
 Download:
Download:




-
The human respiratory syncytial virus (HRSV) belongs to the Orthopenumovirus genus within the Pneumoviridae family (1) and represents the primary etiological agent of acute lower respiratory tract infections (ALRTIs) in children under 5 years, immunocompromised individuals, and elderly populations (2-3). Globally in 2019, HRSV was responsible for 33 million ALRTI episodes, resulting in 3.6 million hospitalizations and 101,400 deaths among children younger than 5 years (1). China bears a substantial burden of HRSV infections, accounting for more than 10% of global cases (4).
Advanced diagnostic technologies in hospital settings have revealed an increasing frequency of HRSV codetection with other respiratory viruses (5). Contemporary research indicates that HRSV codetection with other respiratory viruses occurs in 35%–40% of HRSV infections among young children (6-7). However, the impact of viral and bacterial coinfections on the disease burden of HRSV-associated respiratory illnesses remains incompletely understood (8).
This study examined hospitalized children aged ≤5 years admitted with influenza-like illness (ILI), acute respiratory infection (ARI), or severe acute respiratory infection (SARI) (
Supplementary File 1 ) between January 1, 2018, and August 31, 2023, across eight hospitals in Zhejiang Province. HRSV infection was confirmed through laboratory antigen testing or reverse transcription polymerase chain reaction (RT-PCR). Hospital selection criteria incorporated geographical location, economic development level, and population coverage considerations (Supplementary File 2 Supplementary Table S1 ). Total hospitalization costs encompassed all direct patient expenses during admission, including examination, medication, bed, and treatment fees. To account for temporal cost variations across the 5-year study period, this research applied a 3% discount rate (9) to adjust hospitalization costs from 2018–2022.This study stratified patients into four categories based on pathogen infection status: HRSV alone, HRSV+virus, HRSV+bacteria, and HRSV+virus+bacteria. Pathogen positivity rates were compared across these groups, considering gender, age group, pneumonia status, coronavirus disease 2019 (COVID-19) epidemic phases, and hospitalization duration. This study analyzed the pathogen spectrum in HRSV coinfection cases and evaluated the hospitalization duration and total costs associated with the three most prevalent viral and bacterial coinfections.
Statistical analyses were conducted using R software version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was established at P<0.05 (two-tailed).
Between January 2018 and August 2023, the eight participating hospitals recorded 8,338,484 outpatient and 252,658 inpatient visits across all age groups. Of these, 180,601 patients underwent HRSV testing via nucleic acid or antigen detection methods, yielding 10,956 positive cases (positivity rate: 6.07%). The highest monthly positivity rates were observed in August 2021 (26.9%) and December 2018 (25.9%), while no positive cases were detected in May and June 2020 (Figure 1A).
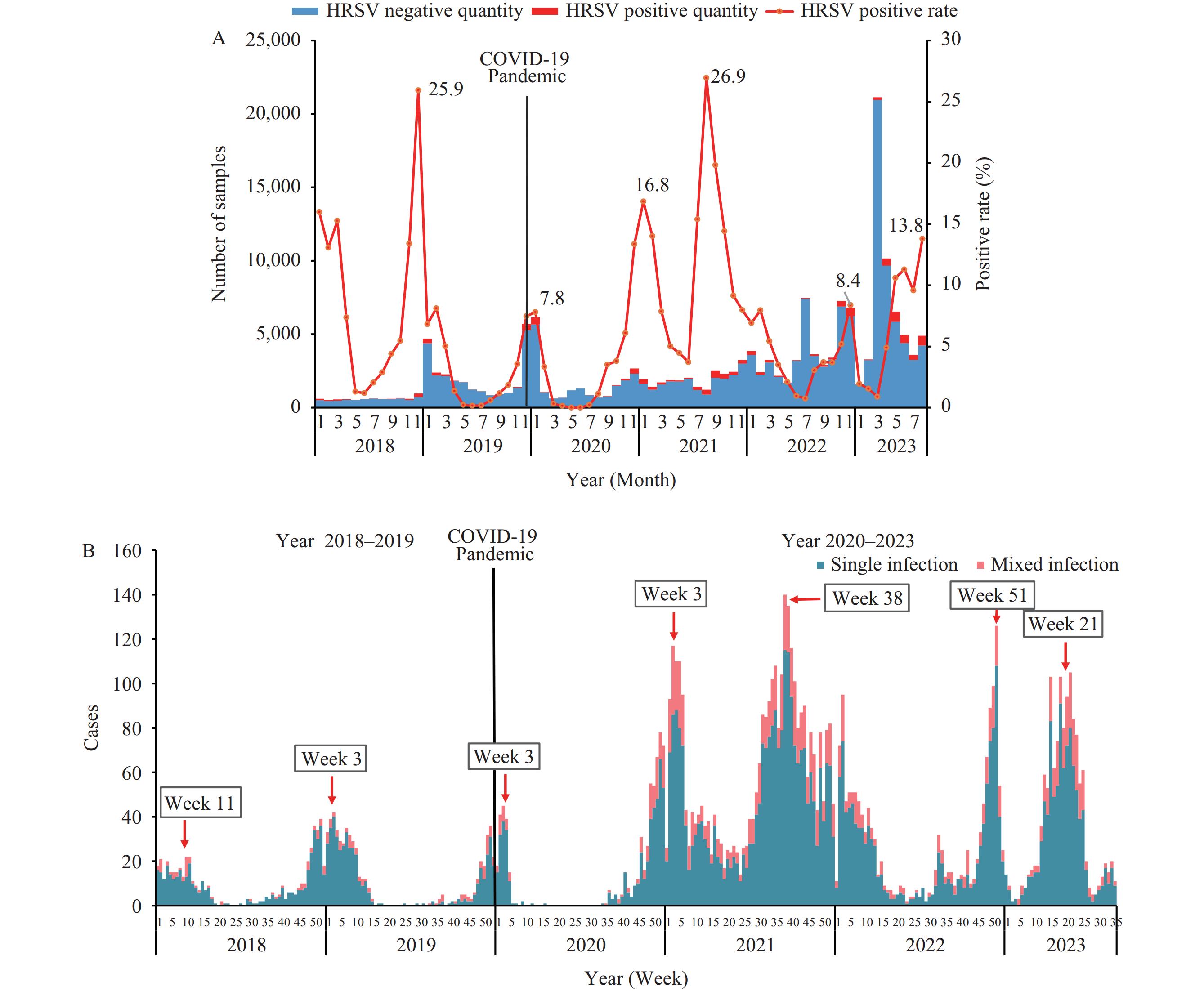 Figure 1.
Figure 1.The timeline distribution of HRSV monoinfections and coinfections among outpatients and inpatients in Zhejiang Province, China, 2018–2023. (A) Monthly detection rates of HRSV among outpatients and inpatients; (B) Weekly distribution of HRSV monoinfections and coinfections among hospitalized children aged 5 years and younger.
Abbreviation: COVID-19=coronavirus disease 2019; HRSV=human respiratory syncytial virus.Among the 7,857 HRSV-positive inpatients aged 5 years and younger included in this study, the median age was 12.0 months [interquartile range (IQR): 4.0–24.0 months], with 65.9% being 12.0 months or younger. Males comprised 60.4% (4,746/7,857) of the cohort, and 80.9% (6,360/7,857) were diagnosed with pneumonia. HRSV coinfection with other pathogens was identified in 20.4% (1,601/7,857) of cases.
A significant increase in HRSV hospitalizations was observed from 2020 to 2023 compared to 2018–2019 (Figure 1A). The median age of patients during the COVID-19 pandemic period (2020–2023) was significantly higher than in the pre-pandemic period (2018–2019) (17.0 months vs. 10.1 months, P<0.010). The pandemic period saw a reduction in the proportion of HRSV inpatients aged 0–5 months (from 45% to 28%) and concurrent increases in those aged 13–24 months (from 9% to 15%) and 25–36 months (from 6% to 15%) (
Supplementary Figure S1 ).Compared to HRSV mono-infection cases, patients with coinfections were significantly older (19.7 months vs. 15.0 months, P<0.01) (Table 1). Notable increases were observed in the 13-24 months (13% to 18%) and 25-36 months (12% to 20%) age groups (
Supplementary Figure S2 ). Coinfection rates were lower in males compared to females (18.8% vs. 22.7%, P<0.01) and higher in pneumonia cases compared to non-pneumonia cases (21.9% vs. 14.1%, P<0.01), Table 1. The highest coinfection rates were observed in patients with hospital stays of 15 days (31.2%), followed by those staying 8–14 days (21.7%) (Table 1).Categories Number
(N=7,857)Mono-HRSV
infection
(n1=6,256)Co-HRSV infection P Total
(n2=1,601)HRSV+virus (n3=418) HRSV+ba-cteria (n4=1,110) HRSV+virus+
bactetia
(n5=73)Proportion, No. (%) 7,857 (100.0) 6,256 (79.6) 1,601 (20.4) 418 (26.1) 1,110 (69.3) 73 (4.6) − Gender, No. (%) Male 4,746 (60.4) 3,852 (81.2) 894 (18.8) 256 (28.6) 599 (67.0) 39 (4.4) <0.0001 Female 3,111 (39.6) 2,404 (77.3) 707 (22.7) 162 (22.9) 511 (72.3) 34 (4.8) Mean age (months) 15.9 15.0 19.7 16.4 20.9 20.9 Age group (months), No. (%) 0–5 2,383 (30.3) 2,085 (87.5) 298 (12.5) 135 (45.3) 150 (50.3) 13 (4.4) 0.035 6–12 2,816 (35.8) 2,225 (79.0) 591 (21.0) 147 (24.9) 421 (71.2) 23 (3.9) 0.663 13–24 1,124 (14.3) 841 (74.8) 283 (25.2) 60 (21.2) 207 (73.1) 16 (5.7) 0.004 25–36 1,039 (13.2) 735 (70.7) 304 (29.3) 56 (18.4) 234 (77.0) 14 (4.6) 0 37–48 376 (4.8) 274 (72.9) 102 (27.1) 14 (13.7) 82 (80.4) 6 (5.9) 0.007 49–60 119 (1.6) 96 (80.7) 23 (19.3) 6 (26.1) 16 (69.6) 1 (4.3) Reference group Pneumonia or not, No. (%) Yes 6,360 (81.0) 4,970 (78.1) 1,390 (21.9) 315 (22.7) 1,017 (73.2) 58 (4.1) 0 No 1,497 (19.0) 1,286 (85.9) 211 (14.1) 103 (48.8) 93 (44.1) 15 (7.1) Period, No. (%) Year 2018–2019 1,081 (13.8) 925 (85.6) 156 (14.4) 53 (34.0) 99 (63.5) 4 (2.5) 0 Year 2020–2023 6,776 (86.2) 5,331 (78.7) 1,445 (21.3) 365 (25.3) 1,011 (70.0) 69 (4.7) Hospitalization duration (day) 1–3 950 (12.1) 827 (87.1) 123 (12.9) 43 (35.0) 78 (63.4) 2 (1.6) 0 4–7 5,847 (74.4) 4,605 (78.7) 1,242 (21.2) 290 (23.3) 898 (72.3) 54 (4.4) 0.052 8–14 996 (12.7) 780 (78.3) 216 (21.7) 73 (33.8) 129 (59.7) 14 (6.5) 0.075 >15 64 (0.8) 44 (68.8) 20 (31.2) 12 (60.0) 5 (25.0) 3 (15.0) Reference group Note: P comparing mono-HRSV infection vs. co-HRSV infection.
Abbreviation: HRSV=human respiratory syncytial virus.Table 1. Pathogen positivity rates among hospitalized children aged ≤5 years with human respiratory syncytial virus infections in multicenter surveillance, Zhejiang Province, China.
Among the HRSV inpatients, 14.1% (1,110/7,857) tested positive for at least one bacterial pathogen. Patients with bacterial coinfections demonstrated a substantially higher incidence of pneumonia compared to those with viral coinfections (73.2% vs. 22.7%). Additionally, the rate of bacterial coinfections was significantly elevated during the 2020–2023 period compared to 2018–2019 (Table 1).
In bacterial coinfection cases, Mycoplasma pneumoniae (M. pneumoniae) emerged as the predominant pathogen, representing 59.2% of all bacterial detections. This was followed by Streptococcus pneumoniae (S. pneumoniae) at 25.3% and Haemophilus influenzae (H. influenzae) at 8.8% (Figure 2).
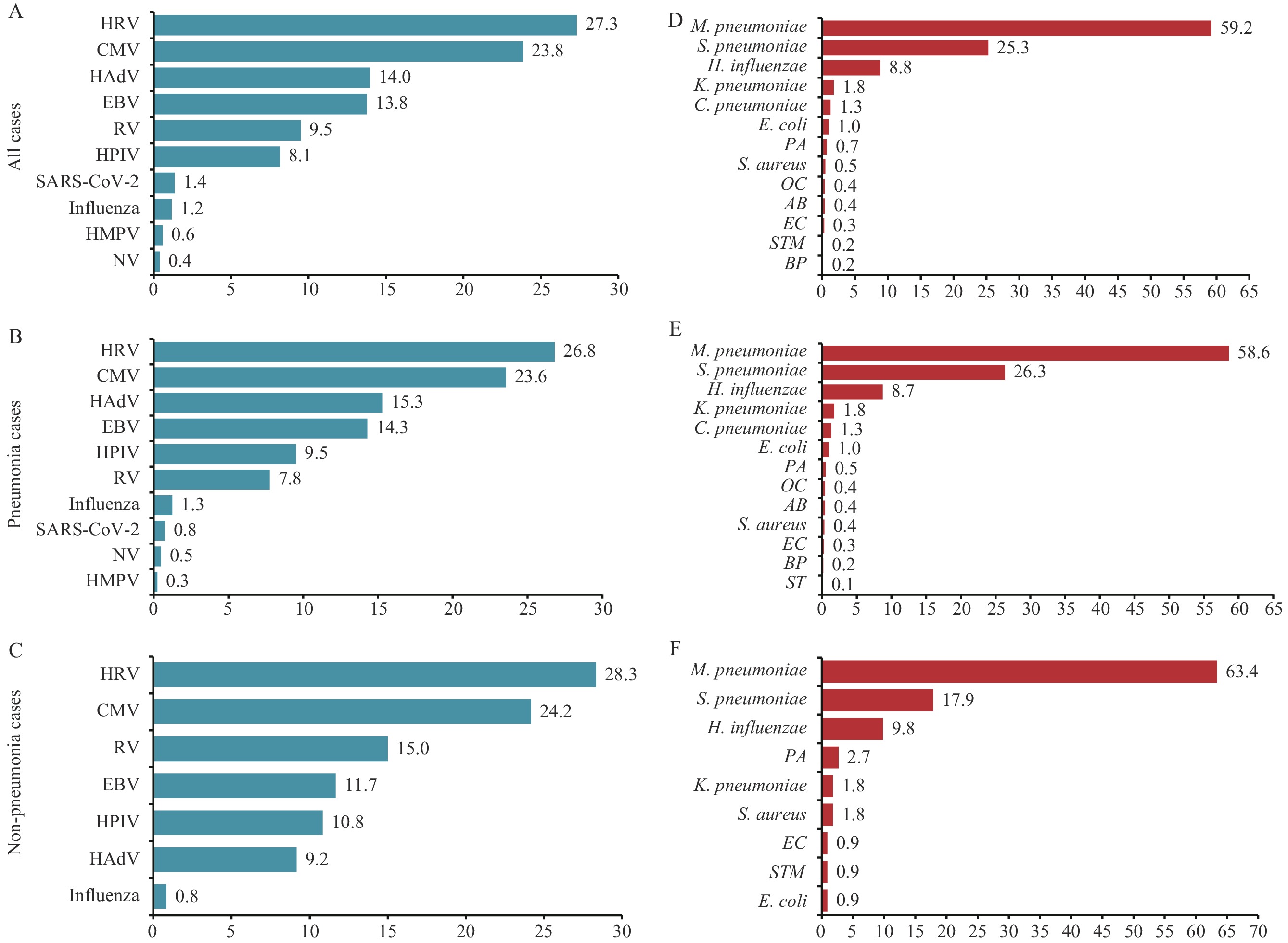 Figure 2.
Figure 2.Viral and bacterial composition of HRSV-positive hospitalized children aged 5 years and younger in Zhejiang Province, China, 2018–2023. (A) Viral composition in all patients; (B) Viral composition in pneumonia cases; (C) Viral composition in non-pneumonia cases; (D) Bacterial composition in all cases; (E) Bacterial composition in pneumonia cases; (F) Bacterial composition in non-pneumonia cases.
Note: Analysis includes all cases tested for ten viral and 13 bacterial pathogens among HRSV-positive hospitalized children. Bar lengths and accompanying numbers represent the proportion of each pathogen, calculated as the number of positive cases divided by the total number of HRSV-positive cases.
Abbreviation: HRV=human rhinovirus; CMV=cytomegalovirus; HAdV=human adenovirus; EBV=Epstein-Barr virus; RV=rotavirus; HPIV=human parainfluenza virus; COVID-19=coronavirus disease 2019; HMPV=human metapneumovirus; NV=norovirus; M. pneumoniae=Mycoplasma pneumoniae; S. pneumoniae=Streptococcus pneumoniae; H. influenzae=Haemophilus influenzae; K. pneumoniae=Klebsiella pneumoniae; C. pneumoniae=Chlamydia pneumoniae; E. coli=Escherichia coli; PA=Pseudomonas aeruginosa; S. aureus=Staphylococcus aureus; OC=oral candidiasis; AB=Acinetobacter baumannii; EC=Enterobacter cloacae; BP=Bordetella pertussis; ST=Salmonella typhi; STM=Salmonella typhimurium.
Among viral coinfections, human rhinovirus (HRV) was the most frequently detected pathogen, accounting for 27.3% of all viral-positive detections, followed by cytomegalovirus (CMV; 23.8%) and human adenovirus (HAdV; 14.0%) (Figure 2).
Analysis of hospitalization expenses revealed that HRSV coinfection cases, whether viral or bacterial, incurred significantly higher costs (median: 4,971.4, IQR: 3,864.7–6,878.0) compared to HRSV monoinfection cases (median: 4,649.1, IQR: 3,486.6–6,524.9, P=0.013). Among all coinfections, CMV was associated with the highest median hospitalization expense (median: 7,243.6, IQR: 5,459.3–9,569.8) (Figure 3).
 Figure 3.
Figure 3.Disease burden in HRSV mono- and co-infections among hospitalized children aged 5 years and younger in Zhejiang Province, China, 2018–2023. (A) Hospitalized expense (HRSV only vs. HRSV coinfection); (B) Hospitalized expense (HRSV coinfections with all viruses vs. single virus); (C) Hospitalized expense (HRSV coinfections with all bacteria vs. single bacteria); (D) Hospitalized days (HRSV only vs. HRSV coinfection); (E) Hospitalized days (HRSV coinfections with all viruses vs. single virus); (F) Hospitalized days (HRSV coinfections with all bacteria vs. single bacteria).
Abbreviation: HRV=human rhinovirus; CMV=cytomegalovirus; HAdV=human adenovirus; M. pneumoniae=Mycoplasma pneumoniae; S. pneumoniae=Streptococcus pneumoniae; H. influenzae=Haemophilus influenzae; CNY=Chinese Yuan.Regarding length of stay, cases with viral or bacterial coinfections demonstrated marginally longer durations (median: 5.0, IQR: 4.0–7.0) compared to HRSV monoinfections (median: 5.0, IQR: 4.0–6.0, P<0.01). Among viral coinfections, CMV cases exhibited significantly extended hospitalization periods (median: 6.0, IQR: 5.0–8.0, P=0.003). In bacterial coinfections, both S. pneumoniae (median: 6.0, IQR: 5.0–7.0, P=0.025) and H. influenzae (median: 6.0, IQR: 5.0–7.0, P=0.018) demonstrated comparable prolonged hospital stays (Figure 3).
HTML
-
This study analyzed surveillance data from 2018 to 2023, encompassing comprehensive pathogen testing data from 8 hospitals in Zhejiang Province for 10 viruses and 13 bacteria in pediatric inpatients under 5 years of age. This analysis revealed significant patterns in the prevalence, pathogen spectrum, and disease burden of HRSV coinfections in this population.
These findings demonstrate a marked increase in HRSV infections during 2020–2023 compared to previous seasons (2018–2019), with a notable shift in age distribution toward older children within the under-5 age group. This pattern suggests that pandemic-related disruptions created increased susceptibility among older children who lacked prior exposure to endemic HRSV (9-10).
The study revealed that HRSV coinfection with other respiratory pathogens was common, affecting 20.4% of all hospitalizations during 2018–2023. Notably, HRSV coinfection rates were substantially higher during 2020–2023 compared to 2018–2019. While the precise mechanism remains unclear, this increase likely relates to both enhanced RT-PCR testing implementation and elevated respiratory pathogen circulation during the COVID-19 pandemic period (11).
Regarding disease status, HRSV coinfections showed significantly higher prevalence in patients with pneumonia compared to those without pneumonia, aligning with Liu et al.’s findings on coinfection patterns in community-acquired pneumonia (12).
This study revealed increased hospital stays and expenses among HRSV coinfections, potentially attributable to the implementation of multiple therapeutic interventions (13–14). These findings underscore the importance of specialized care for hospitalized children with HRSV coinfections. Optimal management should include isolation in separate wards, with particular emphasis on early detection of coinfections through comprehensive testing for HRSV and other common respiratory viruses, especially in infants under 6 months of age.
This study had two primary limitations. First, the analysis of hospitalization expenses excluded indirect costs. Second, selection bias may have occurred as the study included only inpatients with confirmed HRSV infection, excluding those without HRSV detection.
In conclusion, this study demonstrates a significant increase in HRSV coinfections during the COVID-19 pandemic, particularly among patients with pneumonia and those requiring extended hospitalization exceeding 14 days. These coinfections were associated with prolonged hospital stays and elevated healthcare costs. To mitigate future HRSV coinfection incidence and disease burden, public health initiatives should focus on raising awareness among parents and the general public regarding pediatric coinfection risks and prevention strategies. Healthcare providers should implement recommended testing protocols for patients presenting with acute respiratory symptoms to identify HRSV coinfections promptly, potentially reducing infection severity and associated disease burden.
-
The contributions of the local hospitals and prefecture Centers for Disease Control and Prevention in China for their assistance with data collection and field investigations.
| Citation: |

|