Download:
Download:




-
Congenital hearing loss represents a critical public health challenge, affecting 1 to 3 per 1,000 neonates in the general population (1), with prevalence rates escalating to 2% to 4% among those with established risk factors (2). Early-onset hearing impairment significantly impacts speech and language development. Without early intervention, congenital hearing loss frequently progresses to profound deafness, leading to substantial learning difficulties and emotional and social developmental challenges (3-4). However, when detection, diagnosis, intervention, and rehabilitation are implemented early, individuals with hearing impairment can achieve developmental outcomes comparable to their normal-hearing peers, facilitating social integration and reducing both familial and societal burden.
Universal Newborn Hearing Screening (UNHS) has emerged as the most effective strategy for early detection of congenital hearing loss (5). While some developed nations have achieved UNHS screening rates as high as 97.7% (6), the global landscape reveals significant disparities. Only 41 countries have attained coverage exceeding 85%, while at least 64 countries report coverage rates below 1% (7). As UNHS systems mature, an increasing number of hearing-impaired children receive timely interventions, enabling their integration into mainstream educational settings rather than specialized institutions. This shift in mainstream school enrollment patterns reflects various social, economic, and educational reforms, corresponding to UNHS development and serving as an indicator of intervention outcomes.
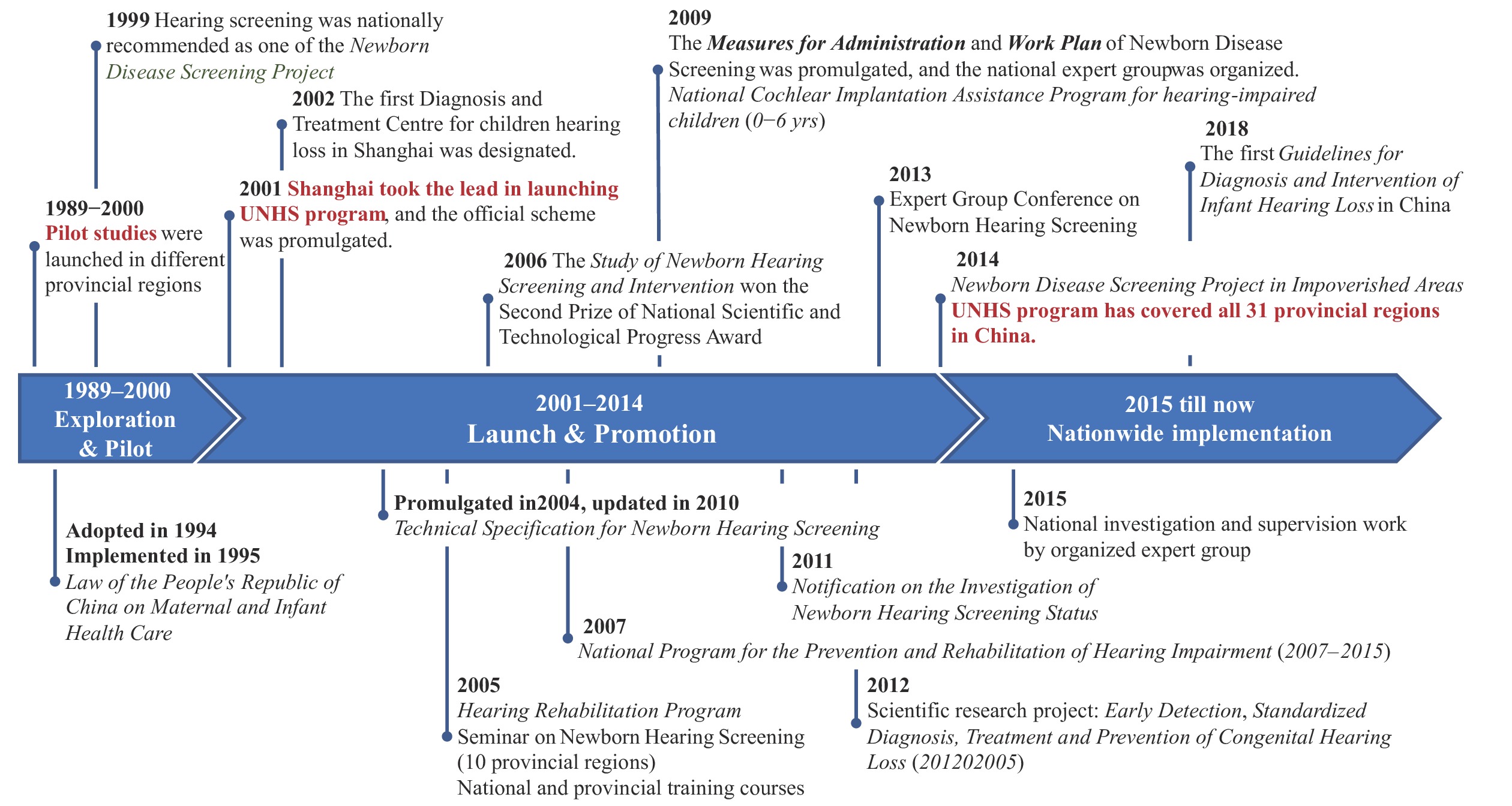
China, as a developing nation with one of the world’s largest populations, has made remarkable progress in UNHS coverage through sustained governmental initiatives over two decades. The country established its first national technical specification for newborn hearing screening in 2004, followed by the launch of a targeted national newborn disease screening project in 2014 to enhance screening rates in economically disadvantaged regions (
Supplementary Figure S1 ). This study examines the policy implementation and practical outcomes of UNHS in China across the past two decades, with particular emphasis on resource equity, health impacts (including screening coverage and mainstream education integration of hearing-impaired students), and future challenges. The insights gained from this experience may prove valuable for similar healthcare contexts globally.This study encompassed 31 provincial-level administrative divisions (PLADs), excluding Hong Kong Special Administrative Region (SAR); Macau SAR; and Taiwan, China, due to data unavailability. Data on the UNHS program were collected in 2021 through questionnaires distributed to 31 provincial health committees by the National Health Commission (NHC) of China. Educational data were obtained from the Ministry of Education (MOE) of China website (http://www.moe.gov.cn/jyb_sjzl/moe_560/). The study received approval from the ethics committee of Shanghai Ninth People’s Hospital Shanghai Jiao Tong University (SH9H-2022-T377-1).
-
China initiated the UNHS program in the late 1990s, achieving comprehensive coverage across all PLADs by 2014. According to the National Center for Birth Defects Monitoring of China, national coverage increased substantially from 29.9% in 2008 to 86.5% in 2016 (8). The program’s development can be categorized into three distinct phases: the exploration and pilot stage (1989–2000), the launch and promotion stage (2001–2014), and the nationwide implementation stage (2015-present) (Supplementary Figure S1).
The Chinese UNHS protocol follows a two-step screening process: initial screening after birth and repeat screening within 42 days. Distortion product otoacoustic emissions (DPOAE) serve as the primary screening method, followed by hearing diagnosis within 3 months, intervention within 6 months, and rehabilitation from 6 months to 6 years of age, culminating in enrollment for compulsory education for ages 6–14 (
Supplementary Figure S2 ). China’s compulsory education law, enacted in 1986, mandates nine years of schooling, encompassing elementary (grades 1–6) and middle school (grades 7–9). Educational options for hearing-impaired students include special education schools, attached classes, regular classes, and ’home delivery’ teaching (http://www.moe.gov.cn/). With UNHS implementation, an increasing number of hearing-impaired students now attend regular classes rather than special schools or classes. However, to our knowledge, the enrollment proportion among hearing-impaired students in China has not been previously documented in the literature. -
The Gini coefficient and Lorenz curve, well-established metrics for quantifying inequality, were employed to evaluate the distribution equity of healthcare services (including screening institutions and pediatric hearing diagnosis and treatment centers) and educational resources (including rehabilitation institutions and specialized schools for deaf-mutes) (Figure 1). Using each PLAD as an analytical unit, we conducted a nationwide equity assessment. The X-axis represents the cumulative proportion of births (in 2020, stratified by PLADs), while the Y-axis represents the cumulative proportion of corresponding resources.
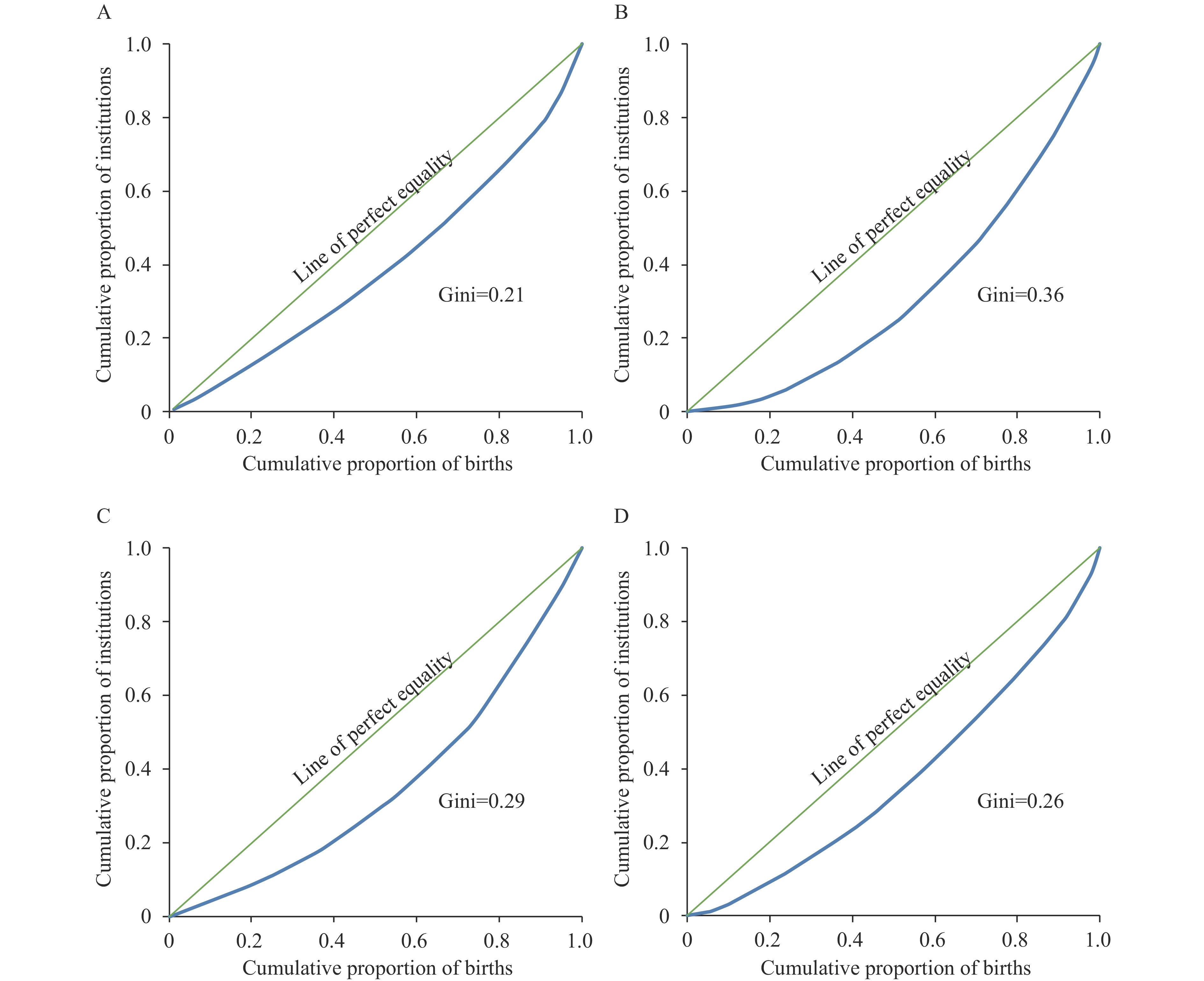 Figure 1.
Figure 1.Distribution of health services and educational resources in China, 2020. (A) Lorenz curve for hearing screening institutions; (B) Lorenz curve for hearing diagnosis and treatment centers; (C) Lorenz curve for rehabilitation institutions; (D) Lorenz curve for special schools.
Note: The green line represents perfect equality. The deviation between the two curves reflects the magnitude of inequality in resource distribution. The Gini coefficients are 0.21, 0.36, 0.29, and 0.26, respectively.The Gini coefficient ranges from 0 to 1, with higher values indicating greater inequality. Conventionally, coefficients below 0.2 indicate absolute equality, 0.2–0.3 relative equality, 0.3–0.4 adequate equality, 0.4–0.5 relative inequality, and above 0.5 severe inequality. Graphically, the coefficient represents the ratio between two areas: the area between the Lorenz curve (blue) and the line of perfect equality (green), and the total area beneath the line of perfect equality. A lower Gini coefficient indicates more equitable resource distribution relative to birth population across PLADs. As of 2020, China’s infrastructure comprised 14,648 screening institutions, 273 diagnosis and treatment centers, 865 hearing and speech rehabilitation institutions, and 389 special schools for deaf-mutes. The corresponding Gini coefficients were 0.21, 0.36, 0.29, and 0.26, respectively (Figure 1), indicating relative to adequate equality in resource distribution.
-
Screening coverage of Newborn Hearing Screening in China: Initial data collection in 2005 revealed that only nine PLADs reported newborn hearing screening cases, with a coverage rate of 10.9%. Following program implementation and promotion efforts, coverage expanded significantly, with 30 PLADs (excluding Xizang Autonomous Region) reporting data in 2010, achieving 37.8% newborn coverage. This rate subsequently increased substantially to 81.5% by 2015 (Figure 2,
Supplementary Table S1 ).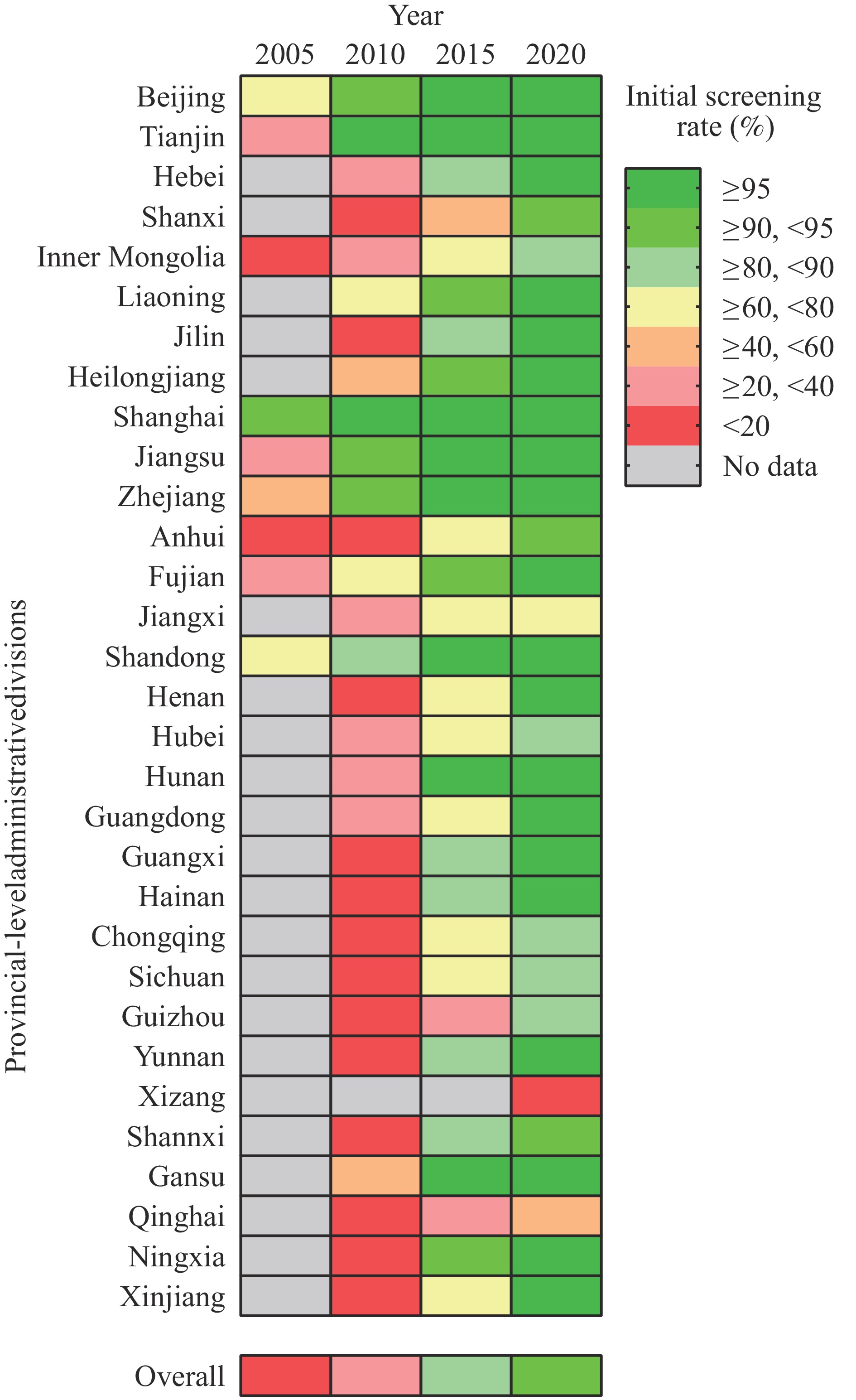 Figure 2.
Figure 2.Heat map of UNHS coverage across 31 PLADs in China for 2005, 2010, 2015, and 2020.
Note: Overall screening coverage rates for 2005, 2010, 2015, and 2020 were 10.9%, 37.8%, 81.5%, and 94.3%, respectively. The heat map employs a color gradient to represent screening rates across divisions, with green indicating higher coverage and red indicating lower coverage. Gray-shaded areas represent unavailable data.
Abbreviation: UNHS=Universal newborn hearing screening; PLADs=provincial-level administrative divisions.
By 2020, China had achieved a 94.3% initial hearing screening completion rate among newborns. Of those who failed the initial screening, 87.2% completed the repeat screening protocol. Among infants who failed the repeat screening, 62.0% received comprehensive audiological diagnosis, resulting in a congenital hearing loss detection rate of 1.6 per 1,000 newborns (
Supplementary Table S2 ).Special schools for deaf-mutes and hearing-impaired students in special schools: Students with hearing impairments may attend one of three educational settings: regular schools, comprehensive special schools that serve multiple types of disabilities, or specialized schools exclusively for deaf-mutes. In 2001, before the widespread implementation of UNHS, specialized schools for deaf students comprised 41.7% (639/1,531) of all special schools in China. This proportion decreased to 31.7% (541/1,706) by 2010, and further declined to 17.3% (389/2,244) in 2020, six years after achieving national UNHS coverage (
Supplementary Figure S3 ).Concurrent with this institutional shift, enrollment of hearing-impaired students in special schools has shown a marked decline over the past two decades. From 2001 to 2020, the number of hearing-impaired students in special schools decreased by 54.4%, from 76,554 to 34,945 (
Supplementary Figure S3 ).Mainstream education proportion among hearing-impaired students: In China, hearing-impaired students who achieve satisfactory rehabilitation outcomes typically integrate into mainstream schools. The mainstream education proportion was calculated as the ratio of hearing-impaired students in mainstream schools to the total number of hearing-impaired students in both mainstream and special schools. Students enrolled in attached special education classes within mainstream schools, though relatively few, were excluded from this calculation. The overall mainstream education proportion for hearing-impaired students from grades one through nine increased substantially from 24.8% in 2001 to 57.5% in 2020 (Table 1). When analyzed by educational stage within China’s nine-year compulsory education system, which comprises elementary school (grades one through six) and middle school (grades seven through nine), the mainstream education proportion showed differential growth. From 2001 to 2020, elementary school integration increased from 26.8% to 62.2%, while middle school integration rose from 16.5% to 48.2%.
Year Compulsory Education Stage
(grade 1st–9th)Elementary School Stage
(grade 1st–6th)Middle School Stage
(grade 7th–9th)N Proportion (%) N Porportion (%) N Proportion (%) 2001 25,520 24.8 22,327 26.8 3,193 16.5 2002 27,408 25.2 22,308 26.4 5,100 21.1 2003 26,558 24.2 21,353 25.8 5,205 19.3 2004 27,060 24.0 21,122 25.2 5,938 20.4 2005 27,781 24.1 21,733 25.8 6,048 19.6 2006 26,444 22.8 20,620 24.5 5,824 18.4 2007 28,268 24.9 21,111 25.3 7,157 23.7 2008 26,727 23.9 19,427 24.1 7,300 23.5 2009 25,412 23.3 17,865 23.0 7,547 23.9 2010 23,980 22.6 17,189 22.9 6,791 22.1 2011 21,389 21.2 14,866 21.1 6,523 21.6 2012 19,244 20.5 13,674 20.7 5,570 19.9 2013 17,189 20.8 12,334 21.2 4,855 19.7 2014 20,095 24.4 14,469 25.1 5,626 22.8 2015 24,432 29.3 17,784 30.4 6,648 26.6 2016 28,425 33.8 20,846 35.4 7,579 29.9 2017 34,000 40.3 24,959 43.0 9,041 34.3 2018 35,348 44.0 25,576 47.7 9,772 36.6 2019 42,900 51.9 30,907 56.7 11,993 42.6 2020 47,251 57.5 33,853 62.2 13,398 48.2 Note: Source from public data released by the Ministry of Education of China, at http://www.moe.gov.cn/jyb_sjzl/moe_560/. Table 1. Number and proportion of hearing-impaired students in mainstream education in China, 2001–2020.
-
This nationwide study demonstrates that China’s UNHS program coverage increased substantially from 10.9% to 94.3%, while concurrent mainstream school enrollment for hearing-impaired students rose markedly from 24.8% to 57.5% over the past two decades.
The UNHS program, as a proactive public health initiative, has profoundly impacted early diagnosis, etiological identification, and timely intervention for pediatric hearing loss. China’s remarkable progress in screening coverage from 10.9% in 2005 to 94.3% in 2020 was facilitated by technical advancements, enhanced training implementation, and particularly the development of the maternal and child health system. The dramatic increase in hospital delivery rates from 76.0% in 2001 to 99.2% in 2012 enabled the integration of newborn screening as standard hospital protocol (9). However, significant regional disparities persist, with some PLADs reporting screening rates substantially below the national average. The Gini coefficient for diagnosis and treatment centers (0.36) exceeds those of other resources (0.21, 0.29, and 0.26 for screening institutions, rehabilitation facilities, and special schools, respectively), likely reflecting the higher staffing and equipment requirements for diagnostic facilities. These disparities highlight potential areas for UNHS system improvement. Despite the establishment of a preliminary UNHS management framework, many specialists advocate for developing a nationally integrated informatics platform to enhance screening, diagnosis, and intervention rates while addressing regional inequities.
Historically, hearing-impaired children were predominantly enrolled in specialized schools for the deaf and hard of hearing (10). Contemporary approaches now emphasize mainstream education integration, supported by early diagnosis and comprehensive hearing interventions. For instance, in the Netherlands, 61% of hearing-impaired children attend mainstream elementary education (11). Modern mainstream schools increasingly provide inclusive educational environments through various formats, including regular classes, resource rooms, and separate classes. In mainland China, the proportion of hearing-impaired students in regular mainstream classes has risen substantially from 24.8% in 2001 to 57.5% in 2020. Within mainstream schools, hearing-impaired students are primarily integrated through two approaches: attached special classes (dedicated classes for hearing-impaired students) and full integration into regular classes, with the latter being the predominant model. Future research should focus on tracking the academic performance of hearing-impaired students, given the long-term developmental impact of hearing loss. Additionally, an integrated service system encompassing both medical treatment and education is anticipated.
The reduction in special schools for deaf-mutes from 679 in 2001 to 389 in 2020 can be attributed to several key factors. First, the expanded UNHS coverage and enhanced early intervention protocols have played a crucial role. Second, systematic educational reforms have significantly influenced this transition. Third, the comprehensive service system for hearing-impaired children has evolved to integrate screening, diagnosis, intervention, rehabilitation, and education through coordinated efforts among the Health Commission, the Disabled Persons’ Federations, and the Ministry of Education. This multi-departmental collaboration has effectively reduced both the number of specialized schools and their enrollment rates. However, the shift toward mainstream education cannot be solely attributed to increased UNHS coverage, as multiple factors influence this trend, including health and educational policies, financial support mechanisms, and broader socioeconomic considerations. For example, more than 10 PLADs (including Shanghai, Jiangsu, Zhejiang, etc.) have progressively included cochlear implants in their basic medical insurance coverage. Furthermore, the first centralized procurement program will significantly reduce cochlear implant costs from over 200,000 CNY (27,400 USD) to approximately 50,000 CNY after March 2025, substantially improving intervention accessibility for hearing-impaired newborns. Additionally, as part of the educational reform, many special schools for deaf-mutes are transitioning into rehabilitation schools for preschool children with hearing aids and/or cochlear implants, focusing on preparing them for future mainstream society integration. Consequently, many teachers of the deaf are undergoing specialized training to become speech and language therapists (SLTs).
Over the past two decades, China has achieved remarkable progress in expanding newborn hearing screening coverage and increasing mainstream school enrollment among hearing-impaired students. To address persistent challenges, including regional disparities in screening and diagnostic rates, the establishment of a comprehensive national informatic platform for the UNHS system remains essential.
HTML
History and Policy of UNHS in China
Resource Equity
Health Impacts
Challenges and Prospects
-
All participants from the National Health Commission of China, China Disabled Persons’ Federations, and Ministry of Education of the People’s Republic of China. All colleagues who have contributed to the UNHS project in China over the past twenty years. Sijia Xu for providing schema and Colin Woodham for language editing.
| Citation: |

|