
 Download:
Download:




-
Introduction: The clinical durations of sporadic Creutzfeldt-Jacob disease (sCJD) patients typically do not exceed 2 years, though considerable variation exists. The factors influencing survival among Chinese sCJD patients remain incompletely characterized.
Methods: We analyzed the potential elements associated with survival using the data of 300 probable sCJD cases from 2020 to 2022 by China National Surveillance for CJD. The associations of 31 factors in 7 categories with survival were estimated by univariate analysis of Kaplan-Meier and multivariate regression analysis of Cox proportional hazard model.
Results: Statistical assays figured out that the patients >65 year-old at onset, having pyramidal or extrapyramidal dysfunction, recording high signal in caudate/putamen on magnetic resonance imaging (MRI), and not receiving nasal feeding were closely associated with short survival. In the subgroup analysis of ≤65 years and >65 years at onsetage, nasal feeding was the contributor to prolonged survival for both groups. MRI high signal of caudate/putamen in the younger group and pyramidal or extrapyramidal dysfunction in older group seemed to be more associated with poor survival separately.
Conclusions: The data indicate the onsetage and nasal feeding are the most crucial factors influencing the prognosis for Chinese sCJD patients, establishing an evidence base for developing and implementing targeted intervention strategies.
-
Human prion diseases encompass Creutzfeldt-Jacob disease (CJD), Kuru, Gerstmann-Sträussler-Scheinker syndrome (GSS), and fatal familial insomnia (FFI). Globally, sporadic CJD (sCJD) accounts for approximately 85% of human prion diseases, while 10%–15% are genetic forms associated with mutations in the PRNP gene — including genetic CJD (gCJD), GSS, and FFI. The remaining 1% are acquired forms, such as Kuru, iatrogenic CJD (iCJD), and variant CJD (vCJD) (1). While sCJD predominantly affects individuals aged 60–70 years, onset can occur between 20–90 years. Clinical presentations vary substantially among sCJD patients, with disease durations ranging from several months to 2 years (2). Despite numerous clinical trials over recent decades (3-4), effective prophylactic and therapeutic interventions remain elusive. Therefore, prompt and appropriate symptomatic management, along with proper nursing care, are crucial for improving patient outcomes.
Previous evaluations of Chinese sCJD patients revealed a median clinical duration of approximately 5.3 months (5). However, factors influencing survival time remain incompletely understood. In this retrospective cohort study, we analyzed 300 probable sCJD cases diagnosed through the China National Surveillance for CJD (CNS-CJD) from January 1, 2020, to December 31, 2022. Diagnoses were established according to the Chinese National Health Commission’s CJD diagnostic criteria as previously described. The study incorporated comprehensive medical records, epidemiological information, clinical data, laboratory findings, and follow-up documentation. We examined the relationship between survival time and 31 factors across 7 categories, including demographic characteristics, clinical features, laboratory results, and post-diagnosis medical care. To ensure data integrity, cases were selected based on criteria outlined in Figure 1, with standardized questionnaires administered by trained investigators to minimize information bias. Follow-up concluded on December 31, 2023, with surviving cases classified as censored. Survival time was calculated from disease onset to death.
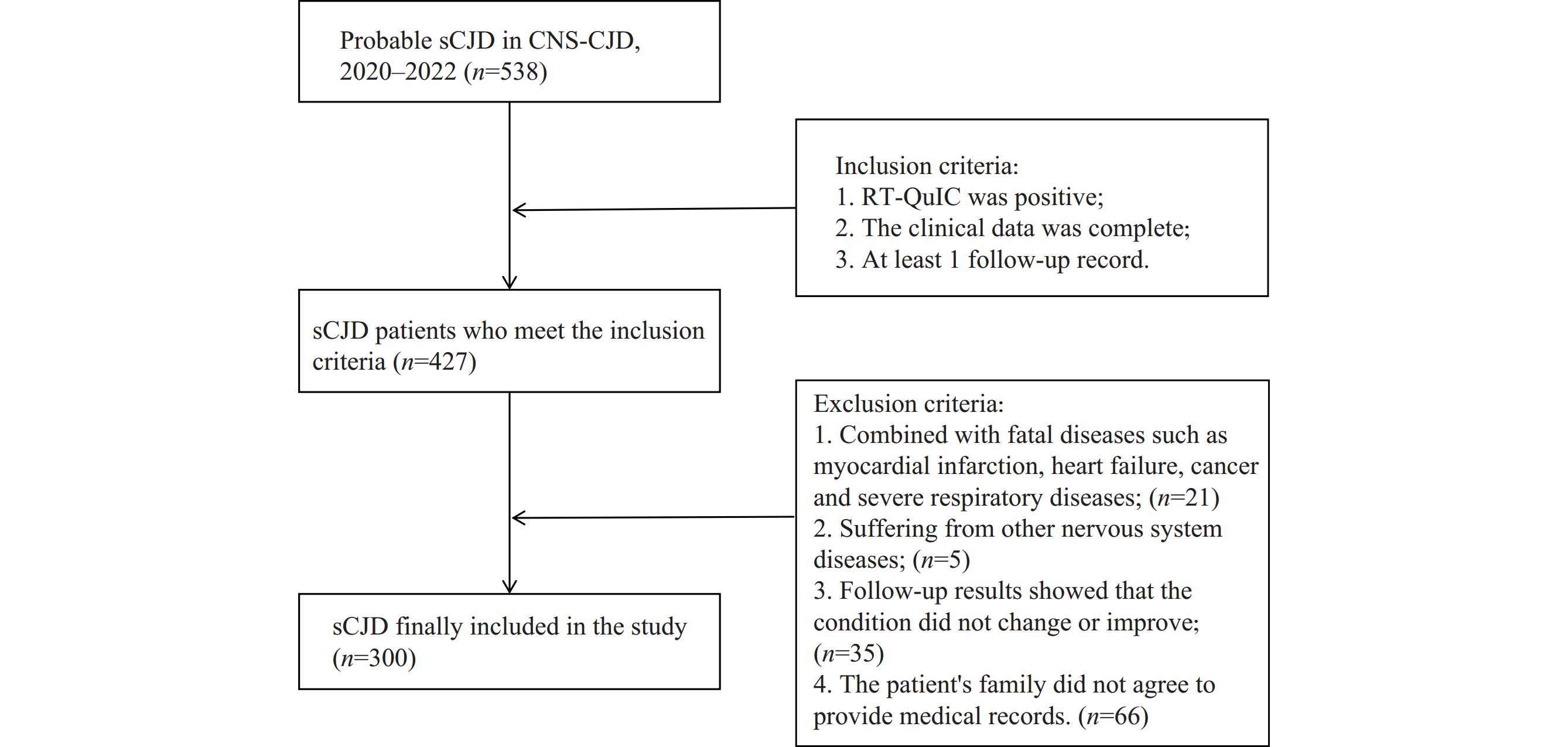 Figure 1.
Figure 1.Flow chart of case selection.
Abbreviation: sCJD=sporadic Creutzfeldt-Jacob disease; CNS-CJD=China National Surveillance for CJD; RT-QuIC=Real-time Quaking-Induced Conversion.Statistical analysis was performed using SPSS 21.0 statistical software (IBM, Armonk, NY, USA). Survival times with 95% confidence intervals (CI) were calculated using the Kaplan-Meier estimator. Between-group differences in survival time were assessed using the log-rank test. Factors showing statistical significance (P<0.05) in univariate analysis were subsequently evaluated through multivariate analysis using the Cox proportional hazard model to determine hazard ratios (HR) with corresponding 95% CI. The complete workflow for data collection and statistical evaluation is detailed in
Supplementary Figure S1 .Of the 300 sCJD cases documented in CNS-CJD, 285 cases had confirmed death dates prior to the follow-up endpoint, while 15 cases were censored. The median survival time was 5 months (95% CI: 4.165, 5.835). The cohort demonstrated a male-to-female ratio of 1:1.14, with an average onset age of 65 years (range: 39–84 years). The majority of cases (187 cases, 62.3%) occurred in patients aged 60–74 years.
Analysis of 31 factors across 7 categories using Kaplan-Meier methodology revealed several significant associations with survival time (Table 1). Among demographic factors, onset age showed statistical significance (P=0.035), with patients >65 years demonstrating shorter survival times (median: 5 months, 95% CI: 3.644, 6.356) (
Supplementary Figure S2A ). Regarding clinical manifestations, patients without pyramidal or extrapyramidal dysfunction exhibited significantly longer survival times (median: 7 months, 95% CI: 2.962, 11.038, P=0.003) (Supplementary Figure S2B ). Clinical examinations revealed that cases with high signal intensity in caudate/putamen on magnetic resonance imaging (MRI) had shorter survival times (median: 4 months, 95% CI: 3.972, 6.028, P=0.004) (Supplementary Figure S2C ). In the category of medical support and therapeutics, nasal feeding demonstrated significant impact on survival (P<0.001), with patients receiving nasal feeding showing longer duration (median: 8 months, 95% CI: 6.137, 9.863) (Supplementary Figure S2D ). Further analysis of survival based on the frequency of four sCJD-associated symptoms (visual or cerebellar disturbance, myoclonus, pyramidal and extrapyramidal symptoms, mutism) or three MRI abnormalities (symmetrical or asymmetrical cortical “ribbon” signs on diffusion weighted imaging (DWI), high signal in caudate/putamen, or high signal in bilateral posterior thalamic tuberosity in the proton density phase) showed no statistical significance, although patients with more symptoms or MRI abnormalities tended toward shorter survival durations (Supplementary Table S1 ).Factor Cases (%) Median (m) (95% CI) χ2 P Demographics Onsetage (years) 4.441 0.035* 35–65 166 (55.3) 6 (4.356, 7.644) ≥66 134 (44.7) 5 (3.644, 6.356) Gender 0.127 0.721 Male 140 (46.7) 5 (3.762, 6.238) Female 160 (53.3) 6 (4.229, 7.771) Geographic area 4.543 0.604 Northeastern 21 (7.0) 6 (1.514, 10.486) Eastern 86 (28.7) 6 (4.403, 7.597) Northern 43 (14.3) 4 (2.847, 5.153) Central 56 (18.7) 7 (4.340, 9.660) Southern 10 (3.3) 3 (1.482, 4.518) Southwestern 66 (22.0) 5 (3.508, 6.492) Northwestern 18 (6.0) 5 (0, 11.237) Residence 0.821 0.365 Urban 121 (40.3) 5 (4.600, 7.400) Rural 179 (59.7) 6 (3.690, 6.310) Initial symptom Rapid dementia 0.001 0.971 Yes 236 (78.7) 5 (3.950, 6.050) No 64 (21.3) 6 (3.060, 8.940) Slow dementia 1.833 0.176 Yes 17 (5.7) 10 (3.277, 16.723) No 283 (94.3) 5 (4.162, 5.838) Mental problems 0.210 0.647 Yes 109 (36.3) 6 (4.198, 7.802) No 191 (63.7) 5 (4.010, 5.990) Cortical blindness 1.297 0.255 Yes 31 (10.3) 4 (2.205, 5.795) No 269 (89.7) 6 (4.934, 7.066) Cerebellar disturbance 2.821 0.093 Yes 105 (35.0) 4 (3.163, 4.837) No 195 (65.0) 6 (4.632, 7.368) Pyramidal or extrapyramidal dysfunction 3.318 0.069 Yes 100 (33.3) 5 (3.726, 6.274) No 200 (66.7) 6 (4.570, 7.430) Clinical manifestation Myoclonus 1.073 0.300 Yes 200 (66.7) 5 (4.012, 5.988) No 100 (33.3) 6 (4.272, 7.728) Visual or cerebellar disturbance 2.162 0.141 Yes 222 (74.0) 5 (4.071, 5.929) No 78 (26.0) 7 (5.569, 8.431) Pyramidal or extrapyramidal dysfunction 9.043 0.003** Yes 248 (82.7) 5 (4.095, 5.905) No 52 (17.3) 7 (2.962, 11.038) Akinetic mutism 2.316 0.128 Yes 238 (79.3) 6 (4.839, 7.161) No 62 (20.7) 4 (2.980, 5.020) Clinical examination EEG (PSWC) <0.001 0.985 Yes 82 (27.3) 5 (2.953, 7.047) No 218 (72.7) 5 (3.842, 6.158) MRI High signal in caudate/putamen 8.084 0.004** Yes 101 (33.7) 5 (3.972, 6.028) No 199 (66.3) 6 (4.467, 7.533) ‘‘Ribbon’’ signs 0.233 0.629 Yes 233 (77.7) 5 (4.103, 5.897) No 67 (22.3) 7 (4.824, 9.176) High signal in posterior tuberosity of thalamus 0.007 0.935 Yes 29 (9.7) 6 (4.688, 7.312) No 271 (90.3) 5 (4.121, 5.879) Laboratory test CSF 14-3-3 1.903 0.168 pos 213 (71.0) 5 (4.022, 5.998) neg 87 (29.0) 6 (4.481, 7.519) PRNP seq Codon 129 0.611 0.737 MM 295 (98.3) 5 (4.172, 5.828) MV 4 (1.3) 2 VV 1 (0.3) 9 Codon 219 − − EE 300 (100) 5 (4.165, 5.835) EK 0 (0.0) − Nursing and care Place 3.739 0.154 Professional unit 150 (50.0) 6 (4.588, 7.412) At home 106 (35.3) 4 (2.739, 5.261) Both 44 (14.7) 4 (2.561, 5.439) Personnel 1.362 0.506 Registered nurse 63 (21.0) 6 (2.667, 9.333) Care worker 182 (60.7) 5 (4.009, 5.991) Both 55 (18.3) 6 (3.587, 8.413) Symptomatic care 0.741 0.389 Yes 280 (93.3) 6 (4.913, 7.087) No 20 (6.7) 4 (0.000, 8.361) Medical supporting and therapeutics Nasal feeding 20.795 <0.001*** Yes 146 (48.7) 8 (6.137, 9.863) No 154 (51.3) 4 (3.330, 4.670) Nutrition injection i.v. 1.620 0.203 Yes 114 (38.0) 5 (3.573, 6.427) No 186 (62.0) 5 (3.972, 6.028) Nutrition oral 0.044 0.833 Yes 29 (9.7) 7 (4.890, 9.110) No 271 (90.3) 5 (4.136, 5.864) Respiratory support 0.105 0.746 Yes 95 (31.7) 5 (3.322, 6.678) No 205 (68.3) 6 (4.885, 7.115) Symptomatic treatment 1.952 0.162 Yes 88 (29.3) 6 (4.471, 7.529) No 212 (70.7) 5 (3.876, 6.124) Antibiotic therapy 0.896 0.344 Yes 35 (11.7) 7 (3.688, 10.312) No 265 (88.3) 5 (4.097, 5.903) Antiviral therapy 0.243 0.622 Yes 53 (17.7) 5 (3.714, 6.286) No 247 (82.3) 6 (4.941, 7.059) Abbreviation: sCJD=sporadic Creutzfeldt-Jakob disease; m=months; CI=confidence intervals; PSWC=periodic sharp wave complexes; EEG=electroencephalogram; MRI=magnetic resonance imaging; CSF=cerebrospinal fluid; seq=sequence; i.v.=intravenous.
* P<0.05;
** P<0.01;
*** P<0.001.Table 1. Univariate analysis of factors associated with survival in sCJD patients.
The factors demonstrating statistical significance in the univariate analysis were further evaluated using multivariate regression with Cox proportional hazard modeling. As shown in Table 2, all four factors maintained statistical significance. Analysis of HR values revealed significantly elevated hazard risks in patients who were >65 years at onset (HR: 1.379, 95% CI: 1.088, 1.748), presented with pyramidal or extrapyramidal dysfunction (HR: 1.476, 95% CI: 1.060, 2.054), demonstrated high signal intensity in caudate/putamen on MRI (HR: 1.346, 95% CI: 1.045, 1.733), or did not receive nasal feeding (HR: 1.711, 95% CI: 1.349, 2.169).
Factor β SE Wald χ2 P HR (95% CI) Onset age (years) 35–65 1.000 ≥66 0.321 0.121 7.039 0.008** 1.379 (1.088, 1.748) Pyramidal or extrapyramidal dysfunction No 1.000 Yes 0.389 0.169 5.319 0.021* 1.476 (1.060, 2.054) High signal in caudate/putamen No 1.000 Yes 0.297 0.129 5.278 0.022* 1.346 (1.045, 1.733) Nasal feeding Yes 1.000 No 0.537 0.121 19.642 <0.001*** 1.711 (1.349, 2.169) Abbreviation: sCJD=sporadic Creutzfeldt-Jacob disease; HR=hazard ratio; CI=confidence intervals.
* P<0.05;
** P<0.01;
*** P<0.001.Table 2. Multivariate regression analysis of the factors associated with survival in sCJD.
Further stratified analyses were conducted by dividing cases into age groups (≤65 years and >65 years) for both univariate and multivariate regression analyses (Table 3). In the ≤65 years group, univariate analysis identified five significant factors associated with survival time: cortical blindness as an initial symptom (P=0.037), cerebellar disturbance (P=0.032), pyramidal or extrapyramidal dysfunction (P=0.028), high signal in caudate/putamen on MRI (P=0.004), and nasal feeding (P=0.019). Subsequent multivariate Cox regression analysis revealed two significant factors: high signal in caudate/putamen (HR: 1.556, 95% CI: 1.111, 2.178, P=0.010) and absence of nasal feeding (HR: 1.476, 95% CI: 1.072, 2.033, P=0.017) In the group of >65 years group, four factors showed statistical significances in the univariate assay, including care place (P=0.022), akinetic mutism (P=0.016), pyramidal or extrapyramidal dysfunction (P=0.027), nasal feeding (P=0.019). Multivariate Cox regression analysis indicated 1.695-fold increased death risk (95% CI: 1.056, 2.721, P=0.025) in the patients with pyramidal or extrapyramidal dysfunction, and 2.386-fold increased death risk (95% CI: 1.605, 3.548, P<0.001).
Factor Univariate analysis Multivariate analysis Cases (%) Median of survival (m) (95% CI) P χ2 P HR (95% CI) sCJD cases ≤65 years (n=166) Cortical blindness in initial symptoms 0.037* 2.301 0.129 Yes 8 (4.8) 4 (1.288, 6.772) 1.000 No 158 (95.2) 6 (4.241, 7.759) 0.568 (0.274, 1.180) Cerebellar disturbance in initial symptoms 0.032* 2.919 0.088 Yes 56 (33.7) 4 (3.025, 4.975) 1.000 No 110 (66.3) 7 (4.944, 9.056) 0.746 (0.533, 1.044) Pyramidal or extrapyramidal dysfunction 0.028* 1.871 0.171 Yes 139 (83.7) 5 (3.641, 6.359) 1.000 No 27 (16.3) 10 (6.183, 13.817) 0.723 (0.454, 1.151) High signal in caudate/putamen 0.004** 6.628 0.010* No 66 (39.8) 7 (4.550, 9.450) 1.000 Yes 100 (60.2) 5 (3.513, 6.487) 1.556 (1.111, 2.178) Nasal feeding 0.019* 5.686 0.017* Yes 84 (50.6) 8 (4.777, 11.223) 1.000 No 82 (49.4) 4 (2.622, 5.378) 1.476 (1.072, 2.033) sCJD cases >65 years (n=134) Place of care 0.022* 2.713 0.258 Professional unit 70 (52.2) 6 (4.366, 7.634) 1.000 At home 54 (40.3) 4 (3.105, 4.895) 1.359 (0.942, 1.961) Both 10 (7.5) 3 (2.290, 3.710) 1.163 (0.771, 1.755) Akinetic mutism 0.016* 0.207 0.649 Yes 107 (79.9) 5 (3.311, 6.689) 1.000 No 27 (20.1) 3 (1.728, 4.272) 1.114 (0.610, 1.372) Pyramidal or extrapyramidal dysfunction 0.027* 5.031 0.025* Yes 109 (81.3) 6 (3.062, 8.938) 1.000 No 25 (18.7) 4 (2.636, 5.364) 1.695 (1.056, 2.721) Nasal feeding 0.019* 18.464 <0.001*** Yes 64 (47.8.) 7 (5.041, 8.959) 1.000 No 70 (52.2) 4 (3.154, 4.845) 2.386(1.605, 3.548) Abbreviaiton: sCJD=sporadic Creutzfeldt-Jakob disease; m=months; HR=hazard ratio; CI=confidence intervals.
* P<0.05;
** P<0.01;
*** P<0.001.Table 3. Univariate and multivariate regression analysis of factors associated with survival in two groups ≤65 and >65 years.
-
Human prion diseases, including sCJD, remain universally fatal with significantly shorter clinical durations compared to other neurodegenerative disorders such as Alzheimer disease (AD) and Parkinson disease (PD) (1). Through analysis of 300 probable sCJD cases reported to the China National Surveillance for CJD between January 2020 and December 2022, we identified four key factors associated with shortened survival times: age greater than 65 years at onset, presence of pyramidal or extrapyramidal dysfunction, high signal intensity in caudate/putamen on MRI, and absence of nasal feeding.
Our findings demonstrate that patient age at disease onset significantly influences survival duration in Chinese sCJD patients. Elderly patients exhibited a 1.379-fold increased mortality risk compared to younger patients, consistent with previous studies documenting age-dependent decreased survival in sCJD (6-7). This association may be attributed to compromised health status and increased comorbidities in older populations, although some studies have failed to establish a clear correlation between onset age and clinical duration (8-9). Pyramidal or extrapyramidal dysfunction emerged as a negative prognostic factor, particularly in patients over 65 years at onset. These movement disorders, which encompass tremors, postural and gait abnormalities, limb ataxia, and dystonic spasms, are common in sCJD patients and may increase the risk of falls while complicating daily care management.
The prognostic significance of MRI for sCJD remains incompletely understood. A recent Korean study demonstrated that caudate nucleus and putamen involvement on diffusion-weighted imaging (DWI) correlates with poor prognosis (7). Our findings align with this observation, revealing high signal intensity in the caudate nucleus and putamen as a negative prognostic factor for sCJD survival, particularly in patients ≤65 years at onset. MRI lesion patterns in sCJD cases appear to demonstrate age-dependent characteristics. Previous research indicates that typical cortical and basal ganglia hyperintensities predominate in younger patients, while unilateral hemispheric or isolated cortical lesions occur more frequently in older individuals (10). Furthermore, extensive DWI abnormalities, particularly those involving three or more lobes with moderate to extensive cortical and striatal involvement, correlate with notably shortened median survival of approximately 1.7 months (7). Importantly, most sCJD patients in our cohort underwent single evaluations of MRI, electroencephalogram (EEG), and CSF 14-3-3 testing post-onset. Serial examinations, combined with clinical features, would enable more precise stratification and prognostication of sCJD cases.
Nasal feeding demonstrates significant survival benefits for sCJD patients. Japanese research has similarly shown that tube-fed patients experience significantly extended survival compared to non-tube-fed patients, regardless of whether feeding was administered via nasogastric tube or gastrostomy (7). Additionally, enteral nutrition through percutaneous endoscopic gastrostomy or radiologically inserted gastrostomy correlates with markedly improved survival across sCJD, gCJD, and acquired CJD patients (11). We posit that nasal feeding represents a crucial intervention in the advanced-stage care of CJD patients. While dysphagia frequently compromises nutritional intake in CJD patients, nasal feeding offers a less invasive alternative to gastrostomy that can be readily implemented in small clinical settings or home environments.
Several limitations should be acknowledged in this study. First, all cases were classified as probable sCJD without neuropathological confirmation or PrPSc detection, which may introduce diagnostic bias. Second, the relatively modest sample size necessitates further validation through expanded cohort studies to confirm the stability of our findings. Third, the implementation of nasogastric feeding is influenced by multiple factors, including family support, patient end-of-life preferences, and physician judgment, which may confound the observed associations. Continued evaluation of these identified survival factors through ongoing CJD surveillance will be crucial for optimizing medical interventions and care strategies for Chinese CJD patients.
-
Received approval from the Ethical Committee of the National Institute for Viral Disease Control and Prevention, China CDC (protocol 2009ZX10004-101).
HTML
| Citation: |

|