
 Download:
Download:




-
Objective: To investigate the prevalence and severity of menopausal symptoms among Chinese women aged 40–60 years and provide evidence for developing personalized health management strategies.
Methods: Using a multi-stage stratified cluster sampling approach, we conducted a nationwide cross-sectional survey across representative provincial-level administrative divisions (PLADs) and prefecture-level cities, encompassing 26 district/county survey sites. The questionnaire collected information on demographic characteristics, menopausal status, and symptoms. Data analysis employed means and standard deviations (X±S) or rates and proportion ratios to describe menopausal symptom occurrence, with group differences analyzed using Mann-Whitney or Kruskal-Wallis tests.
Results: The study included 42,304 women with a mean age of 49.9±5.7 years. The overall prevalence of menopausal symptoms was 46.3% [95% confidence interval (CI): 45.8%, 46.7%], predominantly mild to moderate in severity. The prevalence of mild to severe symptoms began increasing in women over age 44, peaking at age 52. Moderate to severe symptoms showed an uptick after age 46, also peaking at 52 years, while severe symptoms increased after age 48, reaching maximum prevalence at age 56. The most commonly reported symptoms were insomnia (50.0%, 95% CI: 49.5%, 50.5%), fatigue (48.2%, 95% CI: 47.7%, 48.7%), and nervousness (46.9%, 95% CI: 46.5%, 47.4%). Significant differences in symptom severity between premenopausal and postmenopausal women were observed in the 45–49 (P<0.001) and 50–54 (P=0.019 <0.05) age groups.
Conclusions: The study revealed distinct patterns in the prevalence, severity, and manifestation of menopausal symptoms across different age groups in China. The age-related progression of symptoms provides a scientific foundation for developing targeted healthcare interventions for women at various stages of menopause.
-
Menopause represents a critical transitional phase in the female life cycle, characterized by the progressive decline of ovarian function from peak activity to complete cessation. This transition typically occurs between ages 40 and 60 years, encompassing the periods before, during, and after menopause (1). During this transition, women may experience a diverse array of physical, mental, and psychological manifestations associated with decreased ovarian function and fluctuating estrogen levels. The severity and duration of symptoms exhibit considerable individual variation, generally persisting for 3 to 5 years (2). Both domestic and international research demonstrates a high prevalence of menopausal symptoms, albeit with notable population-specific variations (3–5). However, existing domestic research is limited by small sample sizes, inadequately defined age ranges, and regional specificity, which compromises the generalizability of findings (6–7).
This study derives from The Epidemiological Investigation of Menopause Status among Chinese Women (EIM-CW), a nationwide epidemiological survey conducted from August 2023 to February 2024. The study population comprised non-pregnant women aged 40–60 years who were either local residents or had maintained residence in the area for more than 6 months, excluding those with congenital absence of the uterus or history of premenopausal hysterectomy. The investigation employed a multi-stage stratified cluster sampling method to select representative provincial-level administrative divisions (PLADs) and prefecture-level cities nationwide. To ensure comprehensive representation across eastern, central, and western regions, the following locations were selected: Hebei Province (Tangshan City), Inner Mongolia Autonomous Region (Chifeng City), Liaoning Province (Shenyang and Dalian cities), Jiangsu Province (Wuxi City), Zhejiang Province (Ningbo City), Shandong Province (Jinan City), Henan Province (Luoyang City), Hubei Province (Xiangyang City), Guangxi Zhuang Autonomous Region (Liuzhou City), Sichuan Province (Meishan City), Shaanxi Province (Baoji City), and Gansu Province (Zhangye City). Sample allocation was proportional to provincial populations, with selected cities further stratified into urban and rural areas, yielding 26 district/county survey sites. From each site, two streets and two townships were randomly selected. Cluster sampling was then implemented to include all eligible female residents aged 40–60 years within the selected streets and townships.
Data collection was conducted through the custom-developed Chinese Women’s Health Survey Platform, which incorporated a questionnaire covering demographic characteristics, menopausal status, and symptoms. The severity of menopausal symptoms was evaluated using a modified Kupperman scale, a validated tool widely used to assess menopausal symptoms. The scale utilized four severity levels: zero (normal, score=0), occasional (mild, score=1), persistent (moderate, score=2), and affecting life (severe, score=3). Symptom indices were weighted according to clinical significance: hot flushes and sweating received a score of 4; paresthesia, insomnia, nervousness, sexual complaints, and urinary tract infections received a score of 2; and melancholia, vertigo, fatigue, arthralgia/myalgia, headache, heart palpitations, and formication were assigned a score of 1. The total symptom score was calculated by multiplying the basic score by the severity score, yielding a possible range of 0 to 63 points. Based on the modified Kupperman scale, scores were categorized as follows: 6 or less indicated normal symptoms, 7 to 15 indicated mild symptoms, 16 to 30 indicated moderate symptoms, and scores exceeding 30 indicated severe symptoms, with higher total scores reflecting greater symptom severity.
Statistical analyses were performed using IBM SPSS (version 26.0, IBM Corp., New York, USA). Qualitative data were described using rates and proportion ratios, while quantitative data were reported as means and standard deviations (X±S). Group differences were analyzed using Mann-Whitney and Kruskal-Wallis tests, with statistical significance set at α=0.05.
The study included 42,304 women with a mean age of 49.9±5.7 years, comprising 23,475 (55.5%) premenopausal and 18,829 (44.5%) postmenopausal women, with the latter group having a mean age of 49.4±3.3 years. A total of 19,570 women reported menopausal symptoms, yielding an overall prevalence rate of 46.3% [95% confidence interval (CI): 45.8%, 46.7%]. Mild symptoms were most common (31.0%), followed by moderate symptoms (14.3%), while severe symptoms were relatively rare (1.0%). Analysis of menopausal symptom severity across different sociodemographic characteristics revealed statistically significant differences (P<0.001) among women of varying age groups, ethnicities, occupations, regions, educational levels, and marital status (Table 1).
Characteristic Total
n ( %)Severity of menopausal symptoms
n (%)H/U P Normal
22,734 (53.7)Mild
13,096 (31.0)Moderate
6,053 (14.3)Severe
421 (1.0)Age group (years) 40–44 9,363 (22.1) 5,290 (56.5) 2,961 (31.6) 1,052 (11.2) 60 (0.6) 45–49 10,445 (24.7) 5,623 (53.8) 3,257 (31.2) 1,470 (14.1) 95 (0.9) 90.7* <0.001 50–54 11,951 (28.3) 6,172 (51.6) 3,675 (30.8) 1,962 (16.4) 142 (1.2) 55–60 10,545 (24.9) 5,649 (53.6) 3,203 (30.4) 1,569 (14.9) 124 (1.2) Nation (51.8×106)† <0.001 Han 39,441 (93.2) 20,997 (53.2) 12,297 (31.2) 5,754 (14.6) 393 (1.0) Minority 2,863 (6.8) 1,737 (60.7) 799 (27.9) 299 (10.4) 28 (1.0) Occupation 1108.1* <0.001 Farmer (forest, grazing, fishing) 10,963 (25.9) 6,860 (62.6) 2,779 (25.3) 1,242 (11.3) 82 (0.7) Worker 5,468 (12.9) 3,228 (59.0) 1,538 (28.1) 668 (12.2) 34 (0.6) Government/institutions 1,535 (3.6) 708 (46.1) 578 (37.7) 237 (15.4) 12 (0.8) Technical staff 1,533 (3.6) 749 (48.9) 534 (35.4) 221 (14.4) 20 (1.3) Business/service worker 2,753 (6.5) 1,511 (54.9) 899 (32.7) 333 (12.1) 10 (0.4) Individual/private business 2,340 (5.5) 1,355 (57.9) 672 (28.7) 293 (12.5) 20 (0.9) Teacher/soldier 1,324 (3.1) 516 (39.0) 510 (38.5) 271 (20.5) 27 (2.0) Medical worker 5,113 (12.1) 1,960 (38.3) 2,115 (41.4) 982 (19.2) 56 (1.1) Housewife 9,793 (23.1) 5,234 (53.4) 2,882 (29.4) 1,537 (15.7) 140 (1.4) Other 1,482 (3.5) 613 (41.4) 580 (39.1) 269 (18.2) 20 (1.3) Region (20.1×107)† <0.001 Urban (District) 20,708 (49.0) 10,173 (49.1) 6,853 (33.1) 3,441 (16.6) 241 (1.2) Rural (County) 21,596 (51.0) 12,561 (58.2) 6,243 (28.9) 2,612 (12.1) 180 (0.8) Education level 879.6* <0.001 Less than primary 6,990 (16.5) 3,865 (55.3) 1,863 (26.7) 1,145 (16.4) 117 (1.7) Junior secondary 16,845 (39.8) 10,095 (59.9) 4,664 (27.7) 1,949 (11.6) 137 (0.8) Senior secondary 8,304 (19.6) 4,598 (55.4) 2,544 (30.6) 1,105 (13.3) 57 (0.7) University 9,833 (23.2) 4,024 (40.9) 3,892 (39.6) 1,809 (18.4) 108 (1.1) Master and above 332 (0.8) 152 (45.8) 133 (40.1) 45 (13.6) 2 (0.6) Marital status (32.2×106)† <0.001 Married 40,393 (95.5) 21,981 (54.4) 12,376 (30.6) 5,661 (14.0) 375 (0.9) Unmarried/divorced/widowed 1,911 (4.5) 753 (39.4) 720 (37.7) 392 (20.5) 46 (2.4) Note: Numbers outside parentheses represent frequencies; numbers inside parentheses represent percentages (%).
*Kruskal-Wallis H test.
† Mann-Whitney U test.Table 1. Sociodemographic characteristics and severity of menopausal symptoms in 42,304 women.
The analysis showed that 44.7% (10,496 of 23,475) of premenopausal women and 48.2% (9,074 of 18,829) of postmenopausal women experienced mild to severe menopausal symptoms. The Mann-Whitney test revealed significantly greater symptom severity among premenopausal women compared to postmenopausal women (P<0.001). Further analysis of symptom severity variations across age groups and menopausal status demonstrated significant differences between premenopausal and postmenopausal women in the 45–49 (P<0.001) and 50–54 (P=0.019 <0.05) age groups (Figure 1).
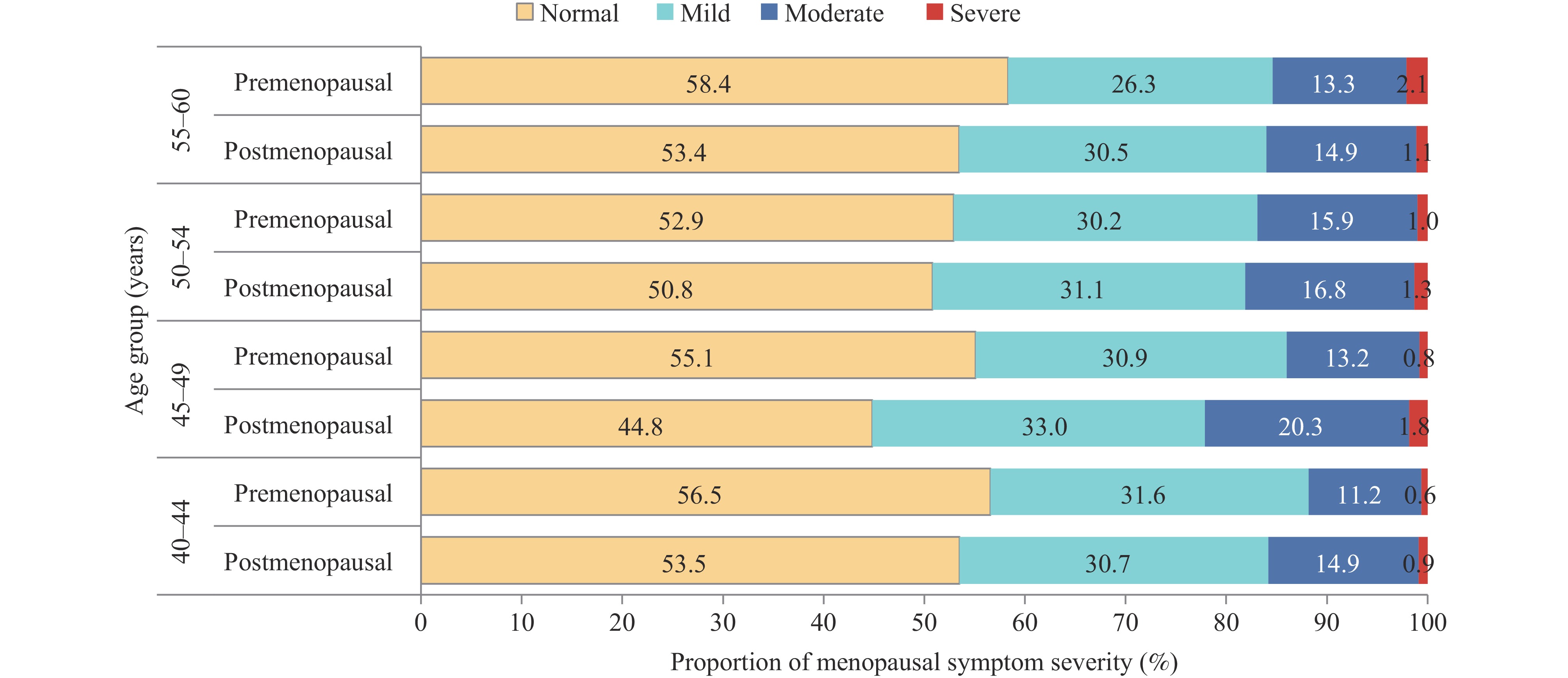 Figure 1.
Figure 1.Severity of menopausal symptoms in women with different menopausal status across age groups.
Analysis by age group revealed that the prevalence of mild to severe menopausal symptoms began increasing in women over 44 years, reaching its peak at age 52 (49.8%, 95% CI: 47.9%, 51.8%). Moderate to severe symptoms showed an uptick in women over age 46, also peaking at 52 years (19.1%, 95% CI: 17.6%, 20.6%). Severe symptoms began increasing in women over age 48, with prevalence reaching its maximum at age 56 (1.6%, 95% CI: 1.0%, 2.1%; Figure 2A).
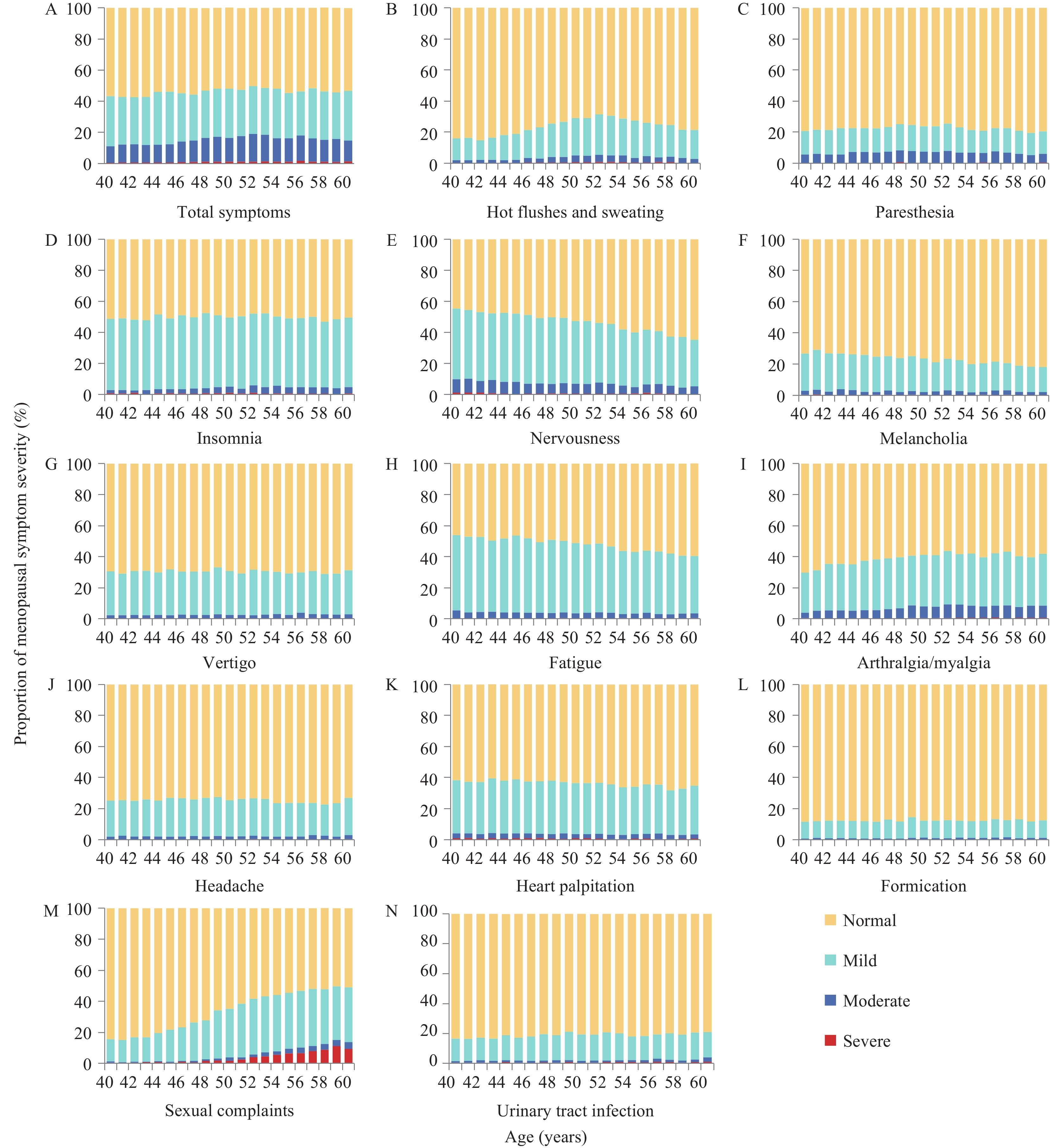 Figure 2.
Figure 2.Severity of total and 13 menopausal symptoms in women of different age groups. (A) Total symptoms; (B) Hot flushes and sweating; (C) Paresthesia; (D) Insomnia; (E) Nervousness; (F) Melancholia; (G) Vertigo; (H) Fatigue; (I) Arthralgia/myalgia; (J) Headache; (K) Heart palpitation; (L) Formication; (M) Sexual complaints; (N) Urinary tract infection.
The most frequently reported menopausal symptoms were insomnia (50.0%, 95% CI: 49.5%, 50.5%), fatigue (48.2%, 95% CI: 47.7%, 48.7%), and nervousness (46.9%, 95% CI: 46.5%, 47.4%). Figure 2 illustrates the severity distribution of total menopausal symptoms and 13 specific symptoms across different age groups. Hot flushes and sweating affected 23.9% (95% CI: 23.5%, 24.3%) of women across all age groups, with prevalence increasing from age 40, peaking at age 52, and subsequently declining (Figure 2B). In contrast, the prevalence of nervousness, melancholia, and fatigue demonstrated an age-related decline (Figure 2E, 2F, and 2H). Notably, melancholia prevalence decreased from 29.2% at age 41 to 18.1% at age 60. Women under 50 exhibited higher rates of fatigue and neuropsychiatric symptoms, with fatigue exceeding 50% in women younger than 50 years and nervousness predominating in those under 47 years. Conversely, arthralgia/myalgia, sexual complaints, and urinary tract infections showed increasing prevalence with age, with sexual complaints demonstrating the most pronounced change, followed by arthralgia/myalgia (Figure 2I, 2M, and 2N).
-
This study represents the first comprehensive cross-sectional investigation of menopausal symptoms among community-dwelling women in China. We provide robust evidence regarding the prevalence and severity of menopausal symptoms in Chinese women aged 40–60 years. Our findings reveal significant variations in the prevalence, severity, and manifestation of menopausal symptoms across different age groups in the Chinese population. Previous research has documented that the prevalence of moderate to severe menopausal symptoms reaches 29.8% among perimenopausal women in Greece (3), while a study in Shanghai Municipality reported a prevalence of 73.8% among women aged 40–60 years (4). Our observed prevalence was lower than that reported in Shanghai, and the occurrence of moderate to severe symptoms was less frequent than in Greek women. The elevated prevalence in Shanghai may be attributed to the city’s intense urban lifestyle and occupational stress, which could adversely affect women’s physical and mental well-being. Additionally, genetic variations among populations likely play a crucial role in symptom manifestation, while methodological differences in sampling, data collection, and analysis may contribute to the observed disparities across studies. Understanding age-specific symptom patterns enables the development of targeted early prevention strategies and more effective health education initiatives, facilitating the implementation of age-appropriate public health interventions.
The study reveals distinct patterns in menopause symptoms between premenopausal and postmenopausal women, with a notably higher prevalence in the latter group (48.2%). Our analysis of how menopausal status influences symptom severity across age groups revealed particularly significant differences among women aged 45–49 years and 50–54 years — periods approaching natural menopause — further substantiating the relationship between menopausal status and symptom intensity. Research indicates that women experiencing premature ovarian failure report both a higher prevalence and greater severity of symptoms compared to those undergoing natural menopause (8).
Our findings reveal that the severity of menopausal symptoms exhibits distinct age-related patterns among women aged 40–60 years. A notable inflection point occurs at age 44, marking a significant increase in mild to severe symptoms. This timing likely corresponds to critical physiological changes, particularly an accelerated decline in ovarian function that leads to substantial hormonal fluctuations affecting endometrial integrity, bone metabolism, and cardiovascular function. The prevalence of moderate and severe climacteric symptoms reaches its peak at age 52, while severe symptoms demonstrate maximum prevalence at age 56. This temporal pattern may be attributed to the increasing prevalence of comorbid chronic conditions such as hypertension, diabetes, and cardiovascular disease with advancing age (9), which potentially exacerbate symptom severity during the 52–56 year age range. These findings suggest that enhanced clinical screening and therapeutic interventions should be targeted toward women in this age group.
Our analysis identified insomnia, fatigue, and nervousness as the predominant menopausal symptoms among women aged 40–60 years. This symptom profile differs from findings in other populations, such as the southwestern United States, where fatigue, musculoskeletal pain, and headaches were most prevalent among women aged 40–65 years (5). Similarly, surveys in Beijing reported bone and joint muscle pain, fatigue, and insomnia as primary symptoms (6), while Guangzhou residents predominantly experienced insomnia, fatigue, and headaches (7). These regional variations likely reflect the influence of cultural factors, lifestyle differences, and disparities in healthcare resource accessibility. Notably, fatigue consistently emerges as a leading symptom across multiple studies, potentially reflecting the fundamental alterations in energy metabolism and physiological function that characterize the menopausal transition.
Hot flushes and sweating, the primary manifestations of vasomotor symptoms in menopausal women, typically peak within 6 months after menstruation cessation and generally resolve within 1–2 years post-menopause. This study found that 23.9% of surveyed women reported experiencing hot flushes and sweating, a notably lower prevalence compared to other countries. For instance, moderate to severe vasomotor symptoms affect 40% of Greek women(3). The prevalence of vasomotor symptoms varies considerably across European countries, ranging from 31% in France to 52% in Italy (10). These differences may be attributed to genetic variations across ethnic groups affecting hormonal sensitivity during menopause. Notably, these symptoms peak among 52-year-old Chinese women, approximately 2–3 years post-menopause, suggesting this period warrants targeted interventions and medical management as needed.
This study has two primary limitations. First, the modified Kupperman score, being a self-report measure, may be subject to varying interpretations among menopausal women participating in the survey. Second, the cross-sectional design inherently limits the establishment of causal relationships between menopausal symptoms and their potential contributing factors. Future research should incorporate longitudinal cohort studies to analyze the factors influencing menopausal symptoms across different age groups and explore effective intervention strategies.
In conclusion, this nationally representative cross-sectional survey reveals a significant prevalence of menopausal symptoms among Chinese women, with notable variations in both severity and prevalence across different age groups. The comprehensive findings provide a robust scientific foundation for developing targeted healthcare strategies tailored to women at various stages of menopause. These insights hold substantial public health implications for alleviating menopausal symptoms and promoting the holistic well-being of women during their menopausal transition.
-
All study participants and staff members at the 26 survey sites for their dedicated efforts in data collection.
-
Received approval from the Ethics Review Committee of the National Center for Women and Children’s Health, China CDC (approval number: FY2022-14), with informed consent obtained from all participants.
HTML
| Citation: |

|