
 Download:
Download:




-
Introduction: The effective dose caused by the external exposure of medical radiation workers has dramatically declined in China. By contrast, less attention has been given to internal exposure to radiation. This study aimed to describe the national monitoring of the internal exposure of Chinese nuclear medicine (NM) workers from 2021 to 2023. These findings provide essential baseline data for enhancing radiation protection protocols in NM facilities and optimizing national internal exposure monitoring.
Methods: All the non-military hospitals in China with an NM program were investigated. Portable gamma spectrometers were used to measure the 131I activities of the thyroid of staff members at 131I treatment sites.
Results: A total of 998 hospitals in China had an NM program in 2023. Detectable rate (measurements above minimum detectable activity) decreased from 26.2% in 2021 to 20.1% in 2023. The proportion of measurements exceeding 1.0×102 Bq decreased from 12.8% in 2021 to 10.0% in 2023. The detectable rate varied with job categories (P=0.001), with the detectable rate of cleaners being the highest.
Conclusions: In China, 131I was detected in the thyroid of about one-fifth of the subjects working at radioiodine treatment sites. Detectable rate exhibited a slow downward trend in recent years.
-
The average annual external exposure doses for medical radiation workers in China have shown a significant decline from 1.4 mSv (1996–2000) (1) to 0.35 mSv (2016) (2). However, beyond external exposure, nuclear medicine (NM) workers face additional risks from potential internal contamination due to their work with unsealed radiopharmaceuticals (3). Among these radionuclides, 131I presents the primary internal exposure risk due to its high volatility and extended half-life.
This study aimed to assess internal exposure levels among NM staff across various hospitals to inform the development of evidence-based management and employee protection strategies. Following pilot measurements of 131I internal exposure in NM workers from 2018 to 2020, the study expanded to include 29 provincial-level administrative divisions (PLADs) from 2021 to 2023 (131I monitoring was not conducted in Shanxi in 2023). We present a comprehensive analysis of 131I treatment practices across China and evaluate thyroid 131I activity levels among staff at radioiodine treatment facilities during this period. The findings are intended to provide an empirical foundation for enhancing radiation protection protocols for personnel working at radioiodine treatment facilities throughout China.
This study comprised two main components. First, information about NM hospitals was collected through questionnaires, encompassing all non-military hospitals in China with NM programs. Second, portable gamma spectrometers were calibrated using 131I standard sources at our institution for thyroid activity measurements. The calibrated equipment was used to measure 131I activities in the thyroid of selected staff members at 131I treatment facilities. A standardized measurement and calculation protocol was developed into a handbook and disseminated through training to detection institutions. The detector was consistently positioned in contact with either the neck or thigh (for background measurement), with a measurement duration of 120 s. Minimum detectable activity (MDA) was employed to characterize the gamma spectrometer’s capability in quantifying radionuclide presence. The detailed methodology for calculating thyroid 131I activity and MDA has been previously published (4). All data were uploaded through the National Radiological Health Information Platform and analyzed using Microsoft Excel 2016 (Microsoft Corporation, Redmond, WA., USA) and SPSS software (version 20.0; IBM, Armonk, USA). Statistical significance was defined as a two-sided P<0.05.
In 2023, China had 998 hospitals with NM programs, employing 11,285 workers across all PLADs except Xizang Autonomous Region. Of these institutions, 637 (63.8%) hospitals with 8,818 NM workers conducted 131I treatment procedures, and 358 (35.9%) hospitals with 5,893 workers specifically performed 131I treatment for thyroid cancer. Surface contamination monitors were available in 906 (90.8%) hospitals. Among the 637 hospitals providing 131I treatment, 62.6% were equipped with automated 131I loading devices (
Supplementary Table S1 ).National internal exposure monitoring of staff at radioiodine treatment sites commenced in 2021. Table 1 presents the comprehensive monitoring results from 2021 to 2023. The number of monitored hospitals increased from 255 in 2021 to 405 in 2023, with participating staff members rising from 1,884 to 3,137. Both the detectable rate (measurements above MDA) and the proportion of measurements exceeding 1.0×102 Bq have showed a consistent decline since 2021.
Year PLADs numbers Hospitals numbers Participants numbers Detectable rate (%) Maximum 131I thyroid activity (Bq) Proportion of measurements above 1.0×102 Bq (%) 2021 22 255 1,884 26.2 4.4×104 12.8 2022 20 287 2,210 21.7 2.9×104 11.3 2023 29 405 3,137 20.1 5.8×104 10.0 Note: Military hospitals are not included in this study.
Abbreviation: PLADs=provincial-level administrative divisions.Table 1. Measurements of 131I activities in the thyroid of staff members at radioiodine treatment sites in China, 2021–2023.
In 2023, thyroid 131I activity measurements were conducted on 3,137 staff members from radioiodine treatment sites across 29 PLADs (
Supplementary Table S2 ). 131I was detected in the thyroid of 630 participants (20.1%), with the maximum measurement reaching 5.8×104 Bq. Further evaluation was performed on measurements exceeding 1.0×102 Bq, which represented 10.0% of all participants.Analysis revealed no significant gender-based differences in detectable rates (P=0.443). However, operators exhibited a significantly higher detectable rate (25.7%) compared to nonoperators (18.2%) (P<0.001). Detectable rates varied significantly across job categories (P=0.001). Notably, cleaners, despite not directly operating 131I equipment, demonstrated the highest detectable rate, followed by nurses. Detailed distributions are presented in Table 2.
Item Participants
numbersAbove MDA P Numbers Proportion
(%)Gender 0.443 Male 1,372 267 19.5 Female 1,765 363 20.6 131I operation <0.001 No 2,186 397 18.2 Yes 908 233 25.7 Job 0.001 Cleaners 156 44 28.2 Nurses 806 190 23.6 Doctors 1,273 241 18.9 Others 140 25 17.9 Technicians 762 130 17.1 Note: Others include physicists, chemists and pharmaceutical engineers. In 2023, thyroid 131I activity measurements were conducted on 3,137 staff members, but the information on 131I operation for 43 subjects is missing. 131I was detected in the thyroids of 630 participants (20.1%).
Abbreviation: MDA=minimum detectable activity.Table 2. Distribution of the participants above MDA in different groups.
Among the 908 participants who had operated 131I during the previous year, 899 provided data regarding their most recent 131I operation timing. Analysis of the relationship between measurement timing and detectable rates revealed a clear temporal pattern (Figure 1). The highest detectable rate of 47.4% occurred when measurements were performed on the same day as 131I operations. This rate decreased significantly to 31.6% after just one day and continued to decline progressively with increasing time intervals (P<0.001).
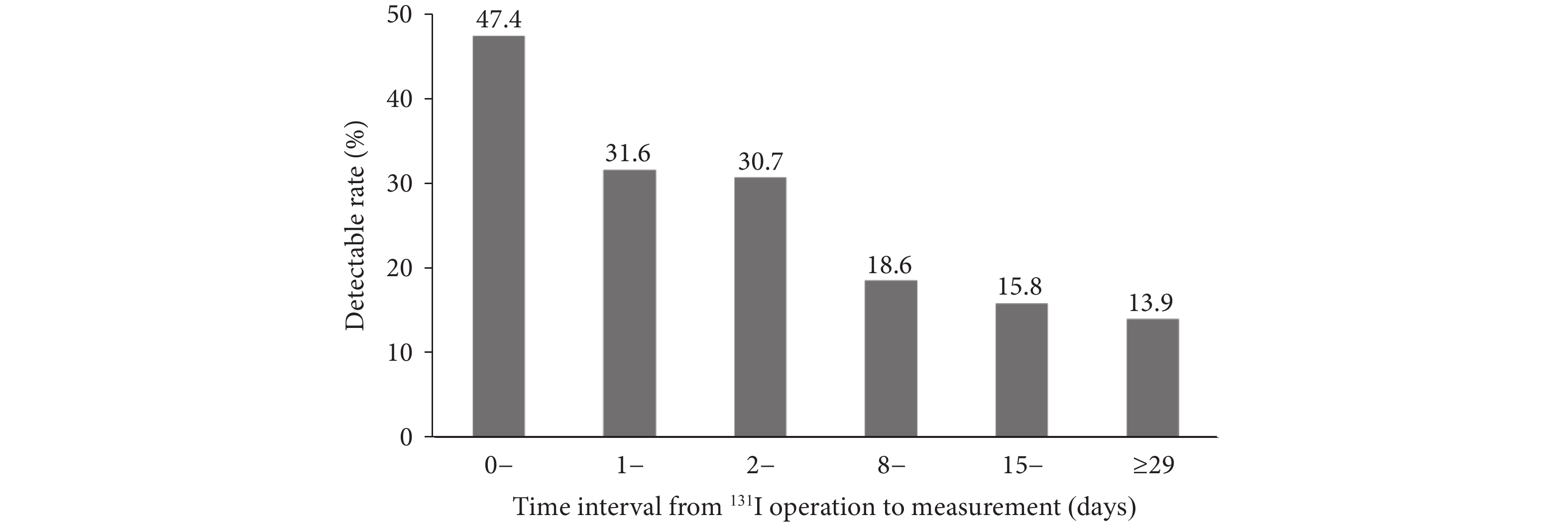 Figure 1.
Figure 1.Detectable rate of different time intervals from 131I operation to measurement in 2023.
Note: A total of 899 measurements are shown in this figure, because the time intervals from 131I operation to measurement for 8 subjects are missing. Linear-by-linear association chi-squared test suggested that the trend of detectable rate exhibited statistical significance (P<0.001). -
Our analysis revealed that 998 hospitals in China, employing 11,285 staff members, maintained NM programs in 2023. Approximately two-thirds of these NM facilities provide 131I treatment services, while one-third specifically conduct 131I treatment for thyroid cancer. The latter requires substantially higher radioiodine doses compared to hyperthyroidism treatment protocols.
Despite a gradual decline in detectable rates from 2021 to 2023, 131I was still detected in the thyroids of approximately one-fifth of workers at radioiodine treatment sites. This detectable rate falls between those reported in previous studies, being lower than the approximately 30% observed in Polish research (5) but higher than the 15% reported in Korean investigations (6). These variations may be attributed to differences in 131I exposure frequency and radiation protection protocols across countries.
The detectable rate exhibits substantial provincial variation, which may be attributed to differences in radiation protection protocols and sample sizes. Provinces with higher detectable rates require enhanced attention to internal contamination monitoring of nuclear medicine workers. Our stratified analysis revealed that nuclear medicine operators had significantly higher detectable rates compared to nonoperators. Furthermore, we identified a negative correlation between the time interval from operation to detection and the detectable rate.
Notably, cleaners exhibited the highest detectable rate among all nuclear medicine workers, despite not directly operating equipment. This elevated risk stems from their prolonged exposure during the cleaning of radioiodine treatment sites, combined with inadequate personal radiation protection (7). The high detectable rate among cleaners likely results primarily from insufficient awareness of self-protection protocols, highlighting the need for enhanced radiation protection training in nuclear medicine facilities. Implementation of basic protective measures, such as wearing charcoal masks and medical rubber gloves, can significantly reduce 131I intake through inhalation and ingestion. The relatively uniform detectable rates observed among other worker categories may be attributed to varied patterns of 131I handling, as all workers except cleaners regularly engage in direct 131I manipulation.
While our findings suggest that increasing the intervals between 131I operations could reduce radiation exposure risk, excessive extension of these intervals may prove counterproductive. Prolonged periods between operations could lead to degradation of technical skills, potentially increasing the risk of radioactive contamination. Therefore, establishing optimal rotation schedules for 131I operations should be a key consideration in daily operational protocols.
This study had a notable limitation regarding the variability in MDA and measurement uncertainty across different monitoring institutions due to the use of diverse portable gamma spectrometers. To enable meaningful comparisons of measurements across PLADs, we standardized the analysis by calculating the proportion of measurements exceeding 1.0×102 Bq, as all MDAs were below this threshold. Future monitoring efforts should prioritize the standardization of gamma spectrometry equipment. Additionally, occupational radiation dose assessment should incorporate both external exposure and committed doses from radionuclide intake during the same period (8). However, committed doses from internal exposure were not estimated as measurements were conducted only once per year. This limitation arises from the restricted availability of internal exposure monitoring capabilities, with only approximately 70 qualified institutions nationwide. Switzerland’s approach of using screening measurements performed by local staff with their own instrumentation offers an economical and practical alternative (9). In future work, we aim to develop a scientific and economic routine monitoring program to accurately assess the committed effective doses of NM workers.
The national screening program conducted over the past three years has yielded valuable data on thyroid 131I levels among NM workers and their provincial distribution patterns. Through detailed analysis, we identified key factors contributing to elevated detectable rates. These findings provide an essential scientific foundation for enhancing radiation protection protocols in NM facilities and optimizing national internal exposure monitoring systems.
-
The authors gratefully acknowledge the support provided by the Core Competence Training Program of Epidemiology and Health Statistics, Chinese Center for Disease Control and Prevention.
-
Received ethics approval from the Institutional Ethics Committee of the National Institute for Radiological Protection, Chinese Center for Disease Control and Prevention (No.LLSC2020-006).
HTML
| Citation: |

|