
 Download:
Download:




-
Introduction: The spread of misinformation and disinformation during infectious disease outbreaks and public health emergencies can significantly impede effective public health responses. This infodemic phenomenon creates confusion and erodes public trust, leading to uncertainty in crisis situations. This study aimed to assess the health department’s capacity and capabilities in infodemic preparedness and management to enhance future emergency preparedness in accordance with International Health Regulations (IHR)-2005 guidelines.
Methods: A mixed-methods cross-sectional study was conducted in the health department of Khyber Pakhtunkhwa. Semi-structured interviews with experts were conducted in August-September 2024 using a self-administered assessment tool based on IHR-2005 guidelines, supplemented by analysis of departmental documents and supporting evidence. Data were analyzed using descriptive statistics, with achievement levels scored from 0% to 100% across five categories.
Results: The overall preparedness score was 21.7%, indicating limited capacities and capabilities. The risk communication and community engagement (RCCE) coordination system showed some strengths, with 80% of focal persons designated and moderate intersectoral coordination (40%), but lacked emergency spokesperson training. Community engagement activities demonstrated moderate effectiveness (40%). Key weaknesses included insufficient human resources (20%), inadequate technological infrastructure (20%), absence of infodemic analysis (0%), and lack of joint infodemic planning (0%). Significant delays were observed in identifying and responding to potentially harmful misinformation.
Conclusions: Despite some effective practices in community engagement, substantial gaps exist in infodemic management preparedness. Critical deficiencies were identified in human and technological resources and infodemic response measures. Priority areas for improvement include human resource development, infodemic surveillance systems, digital tools implementation, and enhanced collaboration. The adoption of innovative tools and streamlined processes is essential for strengthening emergency risk communication preparedness.
-
The spread of misinformation and disinformation alongside infectious disease outbreaks can significantly impede public health responses. This study assessed the health department’s capacity in infodemic management to enhance future emergency response capabilities. A mixed-methods cross-sectional study was conducted in the Khyber Pakhtunkhwa health department using semi-structured expert interviews based on International Health Regulations (IHR)-2005 guidelines, complemented by departmental document review of risk communication capacities. The overall preparedness score was 21.7%, indicating substantial deficiencies in capacities and capabilities. While some strengths were observed in the risk communication and community engagement (RCCE) coordination system, with 80% designated focal persons, intersectoral coordination remained moderate (40%) with notable gaps in emergency spokesperson training. Community engagement activities demonstrated moderate effectiveness (40%). Key weaknesses included limited human resources (20%), limited technological infrastructure (20%), absence of infodemic analysis (0%), and significant delays in identifying and responding to misinformation spread. Despite some effective practices in coordination and community engagement, critical gaps persist in infodemic management preparedness, particularly in human and technological resources and response measures. Priority areas for improvement include human resource development, infodemic surveillance systems, digital tool implementation, and enhanced stakeholder collaboration.
Public health emergencies and disease outbreaks can be significantly exacerbated by the concurrent spread of misinformation and disinformation. While misinformation refers to false information shared without malicious intent, disinformation represents deliberately misleading content. The rapid dissemination of diverse and often contradictory information during outbreaks or emergencies can precipitate an infodemic situation. An infodemic is characterized by an overabundance of information, including false or misleading content, in digital and physical environments during a disease outbreak (1). These infodemics can propagate rapidly and achieve widespread reach, particularly during the initial phases of an epidemic or emergency when official information is limited (2–4). Pakistan’s second Joint External Evaluation (JEE) identified substantial gaps in health emergency preparedness, risk communication, and infodemic management systems (5). The Khyber Pakhtunkhwa province, operating under a devolved health system, lacks a comprehensive risk communication and community engagement plan, though some informal community engagement activities are conducted within the existing primary healthcare framework (5–6). This study represents an effort to assess the capacities within Khyber Pakhtunkhwa to identify best practices, gaps, and challenges. The research aims to identify enablers, bottlenecks, and existing infodemic management capacities to strengthen health department preparedness for future public health crises. Furthermore, the findings and methodological approach will contribute to the evolving field of infodemic management by providing valuable insights for low- and middle-income countries (LMICs) in assessing their risk communication and infodemic response capabilities.
This cross-sectional study was conducted at the Provincial Health Department of Khyber Pakhtunkhwa, Pakistan. A total of 19 subject matter experts (SMEs) were recruited through departmental correspondence, comprising 15 public health experts and 4 additional specialists (
Supplementary Table S1 ). These SMEs were nominated by their respective organizations, representing the animal health department, climate change, environment, and information and public relations departments.Primary data collection occurred from August to September 2024 using a self-administered semi-structured tool based on the Health Emergency Preparedness Self-Assessment (HEPSA) guidelines developed by the European CDC (7). The tool was modified and contextualized to assess RCCE and infodemic capacities as recommended in the IHR Benchmarks 2023 (8). Focus group interviews were conducted at the provincial health department using a peer-to-peer consensus-building approach, as recommended by Joint External Evaluation (4). Additionally, public health planning documents from 2021 onward were reviewed.
Data analysis employed descriptive statistics following the scoring guidelines of the HEPSA tool (7), GHS Index, and CEDM tool developed by New Zealand Ministry of Civil Defense and Emergency Management (9). A percentage-based scoring system was implemented to assess departmental achievement across various progress levels. The scale ranged from “Never” (0%) indicating complete absence of implementation to “Always” (100%) signifying full achievement with sustainable practices. Intermediate levels included “Infrequently” (20%) for initial stages, “Sometimes” (40%) for partial progress without systematic approach, “Often” (60%) for demonstrated commitment with unclear full attainment, and “Mostly” (80%) for substantial progress with minor limitations (
Supplementary Table S2 ). Both descriptive statistical analysis and qualitative thematic analysis were conducted on the primary data and departmental documentation.The overall score for Risk Communication and Infodemic Management preparedness was 21.7%, indicating significant deficiencies in the health department’s capacity and readiness to manage infodemic situations during large-scale outbreaks and public health emergencies.
As shown in Table 1, the RCCE coordination system demonstrated variable capacity across different domains. The department consistently maintained designated RCCE focal persons with dedicated authority (80% achievement). However, public health spokespersons were appointed only during emergencies and lacked formal RCCE training. Intersectoral coordination operated primarily on an ad hoc basis, achieving moderate capacity (40%). The overall capacity distribution is illustrated in
Supplementary Figure S1 .Sr# Indicator Score Remarks 1 RCCE focal person 80% RCCE focal person and spokesperson were identified. 2 Infodemic surveillance 20% Lacks a proper system for online infodemic surveillance and monitoring. 3 Tools for surveillance 0% No software available for monitoring online information flow. 4 Rumor verification 40% Somewhat functional rumors verification system in place. 5 Infodemic analysis 0% Lacks a system for infodemic analysis. 6 Sentiments analyses 20% Sentiment analysis not being used. 7 Trained staff 20% Only 2 staff trained on infodemic surveillance and analysis. 8 Social media engagement 40% Somewhat functional social media community engagement system in place. 9 Active partnerships 20% Only 3 active partnerships with WHO, UNICEF and Polio EOC. 10 Information sharing 0% No information sharing meetings or briefings about misinformation or disinformation. 11 Joint planning for infodemic response 0% No joint action plans for infodemic response. Note: This table presents the preparedness capacity scores of the Khyber Pakhtunkhwa Health Department for infodemic management. A score of 100% indicates full preparedness, while 0% indicates no preparedness. The “Remarks” column provides contextual explanations for the assigned scores.
Abbreviation: RCCE=risk communication and community engagement.Table 1. Preparedness capacity scores of Khyber Pakhtunkhwa Health Department for infodemic management.
Figure 1 reveals critically limited technological infrastructure for RCCE and infodemic management, with an overall score of 12%. The department’s technological readiness was particularly concerning, with only one training session conducted on communication channel utilization (Table 1).
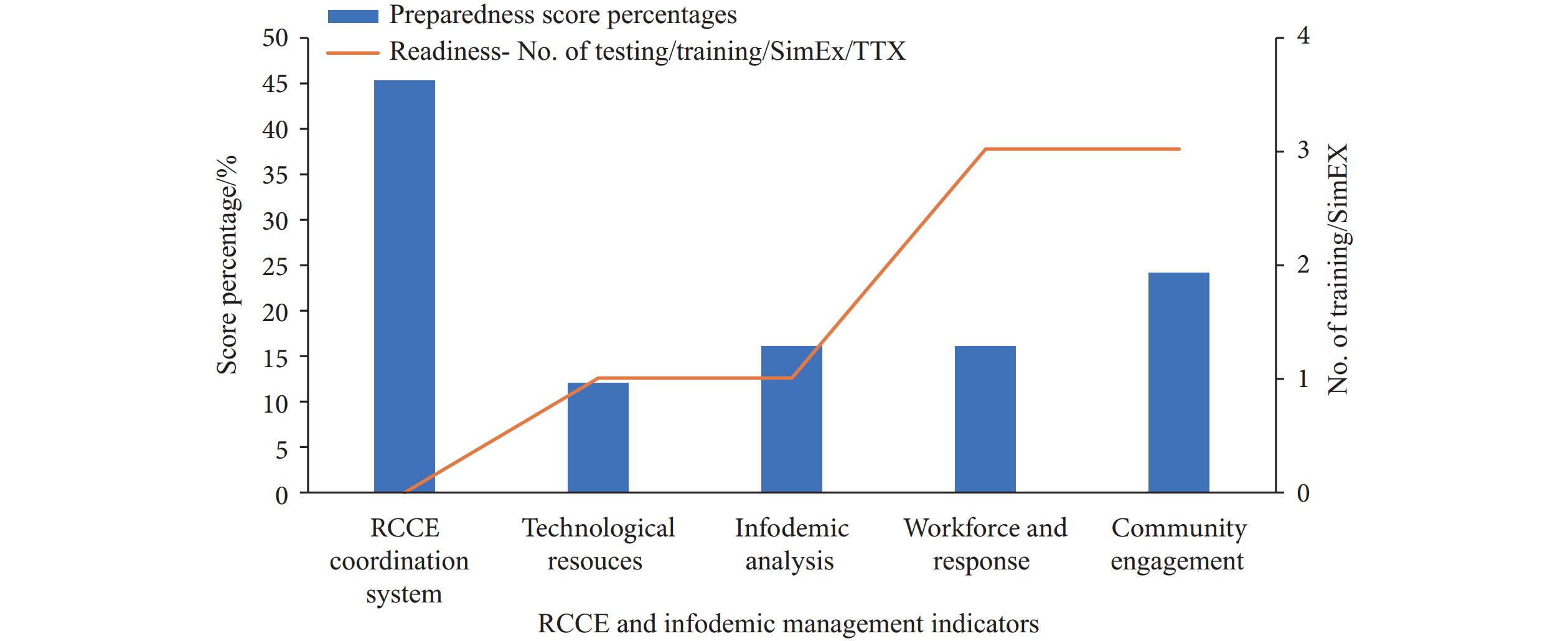 Figure 1.
Figure 1.Indicator-wise risk communication and community engagement preparedness status of health department in Khyber Pakhtunkhwa.
Note: This bar graph illustrates the preparedness and readiness scores for the Khyber Pakhtunkhwa Health Department across various risk communication and community engagement indicators. The y-axis shows achievement scores as percentages (0–100%), while the x-axis displays the different indicators of risk communication and infodemic management capacities and capabilities.The health department’s infodemic analysis and risk assessment capabilities showed significant limitations. While traditional methods were employed for infodemic analysis, achieving a 40% score for rumor verification, sentiment analysis implementation remained minimal at 20%. Only 20% of staff received training in infodemic surveillance and analysis (Figure 1 and Figure 2).
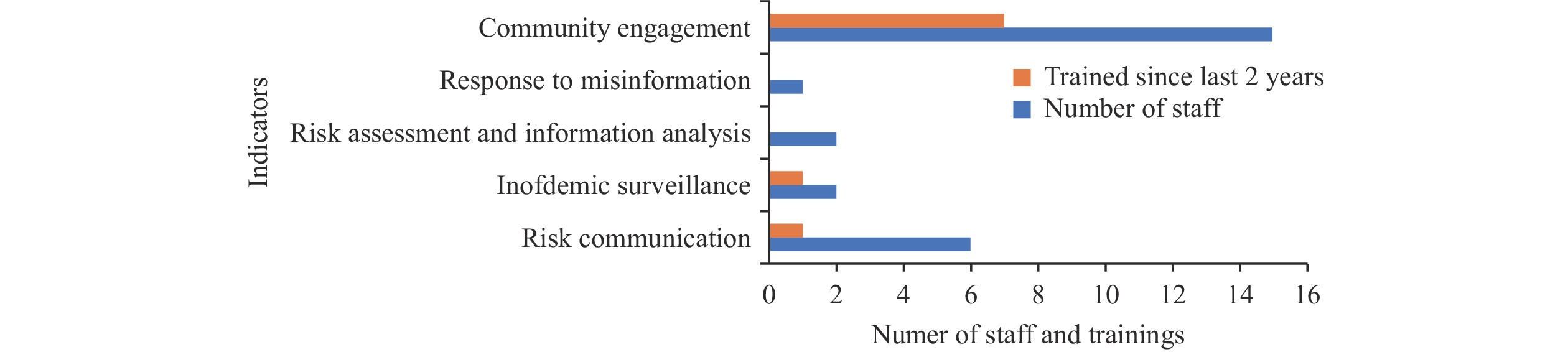 Figure 2.
Figure 2.Workforce capacity and capability of Khyber Pakhtunkhwa Health Department for infodemic management.
Note: This bar graph depicts the workforce capacity and capabilities of the Khyber Pakhtunkhwa Health Department for infodemic management. The y-axis quantifies staffing levels, capacity building initiatives, and training completion rates, while the x-axis presents key indicators related to workforce competencies and infodemic management practices.Assessment of the workforce and response system revealed several areas requiring enhancement. Although the department maintains dedicated personnel for risk communication, infodemic surveillance, and community engagement, other metrics indicated substantial weaknesses. Notably, staff training exercises in infodemic surveillance and management were conducted infrequently, achieving only a 20% implementation rate (Figure 1).
Community engagement emerged as a relative strength within the health department’s capabilities. The department maintained a moderate social media community engagement system (40%) and conducted numerous community awareness and engagement sessions. The department demonstrated moderate capacity (40%) in executing community awareness and engagement initiatives, though partnerships with media and other agencies remained primarily informal (Figure 2).
Quantitative assessment revealed that 14 staff members were engaged in community outreach activities, while risk communication activities were supported by only 6 staff members. Response time analysis indicated concerning delays: 25 days for dengue-related misinformation detection and 30 days for cholera-related false information response. The department averaged 18.3 days to identify new misinformation threats and 6.6 days to implement responses (
Supplementary Figure S2 ). -
The findings of our study revealed both strengths and limitations in the Khyber Pakhtunkhwa Health Department’s capacity for RCCE and infodemic management. Notable strengths include an established RCCE coordination system, dedicated focal person designation, effective community engagement practices, and demonstrated leadership in crisis communication. However, significant gaps exist in technological infrastructure, workforce capacity, and infodemic analysis capabilities, indicating lower levels of preparedness. While some training initiatives have been implemented, there are substantial deficiencies in capacity testing, operational training, simulation exercises, and overall responsiveness to managing mis- and disinformation.
Our assessment identified critical challenges in the health department’s preparedness for managing misinformation during infectious disease outbreaks and public health emergencies. A key finding was the limited capacity for infodemic surveillance and monitoring, a common challenge among LMICs that have yet to develop systematic monitoring capabilities (1). The department’s technological infrastructure for online information monitoring and infodemic analysis remains inadequate. This observation aligns with research by Donelle et al., who identified insufficient investment in these tools as a significant barrier to effective health communication and emergency response (10).
Our analysis revealed that the health department predominantly relies on traditional methods and lacks adequately trained personnel for information flow monitoring, rumor management, and news verification. Current literature advocates for a paradigm shift toward modern information monitoring and infodemic management approaches, incorporating active social listening and digital analysis tools (11–12). The current situation results in significant delays — averaging 18.3 days for identifying and 6.6 days for responding to new misinformation and disinformation threats — highlighting the urgent need for enhanced workforce development, technological infrastructure, and capacity building. These findings are consistent with Purnat’s research emphasizing the critical importance of training health professionals in infodemic management strategies (13).
Community engagement emerged as a relative strength of the health department, demonstrated through effective utilization of social media platforms, community sessions, and strategic partnerships. This aligns with existing literature suggesting that sustained community engagement efforts are crucial for mounting timely responses to future outbreaks (14–15). The implementation of collaborative community engagement approaches can significantly enhance risk communication and infodemic management capabilities for emergency response.
This study’s scope was limited to Khyber Pakhtunkhwa, Pakistan, with input from only 19 subject matter experts and no community perspectives, potentially affecting its generalizability to the national level. The findings may not fully represent risk communication capacities across operational and tactical levels.
Our assessment identified critical gaps in infodemic management preparedness, particularly regarding technological resources, infodemic analysis methods, risk assessment protocols, response times, and community information sharing. While the existing RCCE coordination system and community engagement activities provide a valuable foundation, developing a comprehensive infodemic management strategy is essential. We recommend that the health department prioritize investments in enhanced technological infrastructure, implement robust health infodemic surveillance systems, adopt advanced analytical methods, increase trained personnel, and strengthen risk communication through active stakeholder engagement to effectively manage future public health emergencies.
-
The support of leadership and subject matter experts from the Health Department Khyber Pakhtunkhwa, Livestock Department KP, WHO country and provincial office Pakistan, UNICEF Pakistan office, and JSI KP office who participated in the study and shared documentation on preparedness and planning; the Deanship for Scientific Research, King Faisal University, Saudi Arabia for funding support; and the National IHR-2005 Focal Person of Pakistan at NIH for coordinating support of this study.
-
While this study did not involve human subjects research, as it focused on organizational and institutional preparedness for risk communication, ethical approval was obtained from the Ethics Review Board of the University of Haripur, Khyber Pakhtunkhwa, Pakistan.
HTML
| Citation: |

|