’s Hospital 7 (1.4) Qingdao Eighth People’s Hospital 112 (22.3) Norinco General Hospital 163 (32.4) The First People’s Hospital of Lanzhou City 16 (3.2) Regional economic level High-income cities 226 (44.9) Upper-middle income cities 277 (55.1) Note: The eight participating hospitals are strategically distributed across northern, southern, eastern, and western regions of China. According to World Bank classification standards and based on 2023 per capita GDP, 3 of the 7 cities represent high-income areas (Beijing: 200,000 CNY, Changshu: 166,000 CNY, and Qingdao: 152,000 CNY), while 4 cities fall into the upper-middle-income category (Dezhou: 69,000 CY, Dazhou: 50,000 CNY, Xi’an: 92,000 CNY, and Lanzhou: 79,000 CNY).
Abbreviation: GDP=gross domestic product; CNY=Chinese Yuan.Table 1. Characteristics of participants of the survey (N=503).
Table 2 summarizes participant responses to four key questions regarding tetanus and tetanus vaccination. Overall, participants demonstrated low awareness levels, with higher educational attainment correlating positively with better understanding of tetanus and tetanus vaccines (
Supplementary Figure S1 ). As detailed inSupplementary Table S2 , only 20.1% of respondents demonstrated comprehensive awareness by correctly answering all four tetanus-related questions (Questions 6–9), while 25.6% were completely unaware of any of the queried information.Education background Question 6 Question 7 Question 8 Question 9 Yes, N (%) No, N (%) Yes, N (%) No, N (%) Yes, N (%) No, N (%) Yes, N (%) No, N (%) Postgraduates 32 (78.0) 9 (22.0) 16 (39.0) 25 (61.0) 31 (75.6) 10 (24.4) 14 (34.1) 27 (65.9) Graduates 99 (79.2) 26 (20.8) 58 (46.4) 67 (53.6) 86 (68.8) 39 (31.2) 48 (38.4) 77 (61.6) College graduates 43 (86.0) 7 (14.0) 21 (42.0) 29 (58.0) 30 (60.0) 20 (40.0) 25 (50.0) 25 (50.0) High school graduates 59 (76.6) 18 (23.4) 20 (26.0) 57 (74.0) 24 (31.2) 53 (68.8) 16 (20.8) 61 (79.2) Junior high school graduates 51 (65.4) 27 (34.6) 15 (19.2) 63 (80.8) 21 (26.9) 57 (73.1) 16 (20.5) 62 (79.5) Primary school graduates 24 (38.1) 39 (61.9) 3 (4.8) 60 (95.2) 7 (11.1) 56 (88.9) 1 (1.6) 62 (98.4) Other 27 (39.1) 42 (60.9) 16 (23.2) 53 (76.8) 18 (26.1) 51 (73.9) 21 (30.4) 48 (69.6) Sum 335 (66.6) 168 (33.4) 149 (29.6) 354 (70.4) 217 (43.1) 286 (56.9) 141 (28.0) 362 (72.0) χ2 46.010 44.416 93.735 45.766 P <0.001 <0.001 <0.001 <0.001 Note: Question 6: Did you know that you may develop tetanus after trauma or animal scratches (bites)? Question 7: Did you know that TIG or TAT provides only short-term protection and cannot completely prevent tetanus infection? Question 8: Did you know that the “DTP vaccine” administered during childhood includes tetanus vaccine? Question 9: After completing the full course of tetanus vaccination, immunity remains effective for at least 5–10 years. Only one booster dose is needed when reinjury occurs more than 5 years after the full-course vaccination. Were you aware of this information? Table 2. Knowledge of participants about tetanus disease and tetanus vaccine in different educational background.
For the multiple-choice question regarding reasons for refusing the tetanus vaccine (Figure 1), 503 participants provided a total of 1,073 responses. The goodness-of-fit test showed statistical significance (χ2=324.486, P<0.001), indicating substantial differences in the distribution of response choices. The predominant reason for tetanus vaccine refusal, cited by 34.5% of respondents, was the belief that “there is little risk of tetanus infection after this injury.” Only 4.9% of respondents expressed concerns about the quality and effectiveness of tetanus vaccines as their rationale for refusal. Cross-analysis revealed significant associations between educational level and reasons for vaccine refusal (χ2=69.647, P<0.001), demonstrating that vaccine hesitancy motivations varied substantially across educational strata. Participants with graduate and postgraduate degrees expressed greater concerns about vaccine side effects compared to those with other educational backgrounds (31.2% and 43.9%, respectively). Conversely, individuals with lower educational attainment, particularly primary and junior high school graduates, were more likely to cite the lengthy vaccination process as their reason for refusal (66.7% and 60.3%, respectively).
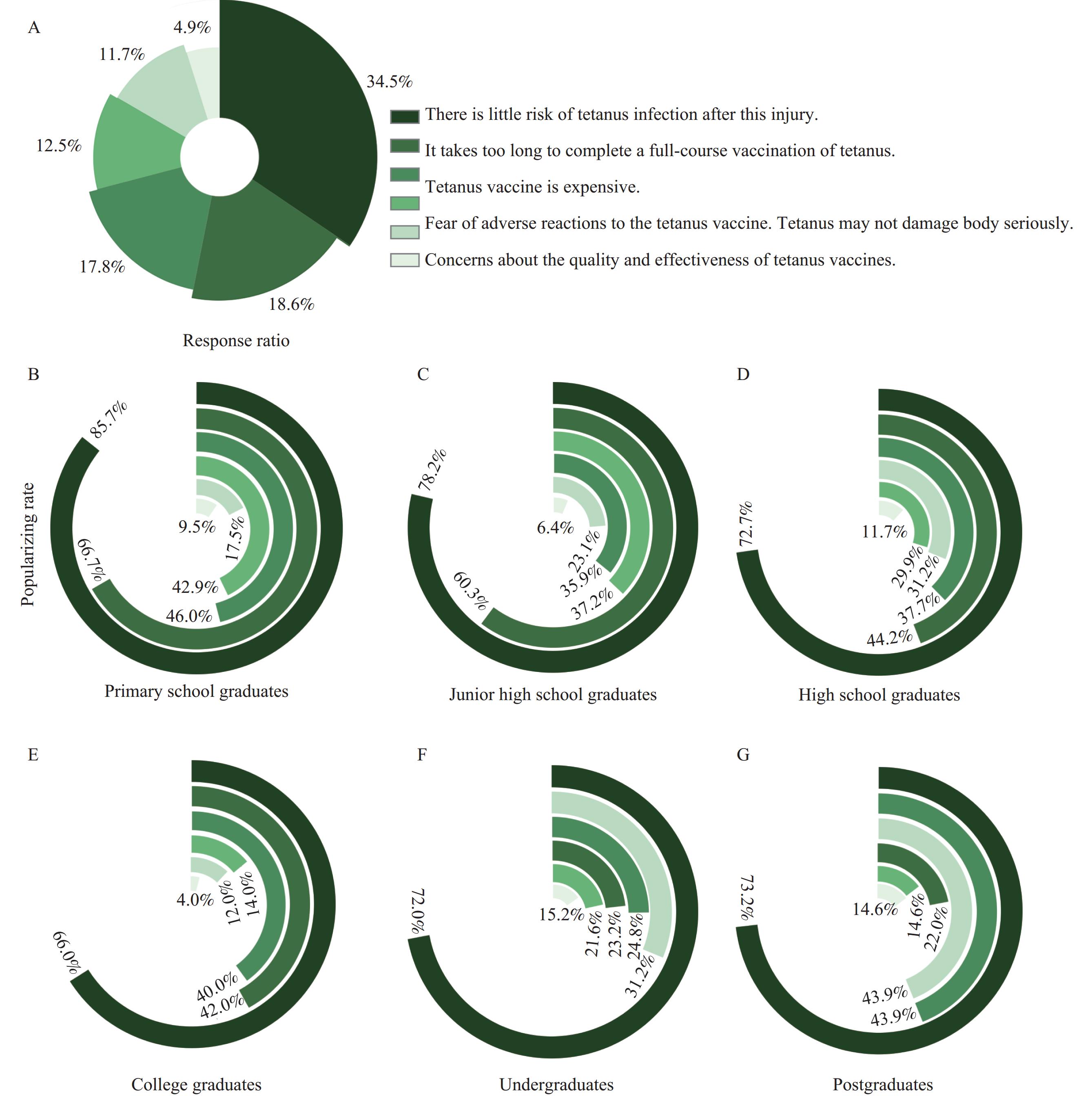 Figure 1.
Figure 1.Reasons of refusing the tetanus vaccine and educational backgrounds. (A) Response ratio for different reasons of tetanus vaccine refusal among participants. Popularizing rate of tetanus vaccine refusal for different reasons among participants who are (B) primary school graduates, (C) junior high school graduates, (D) high school graduates, (E) college graduates, (F) undergraduates, and (G) postgraduates respectively.
In
Supplementary Figure S2 , the 503 participants reported a total of 943 responses regarding their previous sources of tetanus prevention information, with the goodness-of-fit test showing statistical significance (χ2=184.408, P<0.001). Medical institutions or healthcare personnel constituted the most frequently cited information source (31.2%). Similarly, for the multiple-choice question about “the most effective way to learn about tetanus prevention” (Supplementary Figure S3 ), participants provided 1,066 total responses, with the goodness-of-fit test again showing significance (χ2=217.218, P<0.001). Medical institutions or healthcare personnel were again identified as the most effective information source (37.1%).The final question assessed whether participants would reconsider their decision and accept vaccination after completing the questionnaire. As shown in Table 3, 35% of the 503 participants changed their minds and decided to receive the tetanus vaccine. Notably, primary school graduates demonstrated the lowest rate of decision reversal (7.9%) compared to other educational cohorts. Postgraduates and graduates exhibited the highest rates of reconsideration (63.4% and 50.4%, respectively). The proportion of participants willing to change their decision varied significantly across age groups, with a clear inverse relationship between age and willingness to reconsider. Among participants under 18 years old, 72% ultimately changed their minds, compared to only 5.9% of participants over 65 years old. Furthermore, participants from high-income cities demonstrated significantly higher rates of decision reversal (44.2%) compared to those from upper-middle income cities (27.4%), a statistically significant difference (χ2=15.463, P<0.001). Among those who changed their minds, the lowest proportion selected family and friends as effective sources for tetanus information (
Supplementary Table S3 ).Changing decision Characteristics Yes, N (%) No, N (%) χ2 P Education background Postgraduates 26 (63.4) * 15 (36.6) * Graduates 63 (50.4) *,† 62 (49.6) *,† College graduates 12 (24.0) § 38 (76.0) § High school graduates 28 (36.4) †, § 49 (63.6) †,§ 53.462 <0.001 Junior high school graduates 21 (26.9) § 57 (73.1) § Primary school graduates 5 (7.9) ¶ 58 (92.1) ¶ Other 21 (30.4) § 47 (69.6) § Sum 176 (35.0) 327 (65.0) Age (years) 11–17 18 (72.0) * 7 (28.0) * 18–45 126 (48.3) † 135 (51.7) † 76.704 <0.001 46–65 29 (17.5) § 137 (82.5) § >65 3 (5.9) ¶ 48 (94.1) ¶ Sum 176 (35.0) 327 (65.0) Regional economic level High-income cities 100 (44.2) * 126 (55.8) * 15.463 <0.001 Upper-middle-income cities 76 (27.4) † 201 (72.6) † Sum 176 (35.0) 327 (65.0) Note: For each group, identical superscript markers indicate no statistically significant difference between groups, while different superscript markers denote statistically significant differences between groups. Table 3. Population of changing decision after completing the questionnaire.
-
Globally, tetanus affects an estimated 1 million individuals annually, resulting in approximately 200,000 deaths, with the highest burden concentrated in Southeast Asia and Africa (11). While comprehensive epidemiological data on non-neonatal tetanus in China remain limited, available evidence suggests that tetanus incidence in China substantially exceeds rates observed in the United States and European countries (12). Therefore, implementing the 2024 diagnostic and treatment standards for non-neonatal tetanus and accelerating population-wide vaccination initiatives in China represent critical public health priorities.
Despite tetanus vaccine availability across all eight participating hospitals, 26.78% of trauma patients declined vaccination. This study represents the first comprehensive investigation and analysis of tetanus vaccine hesitancy in China. Our findings reveal that individuals exhibiting vaccine hesitancy generally demonstrated poor knowledge regarding tetanus disease and its prevention through vaccination. Unfortunately, because our study design excluded trauma patients who accepted vaccination, comparative analysis of tetanus awareness between hesitant and non-hesitant groups was not possible. Overall, educational attainment positively correlated with greater awareness of tetanus and its vaccine.
Vaccination acceptance involves a complex decision-making process influenced by multiple determinants. Vaccine hesitancy — defined as delayed acceptance or refusal of vaccines despite availability — stems from various factors (7-8). Several conceptual frameworks categorize vaccine hesitancy determinants, with the “3Cs” model offering particular clarity. First proposed to the WHO in 2011, this model delineates three primary categories: complacency, convenience, and confidence (7). In recent years, researchers worldwide have employed the “3Cs” model to analyze factors contributing to vaccine hesitancy among healthcare practitioners and vaccine recipients. Our research identified the predominant reason for tetanus vaccine hesitancy among Chinese trauma patients as the belief that “there is little risk of tetanus infection after this injury,” which aligns with the psychological factor of complacency within the “3Cs” framework. Paradoxically, successful immunization programs may engender complacency and ultimately vaccine hesitancy, as individuals weigh perceived vaccination risks against disease risks (7). The relative rarity of tetanus in China — attributable to governmental, institutional, and healthcare practitioner efforts — appears to underlie complacency as the leading cause of vaccine hesitancy. Participants with higher educational attainment expressed greater concerns regarding vaccine side effects, reflecting diminished confidence in vaccine safety. Vaccination duration (convenience) disproportionately influenced vaccination attitudes among individuals with lower educational levels or those residing in upper-middle income cities, potentially reflecting occupational constraints or financial considerations.
Our study further revealed that most participants obtained tetanus prevention information from medical institutions and healthcare professionals, whom they also regarded as the most effective information sources. Consequently, ensuring healthcare providers possess comprehensive knowledge of tetanus vaccine guidelines and effectively communicate this information to the public is paramount. Notably, approximately one-third of initially hesitant participants changed their minds and consented to vaccination by the conclusion of our survey. This finding suggests that healthcare professionals can significantly reduce vaccine hesitancy and increase tetanus vaccination rates through evidence-based education about tetanus and its prevention (such as clarifying that TIG or TAT provides only short-term protection and cannot fully prevent tetanus, whereas complete vaccination confers immunity for at least 5–10 years). Additionally, empathetic, non-judgmental communication — rather than procedural vaccine introduction — proves most effective in building trust and mitigating vaccine hesitancy (13–14).
Our findings demonstrate that vaccine hesitancy becomes increasingly entrenched with advancing age, paralleling observations that COVID-19 vaccine hesitancy among elderly Chinese populations exceeds rates in the United States and European countries (15–17). With China hosting the world’s largest elderly population — many of whom lack fundamental knowledge about tetanus and face higher tetanus-associated mortality — targeted prevention strategies for this vulnerable demographic could substantially reduce the medical and economic burden of this disease.
Several limitations warrant acknowledgment. Our questionnaire lacked comprehensiveness, omitting factors such as participants’ physical and economic conditions that may influence vaccine hesitancy. The questionnaire was not a validated scale, precluding reliability and validity analyses. Additionally, all participating hospitals maintaining tetanus vaccine supplies, potentially introducing selection bias. Physicians at these facilities likely possessed superior understanding of tetanus vaccination guidelines and demonstrated greater proactivity in recommending vaccination compared to hospitals without vaccine availability. Furthermore, patients with existing tetanus knowledge may preferentially select hospitals known to provide tetanus vaccines. Consequently, our observed vaccine hesitancy rate may underestimate the true prevalence, suggesting that the national tetanus vaccination landscape may be more concerning than our findings indicate. The exclusion of primary and secondary healthcare institutions introduced additional selection bias. Moreover, our study did not incorporate medical facilities from less economically developed regions, explaining the limited representation of lower-middle and low-income areas in China.
In conclusion, this research underscores the critical importance of enhancing public awareness regarding tetanus and its prevention through vaccination. Addressing complacency, strengthening confidence in vaccine safety, and improving tetanus vaccination accessibility represent essential strategies for mitigating vaccine hesitancy in China. Leveraging medical institutions and healthcare providers as primary information channels may significantly enhance understanding and uptake of tetanus vaccinations. The pronounced resistance to vaccination among older adults necessitates targeted interventions for this demographic. These findings provide valuable insights for governmental and health policymakers to strategically promote tetanus vaccination and reduce vaccine hesitancy rates.
-
Approval from the Ethics Committee of Peking University First Hospital (Ref:2024YAN632). All participants provided written informed consent prior to enrollment.
HTML
Data Collection
Sample Size Calculation
Survey Content
Statistical Analysis
| Citation: |

|